Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
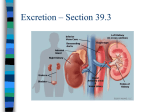
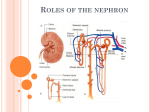
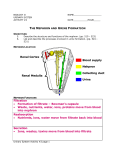
The Urinary System Organs of the Urinary System Ø Kidney Ø Ureter Ø Urinary bladder Ø Urethra Functions of the Urinary System Ø Produce Ø Waste l urine… removal urea, uric acid Ø Regulation of BV, BP of [ion]plasma Ø Help regulate plasma pH Ø Conservation of nutrients Ø Regulation 1 nephrons Ø ~1 million in an adult human kidney Ø Functional unit Ø Tube that processes filtered blood, producing urine Ø Nephron populations l 85% cortical nephrons l 15% juxtamedullary nephrons • Most of kidney function • Capacity to concentrate urine Glomerulus Ø is ~ 50 fenestrated capillaries Ø functions: l l l filtration of blood formation of filtrate filtrate is… Ø blood pressure (BHP) in capillaries forces fluid out of plasma into Bowman’s capsule Juxtaglomerular complex (JGC) Ø 2 l parts macula densa • DCT cells that monitor filtrate [Na] l juxtaglomerular cells • Smooth muscle Ø JGC is an endocrine structure l l JG cells secrete renin EPO may come from here, but details are not verified 2 Nephron Ø Ø modifies filtrate urine is the product of the modification Renal Physiology Ø Maintain l l l homeostasis Volume of blood Composition of blood Excretion of wastes • Urea - most abundant, from a.a. catabolism • Creatinine from catabolism of creatine phosphate • Uric acid from RNA recycling l Waste excretion requires water: this means we have unavoidable water loss in urine Processes of Urine Formation Ø Ø Ø Filtration Reabsorption from filtrate Secretion into filtrate 3 Glomerular Filtration 1 Ø Net filtration from glomerulus to capsular space Ø Result of 2 pressures l l Hydrostatic pressure Osmotic pressure Glomerular Filtration 2: hydrostatic pressures Ø Ø Ø Ø 2 hydrostatic pressures glomerular hydrostatic pressure (GHP) l GHP is 50 mmHg capsular hydrostatic pressure (CsHP) l CsHP is15 mmHg Net Hydrostatic Pressure (NHP) l NHP = GHP- CsHP l NHP = 50 mmHg – 15 mmHg l NHP is 35 mmHg Glomerular Filtration 3: osmotic pressure Ø blood colloid osmotic pressure (BCOP) is 25 mmHg Ø filtrate colloid osmotic pressure is 0 mmHg 4 Glomerular Filtration 4: Net Filtration Pressure Ø Net Filtration pressure (NFP) NFP = NHP – BCOP Ø NFP = 35 mmHg – 25 mmHg Ø Ø NFP = 10 mmHg GFR (glomerular filtration rate) Ø Amount l l of filtrate produced per minute Averages 125 ml/min 10% of blood delivered ends up as filtrate Ø 60 min/hour x 125 ml/min = 7500 ml/hr ml/hr x 24hr/day = 180 liters/day Ø 70 times the amount of total plasma volume! Ø 7500 Controlling GFR Ø heavily dependent on MAP decrease in MAP leads to a decrease in GFR Ø if GHP drops to 40 mmHg, filtration stops… Ø causes of drop in GHP: Ø a l Hemorrhage, shock, dehydration… Ø result: l l l accumulation of metabolic wastes control of pH jeopardized ability to regulate blood volume lost 5 Control of GFR Ø Important Ø Autoregulation Ø Hormonal Ø Autonomic Autoregulation of GFR Ø accomplished diameters of l by changing efferent and afferent arterioles Ø when blood pressure in afferent arteriole decreases, l l l l afferent arteriole dilates glomerular capillaries dilate efferent arteriole constricts effect on GFR is : ________ Ø If blood pressure in afferent arteriole increases, afferent arteriole constricts… Hormonal regulation of GFR Ø Renin-angiotensin Ø Natriuretic system peptides 6 Hormonal regulation of GFR Ø If autoregulation is insufficient to maintain GFR, renin is secreted by this sequence: l l l l a decrease in BP at glomerulus causes decreased [Na] of tubular fluid at macula densa Result: renin secretion…reninangiotensin system activation Note: sympathetic stimulation of JG cells also causes renin secretions renin angiotensin system ANP/BNP Ø atrial natriuretic peptide • atria of heart Ø brain natriuretic peptide • ventricles of heart l l l secreted if BV increases dilation of afferent arterioles constriction of efferent arterioles Ø increases GFR natriuresis Ø Result: increased urine production & decreased blood volume and pressure Ø Induces 7 Autonomic regulation of GFR Ø sympathetic l l effect: powerful vasoconstriction in afferent arteriole decreases GFR, slowing filtrate production Processes of Urine Formation Ø Filtration Ø Reabsorption l l l from filtrate diffusion osmosis carrier-mediated transport • membrane proteins necessary Ø Secretion understanding reabsorption and secretion 8 Regions of nephron & function Ø PCT l reabsorption • ions, organic molecules, vitamins, water Ø Nephron l loop reabsorption • water, NaCl Ø DCT l l reabsorption/secretion drugs, toxins Ø Collecting l system water reabsorption Osmolarity of body fluids Ø Osmolarity l l refers to number of solute particles/liter expressed in milliosmoles/L (mOsm/L) Ø Osmolarity of body fluids = 300 mOsm/L Reabsorption is based on carriermediated transport Ø 160 memory: carriers are substrate specific Ø many types of transport proteins exist in the tubule cells 9 Renal Threshold Ø carrier proteins can be “saturated”; this means a “transport maximum” (Tm) exists for solutes Ø Tm determines renal threshold l This is the plasma concentration at which a given solute will appear in the urine Ø For example, hyperglycemia results in glucosuria PCT Ø reabsorption of 60-70% of filtrate volume Ø reabsorbed solutes & water enter peritubular capillaries Ø secreted solutes enter the filtrate in the tubule lumen 10 PCT functions Ø reabsorption l organic nutrients • List some… l l l ions HCO3- (CO2) water osmolarity… Ø secretion l H+ Ø consider Na+ role nephron loop (loop of Henle) Ø Ø Ø reabsorbs l water + l Na and Cl ions maintains high [osmotic] of medulla provides the means of concentrating the urine nephron loop Ø significant l regions descending limb • thin segment • permeable to water • Impermeable to solutes l ascending limb • thick segment • impermeable to H2O • pumps out l Na+ & Cl- ions Ø removes ~2/3 of the Na and Cl that enters the loop 11 nephron loop function Ø Ø Ø pumping of Na and Cl ions out of ascending limb elevates osmotic concentration of peritubular fluid results in l water flow out of descending limb l increasing solute concentration in ascending limb high concentration in ascending limb facilitates more ion pumping concentration gradient of medulla Ø due to Na and Cl ion pumping by ascending limb Ø also…papillary duct is permeable to urea Ø urea adds to the concentration gradient of the deep medulla benefits of countercurrent multiplication Ø efficient l l reabsorption of water solutes Ø Later on…permits passive reabsorption of water in collecting system 12 DCT Ø receives 15-20% of initial volume filtered Ø reabsorption Ø secretion Ø sensitive to hormones, allows for the adjustment of urine concentration and volume DCT: reabsorption (this slide) & secretion (next 2 slides) Ø reabsorption of remaining ions l l l Na+ and Clmore Na+ if aldosterone is present Ca++ if PTH is present DCT: reabsorption (prev. slide) & secretion (this slide and next) Ø secretion l of K+ If aldosterone is present 13 DCT: reabsorption (2 slides back) & secretion (this slide and previous) Ø secretion l l of H+ increases as blood pH falls two routes • plasma pH decline • tubular cell amino acid deamination l l both generate HCO3- ions that are returned to blood result: addition of buffers in blood Collecting System Ø Ø Includes DCT and collecting duct Sensitive to hormones l l Ø Reabsorption l l l l Ø Aldosterone ADH Na+ HCO3Urea water Secretion l l H+ if pHperitubular fluid is 6 HCO3- if pHperitubular fluid is 5 Control of Urine Volume & Osmotic Concentration Ø Controlling water reabsorption 14 water reabsorption Ø result of osmosis along the nephron Ø water permeability cannot be adjusted l l in PCT descending loop of Henle Ø 85% of filtered water is reabsorbed – can’t be altered Ø “obligatory water reabsorption” the amount of water in urine Ø depends on how much of the remaining 15% is reabsorbed in DCT & collecting system Ø “how much” is reabsorbed is l l l variable precisely controlled called “facultative water reabsorption” facultative water reabsorption Ø controlled l by ADH via the insertion of water channels (aquaporins) in collecting system Ø # of water channels α to [ADH] l if [ADH] increases, then number of water channels increases…and vice versa 15 Absence of ADH Absence of ADH ADH Overview of renal function 16 Normal urine composition Ø pH 4.5- 8 (average is 6) 855-1335 Ø water content 93-97% Ø volume 700-2000 ml/day Ø color clear yellow (urobilin) Ø bacteria none* Ø osmolarity l *unless a urinary tract infection is present Urine Transport, Elimination, and Storage Ø calyces Ø ureter Ø bladder Ø urethra urethral sphincters 17 Micturition reflex controls urination Ø Ø Ø Ø Ø Ø Ø sensations of urine in bladder occur when ~200 ml is in bladder Bladder contracts and increases pressure… again ~1 hour later repeats, repeats … sensations increase in intensity voluntary relaxation of the external sphincter relaxes internal sphincter urine is released Micturition reflex may cause unplanned urination Ø Ø Ø Ø 500 ml may result in strong enough contractions to force open internal urethral sphincter followed by a reflexive relaxation of the external sphincter leading to unplanned urination Capacity: up to 1000 ml 10 ml remaining after urination Incontinence: inability to control urination Ø causes l l damaged sphincters decreased muscle tone Ø damage to nervous system and effects l damaged CNS nervous supply to external urethral sphincter • loss of voluntary control l • “automatic bladder” damaged pelvic nerves • distended bladder • continual leak of urine 18