Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
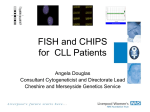
AD_ 0 2 9 _ _ _ APR0 8 _ 1 1 . p d f Pa ge 2 9 3 1 / 3 / 1 1 , 1 1 : 2 6 AM HowtoTreat PULL-OUT SECTION www.australiandoctor.com.au COMPLETE HOW TO TREAT QUIZZES ONLINE (www.australiandoctor.com.au/cpd) to earn CPD or PDP points. inside Chronic lymphocytic leukaemia Follicular lymphoma Managing patients receiving chemotherapy The authors DR SARAH KAMEL, advanced trainee in clinical and laboratory haematology, division of cancer medicine, Peter MacCallum Cancer Centre, East Melbourne, Victoria. Lymphoproliferative disorders Part 2 — Chronic lymphocytic leukaemia and follicular lymphoma Last week, Part 1 of this two-part series discussed the most common of the aggressive types of lymphoma. This week, Part 2 focuses on two of the indolent lymphoproliferative diseases — chronic lymphocytic leukaemia and follicular lymphoma. We discuss diagnosis and management for these conditions, after patients have been referred to a haematologist. The outlook for these malignancies today is also reviewed. PROFESSOR JOHN F SEYMOUR, consultant haematologist, head of haematology department, division of cancer medicine, Peter MacCallum Cancer Centre, East Melbourne, Victoria. PROFESSOR H MILES PRINCE, consultant haematologist, division of cancer medicine, Peter MacCallum Cancer Centre, East Melbourne, and Cabrini Hospital, Malvern, Victoria. Background THE lymphoproliferative diseases are a heterogeneous group of haematological disorders characterised by malignant clonal proliferation of cells derived from their ‘normal’ lymphoid counterparts. They are classified according to distinct clinicopathological features. This group of disorders is distinct from myeloid disorders, which are malignancies that derive from cells destined to form neutrophils, monocytes, etc. (eg, chronic myeloid leukaemia, myeloproliferative diseases and myelodysplasia) (figure 1, page 30.). The lymphoproliferative diseases comprise the lymphomas and the chronic lymphoid leukaemias. The latest edition of the WHO Classifiwww.australiandoctor.com.au cation of Tumours of Haematopoietic and Lymphoid Tissues lists more than 40 different types of nonHodgkin lymphoma (NHL). These can broadly be divided into B- and T-cell disorders and further subdivided into clinically aggressive ‘high-grade’ and clinically indolent ‘low-grade’ malignancies. cont’d next page 8 April 2011 | Australian Doctor | 29 AD_ 0 3 0 _ _ _ APR0 8 _ 1 1 . p d f Pa ge 3 0 3 1 / 3 / 1 1 , 1 1 : 2 7 AM HOW TO TREAT Lymphoproliferative disorders — Part 2 from previous page Figure 1: Ontogeny of haematopoietic cells. The two most common indolent lymphoproliferative diseases are chronic lymphocytic leukaemia (CLL) and follicular lymphoma (FL), both of B-cell origin. Included with the term ‘CLL’ is small lymphocytic lymphoma (SLL), which is essentially a lymphomatous presentation of CLL. First, to clarify a few terms, low-grade implies a slow-growing indolent tumour. Both CLL and FL are in this category. However, both may (albeit unusually) transform into a more aggressive lymphoma. In the case of CLL this is referred to as a Richter’s transformation. Once this occurs, the prognosis for these patients is much bleaker than for de novo aggressive lymphomas such as those discussed in Part 1, and cure is not attainable with currently B cells Common lymphoid progenitor cell T cells LPDs originate from B or T cells NK (natural killer) cells Pluripotent stem cell Neutrophilis Common myeloid progenitor cell Myeloblast Monocytes Eosinophils Platelets Red cells Basophils LPD = lymphoproliferative disease available therapies. Broadly speaking, indolent lymphoproliferative diseases can grumble on for years, even for more than a decade in some patients. In many cases they can be observed for a period of time before therapy is required. The flipside of their indolent nature is that they are generally incurable, although in selected patients, an allogeneic bone marrow transplant may offer the hope of a cure. Similarly, localised FL is curable with radiotherapy. When discussing FL, we focus be on disseminated disease, as this is by far the more common presentation. Epidemiology Many of you will have been involved in the care of lymphoma patients in your practice. According to Australian Institute of Health and Welfare data for 2005, lymphomas were the fifth most commonly diagnosed group of cancers in both men and women. This translates to 4400 new cases of lymphoma, or an incidence of 21/100,000 Australians per year, which equates to just over 4% of all cancer diagnoses. Of these cases, CLL/SLL and FL were each diagnosed in almost 1000 Australians in 2005, with incidences of 4.5 and 4.3 cases/100,000 people, respectively. For CLL the incidence climbs steeply in people over 65, with 2230/100,000 people in this age group diagnosed each year with the disease. By comparison, prostate cancer comprised 16.3% of all cancers, with an annual incidence in men of 164/100,000. Breast cancer made up 12.2% of new cancers and was diagnosed in 111/100,000 women. Other frequently diagnosed malignancies such lung cancer and colorectal cancer comprised 9.1% and 13% of all cancer diagnoses, respectively. Chronic lymphocytic leukaemia CLL is the most common type of leukaemia in Western societies and is less common in people of Asian descent. It is characterised by the protracted but progressive accumulation of small, relatively slow-growing lymphocytes. The median age at diagnosis is 70. Figure 2: A ‘smear’ or ‘smudge’ cell seen in patients with chronic lymphocytic lymphoma (CLL). These cells are fragile and are damaged in the process of blood slide preparation. The presence of these cells should alert the treating doctor that CLL is a possible diagnosis. They may be present even when the absolute lymphocyte count is normal. Flow cytometry Prognosis Median patient survival is 10 years. However, this number does not take into account the heterogeneity seen in the CLL patient population. Many patients will have a very indolent course and ultimately succumb to an illness other than their CLL, while a small proportion of patients will have aggressive disease and live only 1-2 years from diagnosis. Apart from initial staging of the disease, a variety of prognostic markers has been recognised that aid in riskstratifying patients and guiding clinicians as to who is likely to require treatment and when. Two intact CLL cells A smear cell Presentation Many laboratories with a large referral base of GPs will often encounter routine FBCs as part of annual health checks that show a mild lymphocytosis (5-10 × 109 cells/L), but are otherwise unremarkable. In most cases, this lymphocytosis is reactive and thus transient (see box, right, for causes of lymphocytosis). Lymphocyte counts >15 × 109 cells/L are more concerning. Many GPs will prudently repeat the FBC in a few weeks or months and in a minority of cases the lymphocytosis will be persistent. It is essential to assess the patient clinically for lymphadenopathy and splenomegaly. With regard to their blood tests, the presence of an anaemia or thromboycytopenia is more suggestive of underlying malignancy. If 30 | Australian Doctor | 8 April 2011 ther characterise the cell population in question. The request slip should state as much clinical information as possible and stipulate that CLL/NHL is being considered. any of these clinical or laboratory features are present, further investigations should be pursued. Rarely, patients can present with a lymphocyte count of >50 × 10 9 cells/L. This magnitude of lymphocytosis is almost always malignant. A good laboratory will always make an urgent blood film and review the lymphocyte morphology in addition to performing further tests, if required, to exclude an acute leukaemia. Diagnosis A peripheral blood film should be examined by a laboratory haematologist to look for abnormal lymphocytes. CLL cells classically look like small mature lymphocytes. Due to their fragility, the cell membrane can easily tear when a drop of blood is smeared across a glass slide. This results in the laboratory artefact of a ‘smear’ or ‘smudge’ cell (figure 2). Morphology is generally not sufficient to define the malignant nature of the cells or that the lymphoproliferative disease is CLL and not another disorder (such as mantle-cell or marginal-zone lymphoma, T-cell or natural killer (NK) cell proliferations). If CLL is suspected based either on a persistent lymphocytosis, abnormal lymphoid morphology or presence of lymphadenopathy or splenomegaly, flow cytometry of the peripheral blood should be performed to fur- www.australiandoctor.com.au Flow cytometry, also known as ‘cell surface markers’, has a rapid turnaround time and can definitively establish the presence of an abnormal population of cells in the peripheral blood, bone marrow, excised lymph nodes and even CSF or pleural fluid. The principle of flow cytometry is to measure the light-scatter characteristics of a stream of cells in single file, which run past a laser (figure 3, see page 32). Additionally, the light emission of fluorescent markers (fluorochromes) tagged to antibodies that attach to various cluster-of-differentiation (CD) cell surface markers is characterised (figure 4, see page 32). All haematopoietic cells express CD markers, which perform different cellular functions. Different cell types have their own typical pattern of normal CD expression — a ‘phenotype’. Malignant lymphocytes express an aberrant lymphocyte phenotype. For example, all B cells are CD19 positive (CD19+) and this includes CLL cells. What defines the CLL cells as abnormal is they are also CD5+, whereas normal B cells are CD5-. The classic phenotype of CLL cells is CD19+ CD5+ CD10-, with either lambda or kappa light chain restriction. The term light chain restriction implies that all cells in a given population express the same light chain type (ie, kappa or lambda) because they are clonal. Flow cytometry is invaluable not only for the diagcont’d page 32 Differential diagnosis of a lymphocytosis (other than a lymphoproliferative disease) • Viral infection (eg, influenza, Epstein–Barr virus (EBV), cytomegalovirus (CMV), HIV, toxoplasmosis • Stress-related lymphocytosis (during an MI, post-trauma) • Some bacterial infections (eg, pertussis, brucellosis, tuberculosis) • Post-splenectomy • Allergic reaction to a medication • Post-seizure AD_ 0 3 2 _ _ _ APR0 8 _ 1 1 . p d f Pa ge 3 2 3 1 / 3 / 1 1 , 1 1 : 2 8 AM HOW TO TREAT Lymphoproliferative disorders — Part 2 from page 30 Figure 3: Schematic of a flow cytometer. nosis of haematological malignancies but also for detecting minimal residual disease (MRD) post-therapy with a sensitivity of up to 1/10,000 abnormal cells in some laboratories. Additionally, markers of poor prognosis, such as CD38 and ZAP-70 expression in CLL can also be identified. Figure 4: CD19+ cell tagged by a fluorochrome. Fluorochrome conjugated to antiCD19 antibody Single file of cells in sheath fluid CD19 Detector Monoclonal B lymphocytosis It should be noted that the presence of cells in the peripheral blood with a ‘CLL phenotype’ is not enough to diagnose CLL. If the total abnormal lymphocyte population is <5 × 109 cells/L and there is no evidence of lymphadenopathy or organomegaly, the patient is considered to have a ‘monoclonal B lymphocytosis’, which is essentially preCLL. This pattern occurs in at least 3% of people aged 60-80 years. The International Workshop on Chronic Lymphocytic Leukaemia (IWCLL) guidelines state that to diagnose CLL there must be an absolute peripheral blood lymphocytosis (of phenotypically abnormal cells) of >5 × 109 cells/L. This lymphocytosis must be present for at least three months. The progression of monoclonal B lymphcytosis to frank CLL is at the rate of 12% of patients per annum, and these patients typically have very indolent disease, with only about 15% ever requiring therapy. In general they should be monitored on an annual basis. Light scatter comprised of forward and side scatter Detector Fluorescent emission Laser strikes cell After a patient has been diagnosed with CLL, the first thing to decide is how extensively they need to be investigated. marrow involvement is so extensive that normal haematopoiesis is compromised and the patient develops cytopenias — anaemia (stage III) and thrombocytopenia (stage IV). Table 1, adapted from the original 1975 article by Rai, describes each stage of disease. With the increasing utilisation of blood tests in the community, up to 60% of patients may present with isolated lymphocytosis. Prognostic markers Small lymphocytic lymphoma SLL is considered biologically the same disease as CLL and is treated in the same way. Patients diagnosed with SLL have lymphadenopathy and/or splenomegaly but lack the peripheral blood lymphocytosis of >5 × 109 cells/L that is required for a diagnosis of CLL. The different presentation of what is essentially the same disease may be due to different expression of adhesion proteins that result in SLL manifesting in a more lymphomatous rather than leukaemic form. Staging Who should be investigated? After a patient has been diagnosed with CLL, the first thing to decide is how extensively they need to be investigated. It is our practice to address this issue by first asking how will this alter management. In other words, if the patient is over 60 and asymptomatic, a ‘watch and wait’ approach is appropriate. In almost all cases, specialist referral should be sought, as patient investigation and management needs to be individualised. Before referring a patient it is helpful to order a Coombs 32 | Australian Doctor | 8 April 2011 test (to assess for autoimmune haemolysis). Baseline immunoglobulin levels are helpful to assess the degree of underlying immunosuppression. In early-stage CLL we recommend three-monthly reviews in the first year primarily to assess the tempo of disease. The peripheral blood lymphocyte doubling time (the time for the baseline lymphocyte count to double) is one of the most useful prognostic measures, as doubling in less than six months confers a poor prognosis. Conversely, if the patient clearly needs treatment in the foreseeable future (eg, cytopenias, lymphadenopathy, organomegaly or constitutional symptoms are present), immediate staging will help ‘prognosticate’ for that patient. The staging approach described below applies to such patients. Staging investigations Generally, if therapy is being considered in patients with cytopenias, a bone marrow biopsy is performed. This will distinguish between cytopenias caused by marrow infiltration by CLL and autoimmune cytopenias, which are seen in about 7% of patients with CLL. In the presence of an autoimmune cytopenia there will be robust marrow production of the affected cell lineage, indicating that there is peripheral destruction of cells. An autoimmune cytopenia does not ‘upstage’ the disease and the presence of autoimmune cytopenias does not confer a worse overall survival. A bone marrow biopsy will also help with prognostication, as the extent of marrow infiltrate and cytogenetic abnormalities influence prognosis. Most patients will also have CT to assess for the presence of lymphadenopathy, splenomegaly and hepatomegaly. About onequarter of patients with no clinically detectable lymphadenopathy have occult abdominal lymphadenopa- www.australiandoctor.com.au thy on CT, which has been shown to confer a worse prognosis. Both the Rai and Binet staging systems for CLL are used by clinicians. The Rai classification is comprised of five stages, which describe the progressive increase in disease burden over time. In the earliest stage (stage 0), CLL is purely ‘leukaemic’; there are only circulating malignant lymphocytes in the peripheral blood. The stage after this involves the lymph nodes (stage I). An involved lymph node will contain an infiltrate of malignant lymphocytes that are morphologically the same as the cells circulating in the peripheral blood. As the disease progresses, the spleen and liver become engorged with malignant lymphocytes, leading to organomegaly (stage II). At all stages in CLL, the bone marrow will contain malignant cells. However, in the most advanced stages (III and IV), the burden of The Rai staging system has limitations with regard to its ability to risk-stratify patients, as there are patients within Rai 0 or I disease, who only live 1-2 years from the time of diagnosis. In addition to lymphocyte doubling time and staging, several new prognostic markers have been identified (table 2), of which the most important is the presence of a chromosome 17p deletion, identified by standard cytogenetics. In addition, CD38 and ZAP-70 (by flow cytometry) are thought to have prognostic utility because of their correlation with unmutated immunoglobulin variable heavy chain (IgVH) status, which is an indicator of more aggressive disease. These latter tests are variably used and their place in CLL management is still being investigated. Treatment As with most incurable diseases, the treatment paradigm for CLL is not uniform; there is no single ‘one-size-fits-all’ treatment. In patients with early-stage disease, treatment may not be indicated. Indeed, even in young patients a period of observation is recommended to gauge the tempo of disease. Moreover, early intervention does not improve AD_ 0 3 3 _ _ _ APR0 8 _ 1 1 . p d f survival, and indeed premature and prolonged exposure to unnecessary therapy may lead to drug resistance. Chemotherapy For patients who ultimately require chemotherapy, the predominant indications are: • Progressive ‘marrow failure’ (ie, symptoms of anaemia, progressive thrombocytopenia or infections). • Constitutional symptoms such as weight loss or fatigue. • Progressive symptomatic lymphadenopathy. Symptoms such as fever or sweats are quite rare. When deciding on the treatment plan, the patient’s age and fitness for therapy are paramount (table 3). Consideration should always be given to enrolling eligible patients in a clinical trial. In older patients, less intensive oral therapy with alkylating agents such as chlorambucil or cyclophosphamide is often used for symptom control. In younger patients and selected older patients we generally aim to get a deep response, as this generally translates into more prolonged remissions. As such, more intensive therapy with fludarabine-based regimens is frequently used. Recently, the addition of the antiCD20 antibody rituximab has improved patient survival when used in combination with chemotherapy. This progressive improvement has led to drug combinations such as FCR (fludarabine, cyclophosphamide and rituximab) being used relatively early in the disease course. BEFORE PRESCRIBING PLEASE REVIEW PRODUCT AND PBS INFORMATION FOUND IN THE PRIMARY ADVERTISEMENT IN THIS JOURNAL. Pa ge 3 3 3 1 / 3 / 1 1 , 1 1 : 2 9 AM Table 1: Rai staging system for CLL Table 2: ‘New’ prognostic markers in CLL Stage (at time of diagnosis) Description Comments 0 Peripheral blood lymphocytosis In the modern era about 60% of patients present in this way I Lymphadenopathy II Organomegaly III and IV Cytopenias due to the burden of marrow involvement. Hb <110g/L or platelets <100 × 109 cells/L When deciding on the treatment plan, the patient’s age and fitness for therapy are paramount. Autoimmune cytopenias are not included as stage III or IV disease Prognostic marker Detection Example Cytogenetics/fluorescent The malignant cell in situ hybridisation karyotype is analysed. (FISH) Several cytogenetic abnormalities are recognised in CLL that help determine prognosis A deletion of the short arm of chromosome 17 (del17p) confers a poor prognosis and resistance to chemotherapy (median survival 32 months). Trisomy 12 and deletion of chromosome 13 confer a better prognosis CD38 (surrogate marker for unmutated IgVH status) The presence of CD38 on CLL cells is detected by flow cytometry CD38 positivity indicates a worse prognosis ZAP-70, a tyrosine kinase not normally found in B cells Expression of ZAP-70 can be readily detected using flow cytometry The presence of ZAP-70 suggests a worse prognosis but the assay is notoriously unreliable in inexperienced hands Allogeneic stem cell transplant Table 3: Treatment options in patients with CLL An allogeneic stem cell transplant (SCT), or allograft, is considered in patients under 55 (keeping in mind that the median age for CLL is 70). Allogeneic SCT is different from autologous SCT (described in Part 1 of this article) in several important ways. Firstly, the stem cells are not the patient’s own cells; they are obtained from a donor who is HLA (human leukocyte antigen) matched as closely as possible to the patient. Secondly, the aim of infusing donor stem cells is not only to ‘rescue’ the patient from lethal bone marrow failure resulting from highdose chemotherapy, as is the case in autologous transplant. In allogeneic SCT, the infused stem cells are themselves an important element of treatment. Once they repopulate the patient’s bone marrow (engraftment), the patient effectively has a new immune system, which ideally will recognise as foreign and kill the patient’s malignant cells. This is a therapeutic form of graft Patient ‘type’ Goal of treatment The elderly patient with comorbidities Symptom control/quality of life. Any Observe, or ‘gentle’ oral chemotherapy therapy must be balanced against with chlorambucil or comorbidities cyclophosphamide The robust older patient Quality of life always paramount. Aim for tumour bulk-reduction with ‘deepest’ response achievable, ie, reduced lymphadenopathy and reduced marrow infiltrate Observe if asymptomatic. However, if treatment is required, use up-front multidrug chemotherapy + rituximab (eg, fludarabine-based combination therapy) to achieve prolonged remission The younger patient As above. However, consider for allogeneic bone marrow transplant as part of therapy As above versus host disease. Thirdly, the chemotherapy (with or without radiotherapy) used in allogeneic SCT (termed ‘conditioning’) not only directly treats the disease (as in autologous SCT) but also prepares the bone marrow to receive the donor stem cells, and suppresses the patient’s immune system to prevent graft rejection. A recent study of patients with CLL undergoing reduced-intensity, conditioning allogeneic stem cell trans- First-line treatment options plants showed that for a subset of patients, no evidence of relapse was detectable for up to 96 months (the period of follow-up of this study). For appropriately selected patients, allografting can offer long-term disease-free survival and possibly cure. IV immunoglobulin It is well recognised that patients with CLL are often hypogammaglobulinaemic, that is, they have low levels of IgG, IgA and IgM. In patients with severe recurrent infections, monthly infusions of IV immunoglobulin (IVIg) are administered to increase baseline immunoglobulin levels. There are small studies that show reduced numbers of infections in these patients.1,2 In Australia, CLL with recurrent bacterial infection due to hypogammaglobulinaemia is an approved indication for periodic IVIg infusions. cont’d next page Wouldn’t you treat the whole thing? Depression may manifest as a variety of emotional, somatic and other associated symptoms.1 Reference: 1. American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Text revision, Washington DC: American Psychiatric Association; 2000. Eli Lilly Australia Pty Ltd, ABN 39 000 233 992, 112 Wharf Road, West Ryde NSW 2114. 01/11 AUCYM00348 ELB0071/AD www.australiandoctor.com.au 8 April 2011 | Australian Doctor | 33 AD_ 0 3 4 _ _ _ APR0 8 _ 1 1 . p d f Pa ge 3 4 3 1 / 3 / 1 1 , 1 1 : 2 9 AM HOW TO TREAT Lymphoproliferative disorders — Part 2 Follicular lymphoma Epidemiology WITH an annual incidence in Australia of at least four per 100,000 people, FL is the next most common NHL after diffuse large B-cell lymphoma (discussed in Part 1). The median age of diagnosis is in the sixth decade and the disease is generally more prevalent in women, with a female:male ratio of 1.7:1. Eighty per cent of patients present with Ann Arbor stage III or IV disease (ie, disseminated disease) and half have bone marrow involvement (for a description of Ann Arbor staging, please refer to Part 1). Despite being generally considered incurable, there has been an improvement in overall survival in these patients in recent years, which has been attributed to the introduction of the monoclonal antibody against CD20, rituximab. Pathology The malignant lymphocytes in FL are derived from germinal centre (follicle centre) B cells. B cells in germinal centres of lymph nodes normally undergo immunoglobulin class switching, switching from IgM to IgG or IgA. In FL the immunoglobulin heavy chain gene (IgH) on chromosome 14 is translocated and abuts the anti-apoptotic gene, bcl-2, on chromosome 18. This translocation is designated as t(14;18). The bcl-2 gene is already switched on in germinal centre cells, as its antiapoptotic function (preventing programmed cell death) is important in the development of normal memory B cells. Eighty-five per cent of FL cases have a detectable t(14;18) and the translocation is also found in 30% of diffuse large B-cell lymphomas. Diagnosis Unfortunately, laboratories are frequently sent tissue samples from patients with suspected lymphoma who have had only fine-needle aspirates of an accessible node. This is not a practice we generally support, for two reasons. The first is that the limited volume of diagnostic tissue obtained by aspiration risks not captur- Figure 5: Bone marrow involvement with follicular lymphoma (note the lymphomatous infiltrate along bony trabeculae). Follicular lymphoma infiltrate ing malignant tissue in the sample. The second is that nodal architecture cannot be assessed and thus the histological grade of FL cannot be determined. FL is graded 1-3, with grades 1-2 indicating a more indolent lymphoma and grade 3 being a more aggressive disease, which in some cases will lead the treating haematooncologist to pursue more intensive chemotherapy regimens. The practice of most clinicians would be to obtain an excisional node biopsy (or at least a core biopsy if accessibility is an issue, such as with retroperitoneal lymphadenopathy). Staging and prognostic markers As previously described, anatomical staging is performed according to the Ann Arbor staging system. Stages I and II are considered earlystage disease and such a presentation is uncommon in FL. It is critical to accurately stage all patients, as distinguishing stage I, II (and some stage III) will identify a potentially curable group who can achieve long-term disease-free survival with radiotherapy. Thus, most patients will have staging CT in addition to a bone marrow biopsy. recently been updated (FLIPI2). The five adverse prognostic markers that comprise this score are: • Age >60. • Hb <120g/L. • Beta2 microglobulin level higher than the upper limit of normal. • Largest involved node >6cm diameter. • Bone marrow involvement. Patients can then be riskstratified into one of three groups (low, intermediate or high risk) based on whether they have none/one, two, or three or more risk factors, respectively (table 4). Several trials have now shown improved response rates, time to progression and overall survival when patients with newly diagnosed FL are treated with upfront rituximab plus chemotherapy versus chemotherapy alone.3,4 This new index showed a fiveyear overall survival rate of 98%, 88% and 77% in each respective risk group and is more reflective of survival rates in the current rituximab era (table 4). Treatment Table 4: Overall survival of patients with follicular lymphoma based on FLIPI-2 prognostic scoring system Risk group Number of risk factors Percentage of Five-year patients overall survival Low 0 20 98% Intermediate 1-2 53 88% High ≥3 27 77% Regardless of the CT findings, if the bone marrow is involved the patient is deemed to have stage IV disease (figure 5). 18Ffluorodeoxyglucose positron emission tomography (18FFDG-PET) is being used increasingly to help separate early- versus late-stage disease. A prognostic score, the Follicular Lymphoma specific International Prognostic Index (FLIPI), was devised a few years ago using data collected on almost 5000 patients with FL. This scoring system has In the 20% of patients with stage I-II FL, local radiotherapy can achieve long-term remissions and potentially cure in 50% or more of stage I patients. A retrospective study of patients with stages I and II FL treated with radiotherapy showed that at 10 years 40% of patients were relapse-free.5 However, for most patients with stage III or IV disease, FL remains an incurable disease. The frequently indolent nature of FL in some patients means it can be viewed in many cases as a chronic disease. However, some patients with FL undergo large cell transformation, which carries a dismal prognosis. In patients with asymptomatic disease, the watch-andwait approach is usually appropriate, as there is no evidence that treating these patients early improves survival. Studies assessing the early use of rituximab are underway. The indications for treatment are similar to those of CLL and include painful or cosmetically unappealing nodal disease or constitutional symptoms of fatigue and malaise. Fever and sweats are rare presenting features of low-grade NHL. Generally, multi-agent chemotherapy in combination with rituximab is the standard approach to front-line therapy. The two most commonly used regimens are R-CVP (rituximab combined with cyclophosphamide and vincristine) or R-CHOP (cyclophosphamide, hydroxydaunorubicin, vincristine [Oncovin] and prednisolone with rituximab) — which is R-CVP with hydroxydaunorubicin (doxorubicin) added. R-CHOP is generally used in younger patients. These agents are given sequentially on the same day in an ambulatory setting. Five days of oral prednisolone 100mg is also administered. Dosing is spaced at threeweekly intervals to allow time for the bone marrow to recover. The goal is to administer six cycles of therapy, providing the lymphoma is chemotherapy sensitive and the patient is able to tolerate the treatment without significant toxicity. Again, as for CLL, less intensive regimens using alkylating agents can be used for frailer patients. Recently, results from a large international trial showed that initial chemotherapy with ongoing single-agent rituximab ‘maintenance’ therapy every three months for two years led to improved progression-free survival at a medium follow-up of 36 months of 75% in the maintenance arm versus 58% in patients not receiving threemonthly rituximab.6 When relapse occurs, a variety of treatment options are available, including: • Repeating the above therapy. • Rituximab alone. • Fludarabine-based therapy (as for CLL). • Radioimmunotherapy (radioisotope linked to a monoclonal antibody). • Autologous or allogeneic stem transplantation for younger patients. Managing patients receiving chemotherapy Neutropenia MANY of the chemotherapeutic regimens used in patients with lymphoproliferative disorders will result in a period of neutropenia. The nadir of this neutropenia is generally 7-12 days after the first day of chemotherapy administration. Haematology staff provide education on the expected effects of chemotherapy and tell patients that if they feel unwell or have a fever they must call their haematologist or oncologist immediately and present to an ED for prompt assessment. 34 | Australian Doctor | 8 April 2011 Neutropenic patients can deteriorate rapidly, so the time to the first dose of antibiotics must be minimised. As part of supportive care throughout chemotherapy, patients are given additional medications for some regimens. Granulocyte colony stimulating factor (G-CSF) is given to minimise the period of neutropenia. This is a cytokine that stimulates the marrow production of neutrophils. Pegfilgrastim is a pegylated long-acting form of G-CSF, which is given as a one-off injection each cycle. Regardless of whether they www.australiandoctor.com.au have received such cytokine support, any patient with fever post-treatment must be assessed without delay. Immunosuppression Reactivation of herpes simplex virus I and II as well as varicella zoster is not uncommon during this time, and many patients are prescribed prophylactic antiviral therapy. Additionally, oral candidiasis is common in immunosuppressed patients, and some patients are also prescribed prophylactic antifungal agents. Antibiotics to prevent Pneu- mocystis jirovecii (previously P. carinii [PCP]) infection are used in selected patients, especially if steroids are used. All patients with a new diagnosis of lymphoma should be tested for hepatitis B, hepatitis C and HIV. This is because the latter two infections may be aetiologically linked to the development of the patient’s lymphoma. Hepatitis B is particularly important to diagnose because chemotherapy with high-dose steroids can lead to a fulminant flare of the disease. Patients with AD_ 0 3 5 _ _ _ APR0 8 _ 1 1 . p d f Pa ge 3 5 3 1 / 3 / 1 1 , 1 1 : 3 1 AM are up-to-date with their five-yearly pneumococcal vaccine. As to whether these two vaccines should be administered before starting chemotherapy or after completion, no studies have been conducted that answer this question. Ideally we like to have vaccines administered months before chemotherapy. However, this is not feasible in patients requiring more immediate treatment. It should also be appreciated that the immune response an individual mounts to vaccination may be suboptimal. There is no evidence to suggest that in significantly immunocompromised patients a second vaccination will result in a more successful response. Live attenuated vaccines such as MMR and varicella quiescent hepatitis B are prescribed suppressive antiviral therapy throughout their treatment. Vaccinations Patients with indolent haematological malignancies, particularly CLL, are well recognised to be chronically immunosuppressed, primarily due to impaired humoral immunity. Chemotherapy agents, especially purine analogues such as fludarabine (which can impair T-cell immunity) and monoclonal antibodies can exacerbate any underlying immune suppression. These patients should receive the annual influenza virus vaccine, which is comprised of inactivated virus. GPs should also ensure these patients vaccines should be avoided in patients receiving chemotherapy or those with advanced disease. For patients receiving autologous or allogeneic SCTs, revaccination with the diphtheria–tetanus–pertussis vaccine, in addition to inactivated polio, haemophilus influenzae type b, hepatitis B, pneumococcal and influenza vaccines, is required. Administration of the MMR and varicella vaccines is deferred until 24 months post-transplant, the decision as to whether a patient is appropriate for these vaccines being made by the treating haematologist. At many transplant centres both patients and their GPs are provided with a list of which vaccinations are required at what time. Conclusion THE patient diagnosed today with CLL or FL has a better prognosis than patients diagnosed 10 years ago. This is largely due to the introduction of rituximab into modern treatment regimens. For most patients, these malignancies can be viewed as chronic illnesses with the goal of therapy to achieve the best possible quality of life. In younger patients, more aggressive treatment modalities may be appropriate. References GP’s contribution DR DIANNE CHAMBERS Leichhardt, NSW Case study MR RW is a longstanding patient of the practice. He is a resident of a local boarding house and suffers both from chronic schizophrenia, for which he receives risperdone, and also from type 2 diabetes, for which he requires Mixtard insulin. He is looked after primarily by the boarding-house team and community-support liaison psychiatry. He presented to us in 2006 with new-onset enlargement of the lymph glands in his left axilla. This was associated with only mild local discomfort but he had many constitutional symptoms, with drench- BEFORE PRESCRIBING PLEASE REVIEW PRODUCT AND PBS INFORMATION FOUND IN THE PRIMARY ADVERTISEMENT IN THIS JOURNAL. References: 1. Hirschfeld RMA, et al. Depress Anxiety 2005;21:170–7. 2. American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Text revision, Washington DC: American Psychiatric Association; 2000. Eli Lilly Australia Pty Ltd, ABN 39 000 233 992, 112 Wharf Road, West Ryde NSW 2114. 01/11 AUCYM00349 ELB0072/AD Available on request from julian.mcallan @reedbusiness.com.au ing night sweats, hot flushes at night and a 10kg weight loss. He was not able to tell us over what period his glands had become swollen but he did mention that he had also noticed lesser swellings in his neck and groin. Although his sleep and appetite were good, he had noticed weight loss, having to tighten his belt several notches. On examination he had bilateral cervical, axillary and inguinal lymphadenopathy. The largest lymph node was in the left axilla and measured 3 × 3cm. It was mobile and non-tender. He did not have any organomegaly. His initial white cell count was 42 × 109 cells/L, which fell to 28.7 × 109 cells/L. Haemoglobin and platelets were normal. He was initially treated with chlorambucil. All symptoms settled and lymph nodes regressed. However, with further deterioration his chemotherapy has been changed on several occasions over the last five years. The most recent CT scan in February 2011 showed widespread lymphadenopathy, with the largest node being a 4cm left axillary node. The spleen is enlarged at 16.9cm, but the liver is clear. Questions for the author Mr RW was initially prescribed chlorambucil and prednisone (‘gentle chemotherapy’). This seemed to work for a period although he continued to have palpable lymph nodes. After some time his WCC became considerably elevated and he was started on fludarabine, first as singleagent therapy and then combined with rituximab. On what criteria was Mr RW’s lymphoma deemed suitable for gentle chemotherapy? We presume Mr RW has CLL with lymphocytosis and organomegaly. Importantly the initial red cell and platelet counts are preserved. In general, treatment is indicated for symptomatic relief, marrow suppression or constitutional symptoms, particularly fatigue. A rapid lymphocyte doubling time or poor-risk cytogenetics may also influence the decision towards chemotherapy. This patient had notable weight loss and constitutional symptoms and therefore required treatment. Indeed, such a presentation can sometimes indicate an underlying transformation to a more aggressive lymphoma (Richter’s transformation). There has been a shift away from the use of gentle, less intensive chemotherapy in an attempt to achieve deeper and longer responses. However, such an approach is not for frail elderly patients and patients with multiple co-morbidities, such as Mr RW. While the disease tends to improve in the majority of patients receiving chlorambucil monotherapy, less than 5% achieve a deep prolonged response. The average dura- tion of response is typically less than two years. A more usual approach in a patient able to tolerate more aggressive treatment is the use of FCR (fludarabine, cyclophosphamide and rituximab), which results in a complete remission rate of almost 90% and a superior overall survival. In patients not suitable for FCR, a combination of chlorambucil and rituximab would be the favoured approach. Online resources A comprehensive list of useful websites can be found at: www.petermac.org/ haematologyinformation Are their any new treatment regimens in the pipeline for RW? Newer “next generation” CD20 antibodies have recently been developed. One such drug is ofatumumab, which appears to have greater potency than rituximab in patients with relapsed/refractory CLL. Bendamustine is effective in CLL and follicular lymphoma and has a particularly good toxicity profile cont’d next page THINK BROAD. TREAT BROAD. 1† † Targeting many of the symptoms of depression – DSM-IV.2 www.australiandoctor.com.au 8 April 2011 | Australian Doctor | 35 AD_ 0 3 6 _ _ _ APR0 8 _ 1 1 . p d f Pa ge 3 6 3 1 / 3 / 1 1 , 1 1 : 3 1 AM HOW TO TREAT Lymphoproliferative disorders — Part 2 from previous page but is not yet approved in Australia. Alemtuzumab, a CD52 antibody, which can be used in relapsed or refractory CLL is useful in fit, younger patients. When all conventional options have been exhausted, motivated and compliant patients can be considered for enrolment in clinical trials. One such agent currently undergoing clinical trials in Australia is ABT-263, an inhibitor of bcl-2, which is dysregulated in CLL. General questions for the author Patients with febrile neutropenia may present to GPs. Can you give more advice as to what would be a critical level and what is the appropriate antibiotic? Or do these patients all need G-CSF and hospitalisation? It is hard to tell a patient who is sitting in your clinic with no apparent symptoms of impending sepsis, other than a temperature of 38 degrees, that he or she needs to go to hospital. An absence of neutrophils generally means an absence of suppuration, so there are often no localising signs. Many patients will declare that they feel “fine”. Unfortunately, febrile neutropenic patients can deteriorate remarkably quickly, sometimes within the space of a few hours. As a general rule, a febrile neutropenic patient should come into hospital for intravenous antibiotic therapy +/- G-CSF. We use a broad spectrum antibiotic such as piperacillin/tazobactam. If an infected intravenous cannula site or central venous catheter is suspected as the source of infection, vancomycin is added to cover MRSA (methicillin resistant Staphylococcus aureus). Recent Australian guidelines have been published on the management of febrile neutropenia in cancer patients.1 Part 1 of your article advises that both mantle cell and Burkitt’s lymphoma are associated with a characteristic chromosomal translocation. Is the chromosome abnormality the primary cause for these lymphomas, or does it just represent an increased susceptibility. If it is the primary cause, are we moving towards genetic screening and anticipatory care? The chromosomal translocations that occur in haematological malignancies such as those associated with Burkitt’s lymphoma (involving the cmyc gene) and mantle cell lymphoma (involving the cyclin D1 locus) are mutations that occur within malignant cells only and are the main pathogenic steps in the development of these lymphomas. These translocations are not constitutional abnormalities (present in the germ line of the patient), rather they are acquired ‘random’ genetic events in B-lymphocytes. Consequently, there is no role for screening for these translocations in the absence of clinical disease. In Part 1, you advise there is a 20% risk of subsequent breast cancer risk in those who have had mantle radiotherapy. This is news to me. You also mention that this radiotherapy was the standard of care How to Treat Quiz 2. Which TWO statements are correct regarding chronic lymphocytic leukaemia (CLL)? a) Lymphocyte morphology on the blood film is sufficient for the diagnosis of CLL b) Flow cytometry identifies the cell surface markers present on the cell population of interest c) Flow cytometry is used only for the cells in peripheral blood d) Flow cytometry can detect minimal residual disease after treatment and can identify markers of poor prognosis 3. Which TWO statements are correct? a) The presence of <5 × 109 cells/L with the CLL phenotype in peripheral blood without lymphadenopathy or organomegaly has no clinical significance b) Patients with monoclonal B cell lymphocytosis (pre-CLL) should be monitored annually some patients makes mammography a less sensitive modality due to density of breast tissue. Given the sensitivity of breast MRI for detecting abnormalities, it may be desirable to use this modality for very select patients at high risk of subsequent breast cancer (eg, significant radiation exposure and young age); however, currently patients would have to self-fund for this investigation. The original treating team should be consulted in order to establish treatment details and to seek advice on subsequent breast cancer risk. Table 1 in Part 1 alerts us to the need to manage Helicobacter pylori and Chlamydia psittaci infections as effective treatment of extranodal disease in MALToma. What is the risk for lymphoma development in these illnesses? What is thought to be the pathophysiological effect of these organisms? Given the high prevalence of H. pylori infection (about half of the world’s population) and the relative rarity of gastric MALToma, the percentage of patients infected with H. pylori who will go on to develop gastric MALToma is extremely low. While the exact pathogenesis of extranodal MALToma is still being elucidated, the current hypothesis is that H. pylori or C. psittaci induces abnormal aggregations of lymphoid tissue, which (through chronic antigen stimulation) eventually develop a degree of autonomous growth. In the early stages of disease, the lymphocyte proliferation is still partially dependent on the presence of bacterial antigen, so removing the organism may result in resolution of the lymphoma. However, as the disease progresses, the B-lymphocytes acquire further genetic abnormalities that lead to further autonomy, independence from bacterial antigen stimulation and frank malignant behaviour. Reference 1. Internal Medicine Journal 2011; 41:75-81. INSTRUCTIONS Complete this quiz online and fill in the GP evaluation form to earn 2 CPD or PDP points. We no longer accept quizzes by post or fax. The mark required to obtain points is 80%. Please note that some questions have more than one correct answer. Lymphoproliferative disorders — Part 2 — 8 April 2011 1. Which TWO statements are correct? a) If an indolent lymphoma transforms into a more aggressive lymphoma, the prognosis is much better than for ‘de novo’ aggressive lymphomas b) Indolent lymphomas are generally regarded as curable c) On routine FBC, lymphocyte counts above 15 × 109 cells/L should be a cause for concern d) Lymphocytosis with lymphadenopathy, splenomegaly, anaemia or thrombocytopenia is suggestive of underlying malignancy about 15 or more years ago. I suspect that these patients may no longer be under the care of haematology units and would be seeing their GPs. These patients warrant aggressive breast surveillance. You state that the method of investigation is under discussion. In the meantime, would you suggest MRI (which has MBS funding for breast cancer screening in high-risk patients), ultrasound, mammogram or a combination? Due to the multitude of late effects that can occur, we recommend that all patients treated for HL (and indeed all long-term lymphoma survivors) are followed up in the long term by their haematologist/oncologist or in specialised multidisciplinary clinics dedicated to the management of the long-term effects associated with cancer treatment. Depending on risks, a review every 1-5 years may be appropriate. We suggest annual mammography and ultrasound for patients with exposure of breast tissue to radiation. However, the young age of ONLINE ONLY www.australiandoctor.com.au/cpd/ for immediate feedback c) Small cell lymphocytic lymphoma is essentially the same disease as CLL but without the leukaemic component d) An asymptomatic patient over 60 with CLL always requires full investigation and immediate treatment 4. Which TWO statements are correct regarding CLL? a) Before referring an anaemic patient with CLL, the GP should arrange a Coombs test to assess for autoimmune haemolysis b) Baseline immunoglobulin levels do not usually reflect the degree of immunosuppression c) A lymphocyte doubling time of 12 months confers a poor prognosis d) The need for treatment of CLL is determined by the presence of cytopenias, lymphadenopathy, organomegaly or constitutional symptoms 5. Which TWO statements are correct regarding CLL? a) A bone marrow biopsy will make the important distinction between autoimmune cytopenias and cytopenias due to marrow infiltration b) The extent of bone marrow infiltrate and cytogenetic abnormalities does not influence prognosis in CLL c) Patients without clinically detectable lymphadenopathy are unlikely to have occult abdominal lymphadenopathy on CT d) One of the most important prognostic markers for CLL is the presence of a chromosome 17p deletion 6. Which TWO statements are correct regarding CLL? a) Early treatment improves survival b) Indications for chemotherapy include symptomatic anaemia, infections, weight loss or fatigue c) In older patients, less intensive oral therapy (chlorambucil or cyclophosphamide) is often used for symptom control d) The combination of fludarabine, cyclophosphamide and rituximab improves symptoms but does not improve survival in younger patients 7. Which TWO statements are correct? a) In allogeneic stem cell transplant (SCT), the patient’s own stem cells are transplanted b) In allogeneic SCT the transplanted stem cells do not themselves have an anti-cancer effect c) For appropriately selected patients, allogeneic SCT can offer long-term disease-free survival and possibly cure d) In patients with CLL, IV immunoglobulin may decrease the number of infections associated with hypogammaglobulinaemia 8. Which TWO statements are correct regarding follicular lymphoma (FL)? a) Most patients with FL present with early-stage disease b) Fine-needle aspiration of lymph nodes is the preferred method of obtaining tissue for diagnosis c) Excisional biopsy of a lymph node provides an adequate tissue sample and the nodal architecture is preserved for analysis d) Adverse prognostic markers include age >60, involved lymph node >6cm, and bone marrow involvement 9. Which THREE statements are correct? a) Patients with early-stage FL can achieve longterm remissions and possible cure with local radiotherapy b) The indications for chemotherapy for FL include painful or cosmetically unappealing nodal disease, fatigue and malaise c) After chemotherapy a patient with malaise or fever should be assessed urgently for febrile neutropenia d) Patients who have received granulocyte colony stimulating factor (G-CSF) with chemotherapy are not at risk of febrile neutropenia 10. Which TWO statements are correct? a) Antiviral treatment for hepatitis B is contraindicated in lymphoma patients receiving chemotherapy with high-dose steroids b) Patients with lymphoma should receive annual influenza and five-yearly pneumococcal vaccines c) Live attenuated vaccines (eg, MMR, varicella) should be avoided in patients with lymphoma receiving chemotherapy or those with advanced disease d) Re-vaccination is contraindicated after SCT CPD QUIZ UPDATE The RACGP requires that a brief GP evaluation form be completed with every quiz to obtain category 2 CPD or PDP points for the 2011-13 triennium. You can complete this online along with the quiz at www.australiandoctor.com.au. Because this is a requirement, we are no longer able to accept the quiz by post or fax. However, we have included the quiz questions here for those who like to prepare the answers before completing the quiz online. HOW TO TREAT Editor: Dr Giovanna Zingarelli Co-ordinator: Julian McAllan Quiz: Dr Giovanna Zingarelli NEXT WEEK More than one-quarter of the population have some hearing impairment, while in the 70+ age group, the prevalence rises to 87.5%, making this yet another condition that one is likely to see more of as the population ages. The next How to Treat tackles hearing loss in the ageing patient. The authors are Dr Phil Sale, cochlear implant research fellow, Kolling Deafness Research Centre, University of Sydney, NSW; and Clinical Associate Professor Nirmal Patel, clinical director, Northside Cochlear Implant Clinic, and Director, Kolling Deafness Research Centre, University of Sydney, NSW. 36 | Australian Doctor | 8 April 2011 www.australiandoctor.com.au