Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
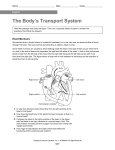
Relation Between Mural Force and Pressure in the Left Ventricle of the Dog By Lloyd L. Hefner, M.D., L. Thomas Sheffield, M.D., Glenn C. Cobbs, B.S., and Willem Klip, M.D., Ph.D. Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 • The study of strips of cardiac muscle has provided much valuable information regarding those factors which determine the force generated during contraction. Interrelationships between force, velocity of shortening, di&stolic stretch, duration of systole, and contractility have been delineated.1"5 These findings are not, however, directly and siiiaply applicable to the physiology of the intact heart because the force generated by the myocardium and the corresponding pressure are by no means synonymous. In order to relate the physiology of muscle strips to that of the intact ventricle, the quantitative relation between force in the wall of the ventricle and pressure in the cavity must be known. The importance of such considerations in cardiac physiology has long been recognized.0"8 The mechanical disadvantage of cardiac enlargement has been frequently cited. Excellent discussions of the problem have been presented by Burch, Ray, and Cronvich,9 Burton,10 and Linzbaeh.11 More recently, Levine and Wagman have discussed the possible influence of the size and shape of the heart on myocardial oxygen consumption, emphasizing the important distinction between the pressure developed by the ventricle and the tension exerted by the fibers.12 An easy wa}' to visualize the simple physics involved in the present experiment is as folFrom the Departments of Medicine and Physiology, University of Alabama Medical Center, Birmingham, Alabama. Supported by American Heart Association grant. Work was done during Dr. Hefner's tenure as an Established Investigator of the American Heart Association and Dr. Sheffield's tenure of a TJ. S. Public Health Service Research Fellowship (HF9775). Received for publication March 30, 1962. 654 lows: Gravitational effects are ignored since they are unimportant in this situation. Consider a static left ventricle of any shape and size containing blood under a given pressure, as in figure 1. Now visualize an imaginary plane through this ventricle as shown in the figure. This imaginary plane divides the ventricle into two parts and passes through a rim of myocardium and a cross-sectional area of the cavity. From elementary hydrostatics it is known that the pressure of the blood in the cavity creates a force in a direction perpendicular to the imaginary plane exactly equal to the product of the pressure (which is force per unit area) times that cross-sectional area of the cavity included in the imaginary plane. The shape of this cross-sectional area of the cavity in our imaginary plane is immaterial, and the size and shape of the rest of the ventricle are also completely without effect on this relation. Since we began by postulating a static ventricle, Newton's laws of motion require that the force mentioned above tending to separate the two parts of the ventricle on each side of the plane be exactly balanced by an equal and opposite force. This equal and opposite force must exist in the rim of myocardium included in the imaginary plane, shown by the stippled area in figure 1. Note that this force exists in the rim of myocardium determined by the imaginary plane, its direction is perpendicular to the plane, and its magnitude is determined only by the pressure and cross-sectional area of the cavity and is independent of the thickness of the wall, the shape or cross-sectional area of the rim, the size or shape of the remainder of the ventricle, the distribution of forces exerted by the individual muscle fibers, the orientation of the various muscle bundles, or the presence of shearing forces. Circulation Research, Volume XI, October 1962 VENTRICULAR FORCE AND PRESSURE Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 The distribution of the forces or stresses within the ventricle wall is of interest and probably is o"f considerable physiological importance, but a consideration of this distribution is much more complicated10'13 than the present approach which is concerned only with the net or resultant force generated by all the fibers of the myocardium included in an imaginary plane through the ventricle. Thus far, we have considered a static ventricle. When the ventricle ejects blood, the force exerted by the rim of myocardium included in the imaginary plane slightly exceeds the opposing force represented by the product of the pressure and the cross-sectional area of the cavity. This slight excess of force is necessary to accelerate the ventricular wall. For all practical purposes we may ignore this minor discrepancy. It is possible to estimate the additional force necessary for ejection, and it has been found that the discrepancy under the most extreme circumstances will be less than 2 per cent. We may say, therefore, that the product of the pressure and the cross-sectional area of the cavity gives a close estimate of the net force perpendicular to the plane generated by a complete rim of the myocardium, as illustrated in figure 1. This conclusion seems obvious but has not previously been verified experimentally, nor has the time course of mural force ever been recorded. An experimental approach to the problem requires a method for measuring the longitudinal force developed by the myocardial fibers. To measure directly the force exerted by a muscle fiber, one must insert a force gauge in series with the fiber. The following method is based on this principle: A slit is made in the wall of the dog left ventricle, and the two edges of the slit are held together by a stiff gauge which allows a record to be made of the force developed by the cut fibers. This setup is tantamount to sampling the force perpendicular to the imaginary plane discussed above. Methods la five consecutive dogs, after induction of pentobarbital anesthesia, 10 to 12 mg./Kg. given slowly intravenously, and institution of positive Circulation Research, Volume XI, October 1962 655 IMAGINARY PLANE CAVITY ENDOCARDIUM EPICARD1UM FIGURE 1 Diagram illustrating an imaginary plane through a left ventricle. The plane divides the ventricle into tioo parts and passes through a rim of myocardium and a cross-sectional area of the cavity. The pressure in the cavity times the crosssectional area of the cavity is the net force perpendicular to the imaginary plane which, if unopposed by an equal and opposite net force in the rim of myocardium included in the plane, would cause the two parts of the ventricle to separate. pressure artificial respiration, a left thoracotomy was performed, the pericardium incised, and the cut edges sutured to the chest wall to provide a cradle for the heart. Aortic and ventricular pressure, the outer circumference of the left ventricle, the electrocardiogram, and the force required to hold together the two edges of a slit in the ventricle were all recorded simultaneously. Left ventricular pressure was measured by a Statham P-23d strain gauge manometer connected to a short, wide-bore, plastic eannula inserted into the ventricle through the apex, and aortic pressure was obtained from a similar transducer connected to a copper eannula inserted into the ascending aorta through a carotid artery. The outer circumference of the left ventricle was measured by a variable resistance gauge described by Rushmer.14 This gauge consists of a rubber tube, about 1 mm. in outside diameter, filled with mercury. The electrical resistance of the mercury column varies directly with its length and is recorded through a strain gauge carrier amplifier. The gauge itself encircles the greatest diameter of the left ventricle parallel to the atrioventricular groove, being threaded through the thin wall of the right ventricle just to the right of the septum, as illustrated in figure 2. The gauge was applied so that it was under tension even at the smallest ventricular size obtained, ensuring that the gauge HEFNER, SHEFFIELD, COBBS, KLIP 656 CIRCUMFERENCE GAUGE FORCE GAUGE SLIT Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 LAMIMTCI ICSIjrtNCE STKUU 6AUCC tUMUTi SVTUKES FORCE GAUGE HIT c FIGURE 2 (A) Diagram of the positions of the circumference gauge and the force gauge on the anterior surface of the left ventricle. In one of the five dogs, the orientation of the slit was perpendicular to that shown. (B) Diagrammatic cross-section of the force gauge sutured to the myocardium with a slit between the legs. The gauge records the force needed to prevent the two edges of the slit from separating. (C) Dimensional view of the force gauge. was well coupled to the ventricular wall and that it operated only in its linear range. This latter factor was verified after each experiment. The characteristics, including the frequency response, of this gauge have been studied thoroughly by Lawton and Collins.15 The amplitude response to increasing frequency is flat to beyond 30 cycles per second. The force required to hold together the two edges of a slit in the ventricle was measured as follows: A gauge was constructed of spring steel, as illustrated in figure 2, upon which were bonded two foil strain gauges for recording the force applied to the legs. The dimensions of the gauge are indicated in figure 2. The gauge weighs 600 ing., is linear from 0 to 100 Gin., has a natural frequency over 100 c.p.s., and at the maximum force encountered in these experiments yielded only 0.4 mm. The two legs were pressed onto an ink pad and then touched to the surface of the left ventricle in an area with no visible coronary arteries, leaving two marks for accurate placement of sutures, allowing precise approximation of the edges of the slit as described below. Two deep sutures were placed on these marks and the gauge tied firmly in place. Then between the two legs of the gauge a slit was made, extending deeper than the sutures. The length of the slit exceeded the width of the gauge by a few millimeters on each side. The depth of the slit extended Circulation Research, Volume XI, October 1962 657 VENTRICULAR FORCE AND PRESSURE Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 through approximately two-thirds the thickness of the ventricular wall. These procedures assured that no uncut fibers remained between the two sutures attached to the gauge. The gauge held the two edges of the slit together and recorded the force. The function of the ventricle as a whole was not detectably disturbed by the presence of the slit, the edges of which were, in effect, sutured back together by the attachment of the gauge. In an ideal experiment the slit would be oriented so as to be parallel to the circumference gauge, as consideration of figure 1 makes clear, but in most of our experiments the slit was actually made almost perpendicular to this gauge, as illustrated in figure 2. This placement was necessary to avoid injury to major branches of the coronary artery. The implications of the orientation of the slit are discussed below. After the gauges were in place, all measurements were recorded simultaneously on an eight-channel oseilloscopie recorder.* Records were made as the dogs were given, stepwise, 15 or more 100-cc. transfusions until the ventricle was grossly distended. Records obtained at the natural heart rate were alternated with records obtained at a slow, constant heart rate by electrical stimulation of the cut peripheral end of the vagus with simultaneous electrical pacing of the heart. These procedures furnished a wide range of pressure, force, and size for analysis in each dog. Identical procedures were carried out in each of five consecutive dogs. At the end of each experiment the circumference gauge was removed and calibrated. The force gauge was calibrated by using known weights. In postmortem study the left ventricle was transected parallel to the circumference gauge, and the circumference and average wall thickness were measured as accurately as possible. Figure 3 shows the type of records obtained. Simultaneous values for pressure, outer circumference, and force across the slit were determined at 0.02-second intervals during ejection systole for one beat from each record made on each clog. Thus, many hundreds of measurements from each of the five dogs were analyzed with a wide range of pressure, force, size, and stroke volume. For each measured value for the outer circumference, an approximate value for the inner radius was calculated as follows: By assuming the ventricle to be a thick-walled sphere, the volume of muscle is calculated from the measurements of wall thickness and outer circumference made at postmortem study. Since the total volume of the ventricle is equal to the sum of the volume of blood in the cavity and the volume of the muscle, •Electronics for Medicine, Inc., White Plains, Xew York. Circulation Research, Volume XI, October 1962 FIGURE 3 Typical records obtained from dog 1. Figure 3A is a record made ivhile the ventricle xoas small, and figure 3B xoas made after transfusion of 2 L. of blood. Note that changes in pressure were not proportional to changes in force and that the force declined during most of ejection systole. Left ventricular pressure (P); left ventricular circumference (C); force across the slit in the wall of the left ventricle (F). one solves the corresponding equation for the inner radius and obtains 3K where A1 is the inner radius, C the outer circumference, and K the volume of the muscle (a constant for each dog). The accuracy of the calculation is determined by the extent to which the dog left ventricle is a thick-walled sphere. That the approximation is close enough to be useful is evidenced by the correlations presented below. Results In figure 3 are typical records obtained from dog 1. Figure 3A was recorded while the ventricle was small, and figure 3B after transfusion of 2 L. of blood. The time course of force in the slit is of special interest. Note that (1) the force in the slit rises rapidly during pre-ejection systole but with or shortlj7 after the onset of ejection ceases to rise and then falls; this fall is more marked in figure 3B where the stroke volume is larger. (2) The 658 HEFNER, SHEFFIELD, COBBS, KLIP •_ DOG «2 DOG f • • • » 4 ••V • • • • tn f O ' U . or O LU "'. > » " » i •• i •) » •'. 'A± " -5' •'• cr O •% R= .875 .%** 20 x ' R= 618 * ' • • Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 20 40 30 PRESSURE - GMS / C M eo :"* . " °- ' • 40 50 60 PRESSURE 70 140 «, DOG " 3 • . 130 eo DOG #4 120 .} 110 •'• 100 " / • * 90 • U U 60 u cc O cr 60 50 40 23 35 45 33 65 75 BS 9$ PRESSURE 105 40 145 123 SO 60 70 80 90 WO MO 120 130 MO PRESSURE FIGURE 4 The relation between force (ordinate) and pressure (abscissa) in four of the five dogs. The units are arbitrary except in dog 1, since the absolute value for the force depends on the size of the slit, which was not the same in all dogs. All measured points for these four dogs are shown. Dog 5 is not shown, being very similar to dog 2, with a correlation coefficient of 0.618. The relatively large scatter seen in this figure indicates that a pressure measurement alone is not a good index to the force developed by the myocardium. time course of force and the time course of pressure differ markedly in contour, pressure rising at the same time force is falling during much of ejection systole. (3) Comparing figure 3B with figure 3A. shows that the force has increased proportionately more than the pressure. Similar findings were predicted in the paper by Bureh, Ray, and Cronvich.9 Linzbach11 calculated that the force would be lower at the end of ejection than at the beginning, as is actually seen in figure 3. This is not invariably true, however, for when the stroke volume is small, no decline or even a slight increase in tension may occur. Figure 4 shows the relationship between force in the wall and ventricular pressure for Circulation Retearch, Volume XI. October 196t VENTRICULAR FORCE AND PRESSURE Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 four of five dogs separately. The correlation coefficients range from 0.618 to 0.936. There is considerable scatter, so that for any given ventricular pressure the corresponding force may vary within wide limits. If onlj- those points where the size of the ventricle is a constant value are selected for graphing, an excellent correlation between pressure and force in the wall is obtained, as shown in figure 5. This graph was obtained by plotting from dog 1 (fig. 4) all those points where the ventricular circumference was 190 mm. and therefore represented measurements near the onset of ejection when the end-diastolic size was small and those points near the end of ejection when the end-diastolic size was large. The high degree of correlation is evidence that the primary reason for the scatter observed in figure 4 is the varying size of the ventricle. The precision of the relationship between pressure and force seen in figure 5 affords a strong indication of the validity of the method for measuring force. Figure 6 shows for the same four dogs the results of comparing the force across the slit against the product of pressure and the square of the inner radius. The inner radius is squared because we want to multiply the pressure by a number proportional to the area of the cavity cut by the plane. The lengthmeter is oriented so that the cavity has a nearly circular cross-section in this particular plane, and the square of the inner radius gives a number proportional to this area. As compared to figure 4, the improvement in the correlation is obvious, the correlation coefficients ranging between 0.913 and 0.978. All measured points for four dogs are plotted both in this graph and in figure 4. Dog 5 is not graphed in either figure 4 or figure 6, since the results were very similar to dog 2. The correlation coefficient for dog 4 was 0.618 for force versus pressure and 0.913 for force versus the product of pressure and the square of the inner radius. In figure 7 a single beat from dog 1 is analyzed. In the top graph, force across the slit is plotted against the pressure. This graph shows that for any given pressure, force can Circulation Research, Volume XI, October 19G2 659 DOG # 1 in ? 45 mm ftugm • "5 "80 90 I0O 110 120 130 140 150 160 170 ISO PRESSURE-GMS/CM2 FIGURE 5 The relation in dog 1 between force and pressure if the size of the ventricle is not a variable. From dog 1 all points home been selected for graphing where the circumference of the ventricle icas 190 mm. The points graphed, therefore, represent measurements made at various times during ejection—near the onset of ejection when the enddiastolic size was small and near the end of ejection when the end-diastolic size was large. have more than one value. The middle graph shows the relation in the same beat between force and the product of the pressure and the square of the outer circumference (use of the outer radius in place of the outer circumference does not change the shape of the graph since the radius is proportional to the circumference). Again, the force is shown to be no function of the product of the pressure and the square of the outer circumference or radius. On the other hand, the bottom graph shows that force is a linear function of the product of the pressure and the square of the inner radius. Discussion The force records in figure 3 are of particular interest since they represent a basic physiological measurement not previously available. They are directly comparable to force or tension curves obtained from muscle strip preparations, with the advantage that the 660 HEFNER, SHEFFIELD, COBBS, KLIP 40 •yfi00 IS I' DOG* 2 D06 «1 30 40 Id 20 iri O tr R-.978 '"*"*• """'V Ul R=.9I6 U 10 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 10 • « . • 0 100 20 8 Or 140 i ISO PA2 -Gms.x 10"' . i i 5" " * i 70 90 PA 2 300 ZZO 130 ISO 140 130 DOG # 4 DOG " 3 120 * MO SO 4• Id x 100 X "x X x x X x X O x X X > 90 OC * 0 • O u. x ** >Xx * $ x JT* x o or eo O 30 ' x x *x FU.954 "- i*' 70 60 50 40 re 30 ^ >^ kx* x SO 70 90 110 IJO ISO 170 : x R = .92l ^ X ISO 200 2 » 300 350 400 450 500 550 600 650 700 190 PA 2 FIGURE 6 For each of the four dogs, force (ordinate) icas plotted against the product of the pressure and the square of the inner radius. All points seen in figure 4 are also represented on these graphs. The improvement in the correlation is evident. The units assigned are arbitrary except in dog 1. Bog 5 is not shown, being similar to dog 2, with a correlation coefficient of 0.936. muscle remains in its natural environment but the disadvantage that the size of the sample is not readily determined. Figure 3 shows the typical contour of the force curve. It is perfectly compatible with what one would expect on the basis of known facts of muscle physiology. Thus, if a strip of cardiac muscle contracts isometrically, the tension curve has a rounded summit, but if shortening occurs at any stage during the contraction, the tension (or force) developed is less than in an isometric contraction. In the force curves in figure 3, the rise in force ceases abruptly soon after shortening (ejection) begins, and in most records the force declines during the remainder of systole. If ejection Circulation Research, Volume XI, October 1962 661 VENTRICULAR FORCE AND PRESSURE Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 had not occurred, the familiar rounded summit of an isometric contraction could be expected. Figure 8 demonstrates this fact, showing a record made during ventricular bigeminy, where the premature beat failed to open the aortic valve. In the isometric beats the summit of the force curve was rounded, whereas, in the beats in which ejection occurred, an abrupt fall in tension is seen. The fall in force development is due to two simultaneously operating influences—the amount of shortening and the rate of shortening.1"3 Such details of the contour of the force record provide evidence of the validity of the method of measuring force, since the contour is consistent with that predicted from known facts. The correlations seen in figure 6 are a measure of the success of this study in establishing that the total force generated by the muscle perpendicular to an imaginary plane through the ventricle is determined by the product of the pressure and the cross-sectional area of the cavity in the same plane. The significance of the good correlations is enhanced by considering that our measurement of the cross-sectional area is indirect and is only an approximation for a nonspherical ventricle. Furthermore, the orientation of the slit in this study was determined principally by the direction of the coronary arteries, so that'the most appropriate orientation of the slit, namely, parallel to the circumference gauge, was achieved only once (in dog 5). It follows from the presentation in the introduction that for a nonspherical ventricle two different orientations of the slit, determining two different cross-sections of the cavity, would give force records which were proportional to one another only if the variations of the two crosssectional areas of the cavity were also proportional. We believe these difficulties make the correlation seen in figure 6 more significant. Theoretical considerations and figure 7 both show that net force in the wall and pressure are related to one another through the dimensions of the cavity of the ventricle, not through the external dimensions of the venCirculation Research, Volume XI, October 19C2 ro eo DOG «1 " -• -\ so «o . . j - * " • " • « • — " ' " " * " ...» cr £30 < - - 100 110 PRESSURE DOG PC2 DOG # 1 PA 2 FIGURE 7 Analysis of a single beat from dog 1. Measurements were made every 0.02 second during ejection. The upper two graphs show that the force is not a function of either the pressure alone or of the product of the pressure and the square of the outer circumference (or outer radius). The loiver graph shows the force to be proportional to the product of the pressure and the square of the inner radius. Product of the pressure and the square of the outer radius (PC2); the graph would not be changed in shape if outer radius had been used instead of outer circumference. Product of the pressure and the square of the inner radius (PA'). tricle. A given small change in the outer dimensions of the heart may correspond to a much greater change in the dimensions of the HEFNER, SHEFFIELD, COBBS, KLIP 662 Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 FIGURE 8 A record made during ventricular bigeminy in dog 4. The second beat is premature with little or no ejection occurring; as evidenced by the aortic pressure pulse and the circumference record. Note that the force curve is roughly sinusoidal in the second beat but quite different in the first beat. The maximum force developed in the premature beat actually exceeds that developed in the normal beat, although the pressure developed is much less. Circumference (C); force (F); left ventricular pressure (P). At represents the inner radius and Ae the outer radius of a thick-walled sphere if the volume of the wall is constant. The graph shows that the inner radius changes more rapidly than the outer radius, especially at small sizes, as the size of the sphere increases. The horizontal distance between the solid and the dotted lines represents the thickness of the wall. cavity. Figure 9 illustrates this point. For a thick-walled sphere the inner radius is plotted on the ordinate and the outer radius on the abscissa. The slope of the graph varies from infinity (when the inner radius is zero) to one (at large ventricular sizes). Therefore, when the ventricle is small, the inner radius changes much more rapidly than the outer radius. The principle is still valid for a nonspherical ventricle. The clinical implications of this principle are obvious: Small increases in the external dimensions of the heart can greatly increase the force which the muscle fibers must develop in order to generate a given ventricular pressure. It was pointed out earlier that the virtual identity between net force in the wall and the product of intracavitary pressure and crosssectional area is not influenced by such factors as the shape of either the cavity (the area is important, not the shape) or the rim of myocardium, fiber direction, shearing forces, or any other consideration one can suggest. Such factors are very important, however, in determining the distribution of forces in the rim of myocardium. This important problem we cannot evaluate because of the simplicity of the mathematics used and because the method of force measurement gives only the net force pulling the two edges of the slit apart and provides no information about the distribution of stresses in the sample. It is very likely, though, that the sample of the myocardium measured in this way is a representative sample, meaning that the force recorded across the slit is a constant fraction of the total force perpendicular to the plane of the slit generated by all the fibers of the ventricle in the imaginary plane determined by the slit. The chief evidence for this conclusion is as follows: (1) the previously cited excellence of the correlation between pressure (which results from the action of all the fibers) and the force recorded across the slit, so long as the ventricular size is a constant, shown graphically in figure 4; (2) the size FIGURE 9 Circulation Research, Volume XI, October 1962 663 VENTRICULAR FORCE AND PRESSURE of the sample is a considerable fraction, about 1/20, of all the fibers that would be included in a complete transection of the ventricle. Summary Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 An investigation of the relationship in the dog between left ventricular pressure, left ventricular size, and total longitudinal force developed by the wall of the left ventricle is reported. This study required the development of a method for recording the force needed to keep together the two edges of a slit in the ventricle. Such a method is described, and samples of the force curves are shown, the general features of which are consistent with predictions from the physiology of muscle strips. The net force which the muscle fibers develop perpendicular to a given plane through the ventricle is almost identical to the product of the intracavitary pressure and the area of the cavity included in the plane. This relationship holds true regardless of the thickness of the wall or the shape of the ventricle. References 3. HILL, A. V.: Heat of shortening and dynamic constants of muscle. Proc. Boy. Soc, London 126: 136, 1939. 4. PODOLSKY, B. J.: Mechanism of muscular eontraction. Am. J. Med. 30: 70S, 1961. 5. SONNENBLICK, E . H . , AND McCOLLUM, Z. T. : Active state, force-velocity relationships, and inotropic mechanisms in mammalian papillary muscle. Fed. Proc. 20: 26, 1961. 6. WOODS, E. H.: Few applications of physical theorem to membranes in human body in state of tension. J. Anat. & Physiol. 26: 362, 1892. 7. WOLF, A. V.: Demonstration concerning pressuretension relations in various organs. Science 115: 243, 1952. 8. EUSHMER, E. F . : Cardiac Diagnosis: Physiologic Approach. Philadelphia, W. B. Saunders Co., 1955, p. 105. 9. BTJRCH, G. E., EAT, C. T., AND CRONVICH, J. A.: Certain mechanical peculiarities of human cardiac pump in normal and diseased states. Circulation 5: 504, 1952. 10. BURTON, A. C.: Importance of shape and size of heart. Am. Heart J. 54: 801, 1957. 11. LrNZBACH, A. J.: Heart failure from point of view of quantitative anatomy. Am. J. Cardiol. 5: 370, 1960. 12. LEVINE, H. J., AND WAGMAN, E. J.: Energetics of human heart. Am. J. Cardiol. 9: 372, 1962. 1. ABBOTT, B. C, AND MOMMAERTS, W. F. H. M.: Study of inotropic mechanisms in papillary muscle preparation. J. Gen. Physiol. 42: 533, 1959. 2. ABBOTT, B. C, AND WILKIE, D. B.: Eelation between velocity of shortening and tension length curve of skeletal muscle. J. Physiol. 120: 214, $ 13. SANDLER, H., DODGE, H., AND HAY, E.: 15. LAWTON, E. W., AND COLLINS, C. C.: Calibration of aortic circumference Physiol. 14: 465, 1959. gauge. J. Erratum Vol. X, pages 741 and 743, Intereoronnry Reflex. Demonstration by Coronary Angiography, Santiago V. Guzman et al.: illustrations for figures 2 and 4 should he reversed. Circulation RetearcjA Volume XI, October 1961 Left ventricular tension and stress in man. Clin. Ees. 9: 145, 1961. 14. EUSHMER, E. F.: Heart size and stroke volume. Minnesota Med. 37: 19, 1954. Appl. Relation Between Mural Force and Pressure in the Left Ventricle of the Dog Lloyd L. Hefner, L. Thomas Sheffield, Glenn C. Cobbs and Willem Klip Downloaded from http://circres.ahajournals.org/ by guest on June 15, 2017 Circ Res. 1962;11:654-663 doi: 10.1161/01.RES.11.4.654 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1962 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/11/4/654 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/