Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
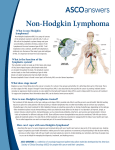
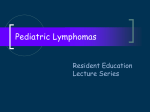
From www.bloodjournal.org by guest on June 15, 2017. For personal use only. REVIEW ARTICLE Prognostic Factorsin Aggressive Non-Hodgkin’sLymphoma: Who Has “High-Risk” Disease? By Margaret A . Shipp to the Ann Arbor MBINATION CHEMOTHERAPY has transformed ized and advanced stage disease according classification (Table 1).L2-28Theseclinicalcharacteristics aggressive non-Hodgkin’s lymphoma (NHL) from a were thought to reflect three basic features:(1) the tumor’s fatal diseaseto one that is now often curable. I Complete response rates of 60%to 80%and predicted 5-year survivals of growth and invasive potential (lactate dehydrogenase [LDH], stage, masssize, number of nodal and extranodal sites ofdisgreater than 55% have been obtained with current regimens e a s e , bone marrow [BM] involvement); (2) the patient’s rein pilot single-institution However, many of these sponse to the tumor (performance status, B symptoms); and regimens(MACOP-B,m-BACOD,ProMace-CytaBOM) (3) the patient’s ability to tolerate intensive therapy (perforproved to be no more effective than standarddose CHOP in mance status,BM involvement, age) (Table1). recent randomized cooperative group ~ t u d i e s ,raising ~ , ~ the disappointing possibility that the favorable pilot results were The prognostic significanceof age deserves special mention. As expected, age at diagnosis was more commonly caused in part by patient selection. This dilemma has refoidentified as a prognostic factor in studies that included large cused our attention on the need to compare treatment reginumbers of older patients.’8.22.24.26.27,29~31 In an early Southmens in comparablepatient subgroups and to identify pawest Oncology Group Trial, elderly patients who received tients with different long-term prognoses to individualize automatic dose reductions becauseof age had significantly therapy. lower complete response ratesthan elderly patients who reThe identification of “high-” or “low-risk” patients with aggressive NHL would haveimportant therapeutic implica- ceived fulldose therapy.29 In a subsequent Nebraska Lymphoma Group trial, elderly patients treated with full-dose tions. “High-risk” patients who are not effectively treated therapy had complete response rates and therapy-related with current regimens are most likely to benefit from new toxicities that were comparable with those of younger paexperimental approaches whereas“low-risk’’ patients may tients; however, fewer elderly patients survived 5 years bedo well withstandard therapy and incur substantialtoxicity cause this group had an increased incidence of death beif they are treated with experimental regimens. As noted, the of elderly identification of different patient risk groups will alsoaid in causeofunrelatedcauses.3oAdditionalseries patients from Canadaand Denmark had higher death rates the design and interpretation of therapeutic trials. caused by both the lymphoma itself and the toxicity of the This review summarizes recent efforts to develop cliniadministered ~hemotherapy.*~*” These studies highlight the cally based pretreatment prognostic factor modelsto identendency to treat elderly patients withlower doses of chetify patients with aggressive NHL who have different risks for death from their disease. Treatment-related prognostic motherapy to reduce treatment-related toxicity while emphasizing the fact that older patients benefit from full-dose factors will also be discussed. In addition, the review will therapy. highlight more recently described cellular and molecular features that may be directly associated with the biologic DEVELOPMENT OF APREDICTIVE MODEL BASED ON heterogeneity of aggressive NHL. c“ CLINICALPRETREATMENTPROGNOSTICFACTORS IDENTIFICATION OFCLINICALPROGNOSTIC FACTORS Early prognostic factor models. Manyinvestigators have identified the clinical pretreatment variables associated with survivalin univariate analysesof their own series of patients with aggressiveNHL.’2-28 Features that retained independent significance in multivariate analyses of survival were often used to develop prognostic factor models node Currently, patients with aggressive NHL are staged with the Ann Arbor classificationthat was originally developed for Hodgkin’s disease.” This classification schemaemphasizes the distribution of nodal disease sites because Hodgkin’s disease commonly spreads via contiguous lymph groups.lo Because the patterns of disease spread in Hodgkin’s and NHL are somewhat different, it is not surprising From the Department ofMedicine. Dana Farber Cancer Institute that the Ann Arbor classification is less accurate in idenand Harvard Medical School, Boston, MA. Submitted August 31, 1993; accepted November23, 1993. tifyingprognosticsubgroups of patients withaggressive Supported in part by an American Cancer Society Junior Faculty NHL.” For this reason, investigators have attempted to Award. identify clinical prognostic factors that would formthe basis Address reprint requests to Margaret A . Shipp, MD, Department of a new classification for aggressive NHL that would be o f Medicine, Dana Farber Cancer Institute and Harvard Medical more reflective ofthe unique biology ofthis disease. School, 44 BinneySt, Boston, MA 02115. In previous analyses of relatively small numbers of paThe publication costsof this article weredejiayed in part by page tients with aggressive NHL, a varietyof pretreatment clinicharge payment. This article musttherefore be hereby marked cal characteristics were consistently associated with sur“advertisement” in accordance with18 U.S.C.section I734 solelyto vival: ageat diagnosis; systemic (B) symptoms; performance indicate thisfact. status; serum LDH; number of nodal and extranodal sites 0 I994 by TheAmerican Society ofHematology. of disease; tumor bulk; and the distinction between local0006-4971/94/8305-0033$3.00/0 B/&, Vol83, No 5 (March l), 1994:pp 1 165-1173 1165 rformance From www.bloodjournal.org by guest on June 15, 2017. For personal use only. 1166 MARGARET A. SHlPP Table 1. Association Between Host/Tumor Characteristics and Clinical Prognostic Features in Aggressive NHL relative risk (low-risk [L], low-intermediate [L-l], high-intermediate [H-I], or high [H] risk) were identified (Table 333). HostITurnorCharacteristlcs Clinical ProanostE Factors In 2,03 l patients of all ages,a model (International Index) Tumor’s growth and invasive potential SerumLDH based on age, stage, serum LDH, performance status, and No. of nodaland extranodal number of extranodal disease sites identified four risk sites of disease groups with predicted 5-year survivals of 73%, 51%, 43%, Mass size Stage according to Ann Arbor and 26%,respectively (Tables 2 and 3A).33 Becauseyounger classification and older patients had significantly different outcomes and BM involvement patients 260 years were more likely to be candidates for intensive experimental regimens, an age-adjusted model for Patient’s response to the tumor Systemic B symptoms patients 560 years of age (age-adjusted International Index) Performancestatus was also de~eloped.’~ In 1,274 younger patients, the clinical Patient‘s ability to tolerate intensive Age at diagnosis features that were independently associated with survival intherapy cluded stage, LDH, and performance status (Table 2). An BM involvement age-adjusted model based on these three features (Table 2 ) identified four risk groups of patients 260 years of age with predicted 5-year survivals of 83%, 69%, 46%,and 32% (Tapredictive for an individual patient’s risk for death.19-22,24-27 ble 3B).” Although the specific clinical features used in these prognosTo determine whether younger patients had better outtic factor models differed, all models incorporated paramecomes because they presented with less extensive disease, ters of disease volume and extent of tumor involvement at the clinical characteristics of patients I and >60 years of age presentation. For example, an early prognostic factor model were compared (Table4). Equal percentages of younger and in patients treated with either M- or m-BACOD was based olderpatients presented with advanced stage disease, on pretreatment performance status, largest mass size, and multiple extranodal sites of involvement, elevated serum ’~ early progLDH, and nonambulatory performance status (Table 4), number of extranodal sites ~ f d i s e a s e .Another nostic factor model in patients treated with CHOP-bleo suggesting that the disease at diagnosis was similar in the used “tumor burden” (the number of extranodal and extentwo age groups. sive nodal sites of disease) and serum LDH.20 A similar To more specifically compare outcomes in younger and prognostic factor model in patients treated with the LNHolder patients, patients older than 60 years were also ana84 regimen incorporated tumor size, numbers of extranodal lyzed according to theage-adjusted International Index (Tasites of disease, collapsed Ann Arbor stage, and serum ble 3C). Similar numbers of younger and older patients fell into each of the four risk groups (Table 3, B and C). AlLDH.” In each model, an individual patient’s risk was rethough patients older than 60 years of agehad complete related to the numberof adverse factors present at diagnosis. The above-mentioned models were similarly predictive for sponse (CR) rates that were similar or only slightly lower than those of patients 560 years, the older patients were outcome in a large series of uniformly treated patients, suggesting that the models used slightly different parameters to identify similar patient subgroups.32 Table 2. Prognostic Factors for Survival in The International Index. To develop a widely accepted International Index Patients prognostic factor model for patients with aggressive NHL, Relative Risk PValue 16 single institutions and cooperative groups in the United States, Europe, and Canadarecently participated in the InA. Patients of all ages ternational Non-Hodgkin’s Lymphoma Prognostic Factors Age ( ~ 6years 0 v >60 years) 1.96 <.001 Project.33In this project, patients with aggressive NHL who 1.00 1.85 1 LDH (snl v >nl) Performance status (0. 1 v 2-4) 1 .80 <.001 were treated with a doxorubicin-containing combination 1.001 1.47 Stage (l/llv III/IV) chemotherapy regimen between 1982 and 1987 wereevaluExtranodal involvement ated for pretreatment clinical features predictive for overall (<l site v z 1 site) 1.48 <.001 survival and relapse-free survival. Clinical features that were B. Patients s60 yrs of age independently associated with survival included age, LDH, 2.17 <.001 Stage (l/ll v III/IV) performance status, stage, and number ofextranodal disease <.001 1.95 LDH (snl v >nl) sites (Table 2). These features were incorporated into a 1.81 1.001 Performance status (0.1 v 2-4) model that identified groups of patients with different risks The subset of factors that retained independent prognosticsignififor death (Table 3).33Because the relative risk associated cance for overall survival in International Index patients of all ages (A) and with each of the clinical features was comparable (Table 2), patients I60 years of age (B) are shown. The only factor that retained an individual patient’s relative risk for death was deterindependent prognostic significancein patients of all ages (A) but not in mined by adding the number of adverse prognostic factors patients I60 years of age (B) was the number of extranodal sites of present at diagnosis (Table 3). The relative risk for death in disease (patients 5 60years of age: s 1 site v > 1 site, relative risk 1.20. patients with each possible number of adverse prognostic P = .134). Abbreviation: nl, normal. factors was determined and groups of patients with similar ~~ ~ From www.bloodjournal.org by guest on June 15, 2017. For personal use only. ORS PROGNOSTIC Table 3. Development of a PrognosticFactor Model:The International index and Age-Adjusted index Survival (%) RFS OF CRs (%) Risk Group Risk Distribution Factors of Cases (%) A. International Index (patients of all ages) 0.1 Low 2 Low-intermediate (LI) 22 3 High-intermediate (HI) 4.5 High (H) 16 (L) 79 35 27 CR . Rate (%) 2-yr 2-yr Rate 5-yr Rate Rate 5-yr Rate 87 67 43 55 44 66 54 59 58 70 50 49 40 84 66 73 51 34 26 92 78 69 46 57 32 46 88 79 59 62 37 86 66 53 58 90 83 80 71 56 36 68 64 60 45 41 21 37 56 44 37 B. Age-Adjusted Index Appliedto Patients S 60 yrs of Age (L) L) 1167 Low Low-intermediate (LI) High-intermediate (HI) High 14 (H) 46 0 l 2 3 22 74 32 32 61 C. Age-Adjusted Index Appliedto Patients> 60 yrs of Age 75 910 18 Low Low-intermediate (LI) 35 High-intermediate (HI) High 16 (H) 1 2 3 31 47 48 31 Adapted from information appearing The in New EnglandJo~rnalofMedicine.3~ lapse from CR were also ide~~tified.’~ As in earlier much lesslikely to maintain their completeremissions age were the feas t ~ d i e s ~stage, ~ - serum ~ ~ ~LDH, ~ ~ ,and ~ ~ (compare RFS of CRs, Table3, B and C).33The age-related tures most closely correlated with the durability of CR.33 differences in relapse rates, which were most striking in lowEach ofthe clinical features associated with an increased risk and low-intermediate-risk patients (Table 3, B and C), for relapse from CR was also associated with a decreased translated into significant age-related differences in survival likelihood of achieving an initial remission,33 suggesting 1). In contrast, high-intermediatein these risk groups (Fig that the achievement and durability of a CRare related paand high-risk patients Iand >60 years of age had more rameters that should be considered together in approaches 1). comparable long-term survivals (Fig to “high-risk” patients. The previously described correlation between outcome and chemotherapy elderly in dose prompts Although the International Index and earlier prognostic speculation that certain patients older than 60 years of age factor models were specifically developed to predict outmay have had less durable CRs because they received less come in patients with aggressive NHL, such models may intensive treatment. In addition, older patients may have also be usefulin lymphoma patients with more indolent hishad blunted host immune responses to their disease. As we tologies. For example, the model developed by Coiffier et also predicted survival in a smaller series of follicular reduce the toxicity of chemotherapy with hematopoietic lymphoma patientq3*and the International Index predicted growth factors, prophylactic antibiotics, and platelet support, it will be easier to treat older patients with full-dose survival in a larger series of similarpatients (Fig 239).Furregimens and to explore additional approachesto maintainthermore, the International Index also predicted survival ing CRs in this age group. and relapse from CR in a recently described series of paIn both the International Index and the age-adjusted intients with low-grade (small lymphocytic, follicular small dex, the increased risk for death resulted from both a lower cleaved, and follicular mixed) lymphoma.@ CR rate and a higher rate of relapse from CR (Table 3).33 TREATMENT-RELATED PROGNOSTIC FACTORS Because patients with an increased risk of relapse might be It is important to distinguish pretreatment clinical feacandidates for intensive experimental “consolidation” thertures that can be used to determine upfront therapy from cell or autologous BM s u p apy with peripheral blood stem parameters that are more directly associated with response the pretreatment clinical features predictive refor to treatment. Although treatment-related parameters caninduction therapy, not be used to guide decisions regarding they provide important prognostic information regarding Table 4. Clinical Characteristics of Patients s the chemosensitivityof an individual patient’s disease. and >60 Years of Age Time to CR. In 1986, Armitageet a14’ identified the s60 yrs (%) r60 yrs (%) time required to achieve CR as an important prognostic 64 68 Advanced stage(lll/lV) variable in aggressive NHL. In their series, only40% of paElevated serum LDH 39 41 tients who required morethan 5 cycles ofstandard therapy 19 19 Non-ambulatory performance status (2-4) to achieve CR remained disease free whereas 80% of pa> 1 Extranodal disease site 30 30 tients who needed 1 3 cycles of therapy to achieve CR re- From www.bloodjournal.org by guest on June 15, 2017. For personal use only. 1168 MARGARET A . SHIPP Fig 1. Overallsurvival of younger ( ~ 6 years) 0 andolder (>60 years) patients according to the (A) Low (L)-risk age-adjusted International patients; (B) low-intermediate (L-l)-risk patients; (C) high-intermediate (H-l)-risk patients; (D) high (H)-risk patients. mained disease free at 2 years.41Engelhard et aI4’ subsequently identified timetoCR asthe most important prognostic determinant of overall survival in their series of 548 patients with aggressive NHL. These data clearly correlate rapid responses with more favorable outcome^.^^^^' However, it is difficult to evaluate time to CRusing standard radiographic techniques because patients with bulky tumors frequently have residual abnormalities of uncertain significance on plain films and CT/MRIscans. For thisreason, Kaplan et a143used gallium-67 citrate (Ga-67) imaging to distinguish between residual viable tumor andscar tissue and toassess early responses to therapy in patients with aggressive NHL. Patients with gallium-avid tumors were reevaluated after 4 to 6 cycles oftherapy and at completion the of their regimen.43Only 24% of the patients who had persistent gallium uptake midtreatment achieved long-term responses, whereas 70% of patients who were gallium-negative 80 0 I 1 L I 1 I 4 I l I 1 8 I 12 I after 4 to 6 cycles maintained durableC R S . In ~ ~more recent studies in which “high-risk” patients with aggressive NHL were imaged with Ga-67 after 2 of 4 planned cycles of highdose induction therapy, patients with negative postcycle 2 gallium scans were significantly more likely to have durable complete remission^.^^ Our own experience suggests that gallium scans provide the most useful information when they are performed with “double dose” (8 to 10 mCi) radioisotope and 72- to 96-hour views and interpreted in conjunction with standard radiographic studies by a committed radi~logist.~~ Doseintensityand schedule. As noted, early studies highlighted significant differences in survival rates of elderly patients who were treated with “full-dose’’ or “dose-reduced” induction therapy.29.30The doses of cyclophosphamide and doxorubicin administered inthe first 12 weeks of therapy were also the factors most closely associated with survival in 1 15 patients with aggressive NHL treated with CHOP, M-BACOD, or MACOP-B at Stanford U n i v e r ~ i t y . ~ ~ Similar patients who received reduced doses of cyclophosphamide on the LNH-84 regimen also had decreased CR rates and increased rates of relapse from CR.’ These data suggest that there may be a minimum dose of therapy required to achieve optimal results in aggressive NHL and that certain patients may benefit from dose escalation of the most active drugs in thisdisease.44 In additional ongoing studies, Wilson etSparanoet and others are evaluating whether a change from a bolus to infusional schedule of administration reduces the development of resistance to several of the agents commonly used to treat aggressive NHL. I 16 Years Fig 2. The age-adjusted International Index also predicts overall survival inpatientswith follicular lymphoma.The predicted survival of 148 follicular lymphomapatients stratified accordingto the ageadjusted International Index is shown.= Risk groups are defined as 3, low (L), low-intermediate(L-l), high-intermediindicated in Table ate (H-l), and high(H). CELLULAR AND MOLECULARFEATURESASSOCIATED WITH PROGNOSIS IN AGGRESSIVE LYMPHOMA It is important to recognize that the clinical features incorporated into predictive models in aggressive NHL are, in part, surrogate variables for the biologic heterogeneity of this disease. For example, it is the biologic features associated with having an elevated serum LDH rather than the From www.bloodjournal.org by guest on June 15, 2017. For personal use only. 1169 PROGNOSTICFACTORSINAGGRESSIVENHL elevated LDH itself that adversely affects a patient’s outcome. In recent years, cellular and molecular features including tumor cell proliferation, immunophenotype, adhesion molecule expression, and karyotypic abnormalities have been linked to survival in aggressive NHL. Tumor cell prolifeation. Several methods including flow cytometric DNA assessment4*and tritiated thymidine uptake49have been used to evaluate tumor cell proliferation and to correlate this parameter with long-term survival in patients with aggressive NHL. Tumorcell proliferation has also been evaluated in aggressive NHL using the nuclear proliferation antigen, Ki-67.50In patient groups that were similar in age, stage, tumor burden, LDH, therapy, and CR rate, the percentage of Ki-67+ cells was closely correlated with median survival (>60% Ki-67’ cells, median survival of 8 months v <60% Ki-67’ cells, median survival of 39 months, P = .003) and was an independent factor in multivariate analy~is.~’ Ki-67 expression was similarly associated with survival in B-lineage diffuse small cell lymphoma^.^' IMMUNOPHENOTYPIC CHARACTERISTICS B- versus T-cellphenotype. Although the majority of aggressive NHLs areof B-cell origin, up to -20% of these tumors have a T-cell phenotype. Controversy remains regarding the prognostic significance of immunophenotype in this disease. To date, morphologic distinctions between diffuse large cell and B- and/or T-cell immunoblastic lymphomas have not been associated with significant differences in out~ o m e . ~ Similarly, ’,~~ the distinction between B- and T-cell disease had no prognostic significance in a recent series of patients with aggressive NHL from Stanford.54 However, Coiffier et a155and Slymen et a156recently reported that patients with T-cell aggressive NHL relapsed from CR more frequently than patients with B-cell disease (eg, T-cell v Bcell, 43% v 29% relapse from CR, P < .OO l 5 5 ) . Majorhistocompatibility complex (MHC) molecules. Patients with drug-induced or infection-associated immunodeficiency clearly have an increased risk of developing aggressive NHL.57-59Because “tumor antigens” may be recognized in association with MHC molecules, several investigators have postulated that the absence of MHC-encoded recognition structures could limithost tumor immunosurveillance in this disease.m%6’ In a small series of large cell lymphoma patients stratified for clinical characteristics, Miller et a1@found thatpatients whose tumors lacked HLADR had significantly shorter mediansurvivals than patients with HLA-DR+ tumors (0.5 years v 2.8 years, P = .003). Although a similar trend was noted ina subsequent Eastern Cooperative Oncology Group study, the differences in survivals of patients with HLA-DR- and HLA-DR’ tumors did not achieve statistical significance.62 Investigators at University of Arizona followed up on their earlier observations6’ by correlating tumor expression of class I and class I1 MHC determinantswith the numbers of CD8’ T-tumor infiltrating lymphocytes (TIL) in patients with aggressive NHL.61 Sixty-eight percent of the tumors with low CD8+ T-TIL counts were missing one or more class I or class I1 HLA determinants, whereas only 20%oftumors with high CD8+ T-TIL were missing similar MHC determi- -/+ +/+ +/+/+ *O 0 t 1 2 3 4 5 Years Fig 3. Lymphocyte homing receptor staining intensity is correlated with overall survival in 7 7 patients with intermediate-grade lymphoma.= The predicted 5-year survivals for patients with f , , and lymphocyte homing receptor staining intensity are shown. Reproduced fromthe Journal of Clinical investigation, 1991, volume87, page 1835, by copyright permissionof the American society for Clinical Investigation.” ++ +++ nants (P= .0004), prompting speculation that the loss of tumor MHC molecules might result in low T-TILs.~’Decreased numbers ofhost tumor T-TILSwere also linked with shortened survival in B-lineage diffuse small cell lymphoma~.~’ p2 Microglobulin is a small extracellular protein that is noncovalently associated with (Y chain of the class I MHC gene; the protein is also detectable in serum. Swan et a163 have correlated elevated serum p2 microglobulin levels with high tumor burdens and shortened survival in patientswith aggressive NHL. Although increased serum 62 microglobulin levels have not yet been linked to decreased lymphoma cell surface p2 microglobulin or deficient antitumor responses, serum p2 microglobulin is an easily measured parameter that has been incorporated into a predictive serologic classification system for aggressive NHL.63 Adhesion molecule expression. The lymphocytehoming receptor (LHR, Hermes antigen, CD44) facilitates the binding of lymphocytes to high endothelial venules and permits the extravagation of lymphocytes into nodal areas.64In early studies, LHR-negative aggressive lymphomas were less likely to disseminate than lymphomas with increased LHR expression (Fig 3).65-68In additional studies, Horst et a169found that 5 1% of patients with CD44hi% lymphomas but only 12%of patients with CD44”” lymphomas presented with advanced stage disease.Not surprisingly, patients whose tumors had increasedlevelsof CD44 expressionalso had shorter survival^.^"^^ These data prompt speculation that this adhesion molecule may promote the dissemination of aggressive lymphomas. In fact, an aggressive lymphoma cell line transfected with the “hematopoietic” CD44 isoform metastasized more frequently in nude mice than CD44- parental cells.” Additional preliminary studies suggest that extranodal and advanced-stage aggressiveNHLs also express CD44 vari- From www.bloodjournal.org by guest on June 15, 2017. For personal use only. 1170 MARGARET A. SHlPP ples but was not altered in other lymphoid malignancies ants including an isoformassociatedwiththemetastatic spread of epithelial malignan~ies.~' such as follicular, Burkitts,and small lymphocytic lymphoThe lymphocyte function-associatedantigen, LFA- 1 (CD mas and acute and chronic lymphocytic leukemias.Io2bel-6 transcripts were identified in mature B cells but not pre-B l 1a/ 18) has also been implicated in lymphocyte adhesion cells, plasma cells,Tcells, and migration.@Although the absence of LFA-1 was linked or other hematopoietic cell with shortened survival in an early study of a smallnumber types,'02 prompting speculation that bel-6 may be a protoof patients with aggressive NHL,72this adhesion molecule oncogene that functions to control normal B-cell differenwas not correlated with clinical behavior in additional larger tiation and specifically contributes to the pathogenesis of ~eries.~~.~~ diffuse large cell lymphoma. For these reasons, lesions in Karyotypicabnormalities. Several chromosomal abnorbel-6may also have prognostic significance in aggressive malities have been identified in aggressive NHL, although NHL. there is no single karyotypic abnormality that is ahallmark SUMMARY for this disease. After early conflicting report^,^^,'^ Cowan et a176 showedthat DNA ploidydid not have predictive value. As the above-mentioned cellular and molecular parameKaryotypic abnormalities in genera177,78and specific deleters and newly identified biologic features are evaluated in tions and abnormalities of the short arm of chromosome 17 larger numbers of patients with aggressive NHL, the bioand 7 have been associated with adverse outcomes in aggreslogic heterogeneity ofthis disease will bebetter appreciated. sive NHL79,'0; abnormalities involving chromosomes 1, 2, With a more complete understanding of the disease, it is 3,6, 1 1, 12, 14, and 18 have also beend e s ~ r i b e d . ~ ~ , ~ ' , ' ' , ~ ~likely that we will substitute biologic variables for clinical A substantial percentage (up to30%)of aggressiveNHLs surrogate features in ourprognostic factor models and target also have the (t[ 14; 18][q32;q21]) characteristic chromothese biologic variables for therapy in specific subsets of pasomal translocation of follicularlymphomas.8',82This chrotients. In the meantime, widely accepted clinical models mosomal translocation results in inappropriately elevated such as the International Index and the age-adjusted index levels of the 18q2 l gene product, bel-2,83-87 which blocks will aid in the identification of specific patient risk groups programedcell death (apoptosis) in B lymphocyte^.^^-^' and the ongoing comparison of different therapeutic a p McDonnell and Korsemeyer" found that transgenic mice proaches. Early restaging with sensitive techniques like Gabearing a bel-2Ig minigene that structurally mimics the 67 citrate scans may also identify patients with suboptimal (t[ 14; 18][q32;q21])chromosomal translocation developed responses to induction therapy at timepoints when addifollicularhyperplasia.Inalargepercentageofthese tional therapeutic alternatives may be most effective. transgenic animals, the follicular hyperplasia evolved into immunoblastic lymphoma and inhalfof these immuACKNOWLEDGMENT noblastic lymphomas, c-myealleleswererearranged." I thank Donna Favreau for manuscript preparation. These data prompt speculation that in certain aggressive NHLs, tumor progression may be related to the aberrant REFERENCES expression of specific genes that regulate both cell death (bel1 . Coleman M, Gerstein G, Topilow A, LebowiczJ, Berhardt B, 2) and cell growth(mye)."Becausebel-2 protein levels Chiarieri D, Silver RT, Pasmantier MW Advances in chemotherwere also elevated in aggressive lymphomas without apy for largecell lymphoma. Semin Hematol24:8, 1987 (t[ 14; 18][q32;q21]), mechanisms other than chromosomal 2. Skarin AT, Canellos GP, Rosenthal DS, Case DC Jr, Maclntyre JM, Pinkus CS, Moloney WC, Frei E: Improved prognosis of translocation may also result in pathogenetically relevant diffuse histiocytic and undifferentiated lymphoma by use of hi& bel-2 overe~pression.~~ In a recent series of 371 patients with dose methotrexate alternating with standard agents (M-BACOD).J aggressive NHL, increased bel-2 expression was significantly more common in patients with advanced stage disease; bel- Clin Oncol 1:9I , 1983 3. Shipp MA, YeapBY, Hanington DP, Klatt MM, PinkusCS, 2over-expression was alsoclosely linked withreduced Jochelson MS, RosenthalDS, Skarin AT, Canellos G P The m-BAdisease-free survival(DFS) (be1-2+ patients v bel-2- or -/+ COD combination chemotherapy regimenin largecell lymphoma: patients, 57% v 75% 2-year DFSP = .006).93These observaAnalysis of the completed trial and comparison with the M-BAtions are of particular interest becauseMiyashita and COD regimen. J Clin Oncol 8:84, 1990 Reed94-95have correlated bel-2 over-expressionwithre4. Klimo P,Connors JM: MACOP-Bchemotherapyforthe duced chemosensitivity of murine and human lymphoma treatmentofdiffuse large-cell lymphoma.Ann Intern Med102596, 1985 cell lines to many of the drugs in current lymphoma regi5. Longo DL, DeVita VT Jr, Duffey PL, Wesley MN, Ihde D C , mens. In the subset of aggressive NHLs with the Hubbard SM, Gilliam M, Jaffe ES, Cossman J, Fisher RI, Young [ 14; 18][q32;q21] translocation, a polymerase chain reacRC: Superiorityof ProMACE-CytaBOM over ProMACE-MOPP in tion-based technique has been used to amplify the translothe treatmentof advanced diffuse aggressive lymphoma: Results of cation and detect minimal residual d i ~ e a s e . ~ ~ . ~ ~ a prospective randomized trial. J Clin Oncol9:25,199 I Chromosomal translocations involving 3q27and several 6. Boyd DB, Coleman M, ParishSW, Topilow A, Kopel SK, other loci have been identified in8% to 12% of diffuselymBernhardtB, Files JC,Schwartz S, Gaynor M, McDermott D, phomas?'"''Ye et all" recently cloned a gene from the Reisman AM, Coleman MI: COPBLAM 111: Infusional combina3q27 breakpoint and identified it as a putative zinc finger tion chemotherapy for diffuse large-cell lymphoma. J Clin'Oncol6: transcription factor, bel-6. The bel-6 gene was truncated 425,1988 7. Coiffier B, GisselbrechtC,HerbrechtR,TillyH, Body A, within its 5' noncoding region in 33% of diffuse LCL sam- From www.bloodjournal.org by guest on June 15, 2017. For personal use only. PROGNOSTICFACTORS IN AGGRESSIVENHL Brousse N:LNH-84 regimen:A multicenter study of intensivechemotherapy in 737 patients with aggressivemalignant lymphoma. J Clin Oncol 7:1018, 1989 8. Gordon LI, Hanington D,Andersen J, Colgan J, Glick J, Neiman R, Mann R, Resnick GD, Barcos M, Gottlieb A, OConnell M: Comparison of a second-generation combination chemotherapeutic regimen (m-BACOD) witha standard regimen (CHOP) for advanced diffuse non-Hodgkin’s lymphoma. N Engl J Med 327: 1342,1992 9. Fisher RI, Gaynor ER, Dahlberg S, Oken MM, Grogan TM, Mize EM, Glick JH, Coltman CA, MillerT P Comparison ofa standard regimen (CHOP) with three intensivechemotherapy regimens for advanced non-Hodgkin’slymphoma. N Engl J Med 328:1002, 1993 10. Carbone PP, Kaplan HS, Musshoff K, Smithers DW, Tubiana M: Report of the Committee on Hodgkm’s Disease Staging Classification.Cancer Res 3 1 :1860, 197l 1 1. Rosenberg SA: Validity of the Ann Arbor staging classification for the NHLs. Cancer Treat Rep 61: 1023, 1977 12. Fisher R, DeVita VT, Johnson BL, Simon R, Young RC: Prognostic factors for advanced diffuse histiocytic lymphoma following treatment with combination chemotherapy. Am J Med 63: 177,1977 13. Cabanillas F, Burke JS, Smith TL, Moon ME, Butler JJ, Rodriguez V: Factors predicting for response and survival in adults with advanced non-Hodgkin’s lymphoma. Arch Intern Med 138: 413, 1978 14. Ferraris AM, Giuntini P, Gaetani G F Serum lactic dehydrogenase as a prognostic tool for NHLs. Blood54:928, 1979 15. Schneider RJ, Seibert K, Passe S, Little C, Gee T, LeeBJ 111, Mike V, Young C W Prognostic significance ofserum lactate dehydrogenase in malignant lymphoma. Cancer 46: 139, 1980 16. Armitage JO, Dick FR, Corder MP, Garneau SC, Platz CE, Slymen DJ: Predictingtherapeutic outcome in patients with diffuse histiocytic lymphoma with cyclophosphamide, adriamycin, vincristine and prednisone (CHOP). Cancer 5 0 1695, 1982 17. Fisher RI, Hubbard SM, DeVita VT, Berard CW, Wesley R, Cossman J, Young R C Factors predicting long-term survivalin diffuse mixed, histiocytic,or undifferentiated lymphoma. Blood 58: 45, 1981 18. Jagannath S, Velasquez WS, Tucker SL, Manning JT, McLaughlin P, Fuller LM: Stage IVdiffuse large-celllymphoma: A long-term analysis.J Clin Oncol3:39, 1985 19. Shipp MA, Harrington DP, Klatt MM, Jochelson MS, Pinkus GS, Marshall JL, Rosenthal DS, Skarin AT, CanellosG P Identification of major prognostic subgroups of patients with large-cell lymphoma treated withm-BACOD or M-BACOD.Ann Intern Med 104:757,1986 20. Jagannath S, Velasquez WS, Tucker SL,FullerLM, McLaughlin PW, Manning JT, North LB, Cabanillas FC: Tumor burden assessment and its implication for a prognostic model in advanced diffuse large-celllymphoma. J Clin Oncol 4:859, 1986 2 I . Danieu L, Wong G, Koziner B, Clarkson B Predictive model for prognosis in advanced diffuse histiocytic lymphoma. Cancer Res 465372, 1986 22. Velasquez WS, Jagannath S, Tucker SL, Fuller LM, North LB, Redman JR, Swan F, HagemeisterFB, Mclaughlin P,Cabanillas F: Risk classification as the basis for clinical staging of diffuse large-cell lymphoma derived from 10-year survivaldata. Blood 74: 551, 1989 23. Jones SE, MillerTP, Connors JM: Long-term follow-upand analysis for prognostic factors for patients with limited-stagediffuse large-cell lymphoma treated with initial chemotherapy with or without adjuvant radiotherapy. J Clin Oncol 9: 1 186, 1989 1171 24. Hoskins PJ, Ng V, Spinelli JJ, Klimo P, Connors J M Prognostic variablesin patients with diffuselarge-cell lymphoma treated with MACOP-B.J Clin Oncol 9:220, 1991 25. Coiffier B, Gisselbrecht C, Vose JM, Tffly H, Herbrecht R, Body A, Armitage J O Prognostic factorsin aggressive malignant lymphomas description and validation of a prognostic index that could identify patients requiring a moreintensivetherapy. The Groupe &Etudes des Lymphomes Aggresifs. J Clin Oncol 9 21 1,199 l 26. Velasquez WS,Fuller LM, Jagannath S, Tucker ST,North LB, Hagemeister FB, McLaughlin P, Swan F, Redman JR, Rodriques MA, Cabanillas F Stages I and I1 diffuse large cell lymphomas: Prognosticfactors and long-term results with CHOP-bleo and radiotherapy. Blood 77:942, 1991 27. Hayward RL, Leonard RCF, PrescottRI, with the members of the Scotland and Newcastle Lymphoma Group Therapy Working Party: A critical analysis of prognostic factors for survival in intermediate and high grade NHL.Br J Cancer 63:945,199 1 28. Kim D, Mauch P, Shaffer K, Pinkus G, Shipp MA, Kaplan WD, Tung N, Wheeler C, Beard C J , Canellos GP, Shulman LN: Largecell and immunoblastic lymphoma of the mediastinum: Prognostic features and treatment outcome in 57 patients. J Clin Oncol 11:1336,1993 29. Dixon D O , Neilan B, Jones SE, Lipschitz DA, Miller TP, Grozea PN, Wilson HE: Effect of age on therapeutic outcome in advanced diffuse histiocytic lymphoma: The Southwest Oncology Group Experience. J Clin Oncol 4:295,1986 30. Vose JM, Armitage JO, WeisenburgerDD, Bierman PJ, Sorensen S, Hutchins M, MoravecDF, Howe D, Dowling MD, Mailliard J, Johnson PS, PevnickW,Packard WM, Qkerbloom J, Thompson RF, Langdon RM, Soon G, Peterson C The importance of age in survival of patients treated with chemotherapy for aggressive non-Hodgkin’slymphoma. J Clin Oncol 6:1838, 1988 3 l. d‘Amore F, Brincker H, Christensen BE, Thorling K,Pedersen M, Nielsen JL, Sandberg E, Pedersen N T , Sorensen E: NonHodgkin’s lymphoma in the elderly. AnnOncol 3:379, 1992 32. Coiffier B, Lepage E Prognosis of aggressive lymphomas:a study of fiveprognostic models with patients included in the LNH84 regimen. Blood74:558, 1989 33. Shipp MA, Harrington DP, Anderson JR, Armitage JO, Bonadonna G, Brittinger G, Cabanillas F, Canellos GP, Coiffier B, Connors JM, Cowan RA, Crowther D, Dahlberg S, Engelhard M, Fisher RI, Gisselbrecht C, Homing SJ, Lepage E, Lister A, Meerwaldt JH, Montserrat E, Nissen NI, Oken MM, PetersonBA, Tondini C, Velasquez WS,Yeap BY A predictive modelfor aggressive NHL: The International Non-Hodgkin’s Lymphoma Prognostic Factors Project. N Engl J Med 329:987, 1993 34. Gulati SC, Shank B, Black P, Yopp J, Koziner B, Straus D, Filippa D, Kempin S, Castro-Malaspina H, Cunningham I, Berman E, Coleman M, Langleben 0, Calvin OM, Fuks Z, O’Reilly R, Clarkson B Autologous bone marrow transplantation for patients with poor-prognosislymphoma. J Clin Oncol6: 1303, 1988 35. Nademanee A, Schmidt G, O’Donnell M,Snyder D, Parker PA, Stein A, Smith E, LipsettJA, SniecinskiI, Margolin K, Somlo G, Niland JC, Blume KG, Forman SI: Highdose chemoradiotherapy followed by autologous bone marrowtransplantation as consolidation therapy during first complete remission in adult patients with poor-risk aggressive lymphoma:A pilot study.Blood 8 0 1 130, 1992 36. Haioun C, Lepage E, Gisselbrecht C, Coiffier B, Body A, Tilly H, Dupriez B, Nouvel C, Sebban C, Herbnxht R, Gaulard Ph, Reyes F Autologous bonemarrow transplantation versus sequential chemotherapy in first complete remissionaggressive nonHodgkin’slymphoma: 1st interim analysis on 370 patients (LNH87 protocol). Proc Am SOC Clin Oncol 1 I :107 1 a, 1992 (abstr) 37. Freedman AS, Takvorian T, Neuberg D, Mauch P, Rabi- From www.bloodjournal.org by guest on June 15, 2017. For personal use only. 1172 nowe SN, Anderson KC, Soiffer RJ, Spector N, Grossbard M, Robertson MJ, Blake K, Coral F, Canellos GP, Ritz J, Nadler LM: Autologous bone marrow transplantation in poor-prognosis intermediate-grade and high-grade B-cell non-Hodgkin’s lymphoma in first remission: A pilot study. J Clin Oncol I 1:93 1, 1993 38. Bastion Y, Berger F, Bryon PA, FelmanD, Ffrench M, Coiffier B: Follicular lymphomas: Assessment of prognostic factors in 127 patientsfollowed for 10 years. Ann Oncol 25:123, 1991 39. Coiffier B, Bastion Y, Berger F, Felman P, Bryon PA: Prognostic factors in follicular lymphoma. Semin Hematol (in press) 40. Lopez-Guillermo A, Montserrat E, Rozman C: The international prognostic index (IPI) for large-cell lymphomas is also useful when applied to patients with low-grade lymphoma. Lugano, Switzerland, FiRh International Conference on Malignant Lymphoma, June 1993, p 59 (abstr) 4 I . Armitage JO, Weisenburger DD, HutchinsM, Moravec DF, Dawling M, Sorensen S, Mailliard J, Okerbloom J, Johnson PS, Howe D, Bascom GK, Casey J, Linder J, Purtilo DT: Chemotherapy for diffuse large-cell lymphoma-Rapidly responding patients have more durable remissions. J Clin Oncol4: 160, 1986 42. Engelhard M, Meusers P, Brittinger G, Brack N, Dornoff W, Enne W, Gassmann W, Gerhartz H, Hallek M, Heise J, Hettchen W, Huhn D, Kabelitz K, Kuse R,Lengfelder E, Ludwig F, Meuthen I, Radtke H, Schadeck C, Schober C, Schumacher E, Siegert W, Staiger H-J, Terhardt E, Thiel E, Thomas M, Wagner T, Willems G, Wilmanns W, Zwingers T, Stein H, Tiemann M, Lennert K: Prospective multicenter trial for theresponse-adapted treatment of high-grade malignant non-Hodgkin’s lymphomas: Updated results of the COP-BLAM/IMVP- I6 protocol with randomized adjuvant radiotherapy. Ann Oncol2: 177, 199l 43. KaplanWD,Jochelson MS, Herman TS, Nadler LM, Stromper PC, Takvorian T, Andersen JW, Canellos GP: Gallium67 imaging: A predictor ofresidual tumor viability and clinical outcome in patients with diffuse large-cell lymphoma. J Clin Oncol 8: 1966, I990 44. Shipp MA, Shulman LN, Kaplan WD, Neuberg D, Canellos GP: Intensified induction therapy for patientswith “high-risk” aggressive N H L High dose CHOP. Am SOCHematol82:332a, 1993 (SUPPI 1) 45. Kwak LW, Olshen RA, Halpern J, Homing SJ: Dose intensity (di): Relationship to prognostic factors for diffuse large cell lymphoma. J Clin Oncol 8:963, 1990 46. Wilson WH, Bryant G, Bates S, Fojo A, Wittes RE, Steinberg SM, Kohler DR, Jaffe ES, Herdt J, Cheson BD, Chabner BA: EPOCH chemotherapy: Toxicity and efficacy in relapsed and refractory non-Hodgkin’s lymphoma. J Clin Oncol I l: 1573, I993 47. Sparano JA,Wiernik PH, Leaf A,Dutcher J P Infusional cyclophosphamide, doxorubicin, and etoposide in relapsed and resistant non-Hodgkin’s lymphoma: Evidence for a schedule-dependent effect favoring infusional administration of chemotherapy. J Clin Oncol 11:107l, 1993 48. Bauer KD, Merkel DE, Winter JN,Marder RJ, Hauck WW, Wallmark CB, Williams TJ, Variakojis D Prognostic implication of ploidy and proliferative activity in diffuse large cell lymphomas. Cancer Res 46:3 173, 1986 49. Bino GD, Silvestrini R, Costa A, Veneroni S, Giardini R Morphological and clinical significance of cell kinetics in nonHodgkin’s lymphomas. Basic Appl Histochem 30: 197, 1986 50. Grogan TM, Kippman SM, Spier CM, Slymen DJ, Rybski JA, Rangel CS, Richter LC, Miller T P Independent prognostic significance of a nuclear proliferation antigen in diffuse large cell lymphomas as determined by the monoclonal antibody Ki-67. Blood 71:1157, 1988 51. Medeiros U, Picker U, Gelb AB, Strickler JG, Brain SW, MARGARET A. SHlPP Weiss LM, Homing SJ, Warnke RA: Numbers of host “helper” T cells and proliferating cells predict survival in diffuse small-cell lymphomas. J Clin Oncol 7: 1009, 1989 52. Kwak LW, Wilson M, Weiss LM, Horning S J , Warnke RA, Dorfman R F Clinical significance of morphologic subdivision in diffuse large cell lymphoma. Cancer 68:1988, 1991 53. Nathwani BN, Dixon DO, Jones SE, Hartsock RJ, Rebuck JW, Byrne GE Jr, Sheehan WW, Kim H, Coltman CA Jr, Rappaport H: The clinical significance of the morphological subdivision of diffuse “histiocytic” lymphoma: A study of 162 patients treated by the Southwest Oncology Group. Blood 60: 1068, 1982 54. Kwak L, Wilson M, Weiss LM, Doggett R, Dorfman RF, Warnke RA, Horning SJ: Similar outcome of treatment of B-cell and T-cell diffuse large-cell lymphomas: The Stanford Experience. J Clin Oncol 9: 1426, 1991 55. Coiffier B, Brousse N, Peuchmaur M, Berger F, Gisselbrecht C, Bryon PA, Diebold J: Peripheral T-cell lymphomas have a worse prognosis than B-cell lymphomas: A prospective study of 36 1 immunophenotyped patients treated with the LNH-84 regimen. Ann Oncol 1:45, 1990 56. Slymen DJ, Miller TP, Lippman SM, Spier CM, Kerrigan DP, Rybski JA, Rangel CS, Richter LC, Grogan TM: Immunobiologic factors predictive of clinical outcome indiffuse large-cell lymphoma. J Clin Oncol 8:986, 1990 57. List AF, Greco FA, Vogler LB: Lymphoproliferative diseases in immunocompromised hosts: The role of Epstein-Barr virus. J Clin Oncol 5: 1673, 1988 58. Swinnen W ,Costanzo-Nordin MR, Fisher SG, O’Sullivan EJ, Johnson MR, Heroux AL, Dizikes GJ, Pifarre R, Fisher RI: Increased incidence of lymphoproliferative disorder afterimmunosuppression with themonoclonalantibody OKT3 in cardiactransplant recipients. N Engl J Med 323: 1723, I990 59. Ziegler JL, Meckstead JA, Volberding PA, Abrams Dl, Levine AM, Lukes RJ, Gill PS, Burkes RL, Meyer PR, Metroka CE, Mouradian J, Moore A. Riggs SA, Butler JJ, Cabanillas FC, Hersh E, Newell GR, Laubenstein U, Knowles D, OdajnykC, Raphael B, Koziner B, Urmacher C,Clarkson BD: Non-Hodgkin’s lymphoma in 90 homosexual men: Relationshipto generalized lymphadenopathy and acquired immunodeficiency syndrome (AIDS). N En@ J Med 31 1565, 1984 60. Miller TP, Lippman SM, Epier CM, Slymen DJ, Grogan TM: HLA-DR (la) immune phenotype predicts outcome for patients with diffuse large cell lymphoma. J Clin Invest 82:370, 1988 6 1. List AF, Spier CM, Miller TP, Grogan TM: Deficient tumorinfiltrating T-lymphocyte response in malignant lymphoma: Relationship to HLA expression and host immunocompetence. Leukemia 7:398, 1993 62. OKeane JC, Mack C, Lynch E, Hamngton D, Neiman RS: Prognostic correlation of HLA-DR expression in large cell lymphoma as determined by LN3 antibody staining. Cancer 66: 1 147. 1990 63. Swan F Jr, Velasquez WS, Tucker S, Redman JR, Rodriguez MA, McLaughlin P, Hagemeister FB, Cabanillas F: A new serologic staging system for large-cell lymphomas based on initial B2-microglobulin and lactage dehydrogenase levels. J Clin Oncol 7: 1518,1989 64. Stoolman LM: Adhesion molecules controlling lymphocyte migration. Cell 56:907, 1989 65. Picker LJ, Medeiros U,Weiss LM, Wamke RA, Butcher EC: Expression of lymphocyte homing receptor antigen in nonHodgkin’s lymphoma. Am J Pathol 130:496, 1988 66. Pals ST, Horst E, Ossekoppele GJ, Figdor CC, Scheper RJ, Meijer CJLM: Expression of lymphocyte homing receptor as a mechanism ofdissemination in NHL. Blood 72:885, 1989 67. Jalkanen S, Joensuu H, KIemi P Prognostic value of lym- From www.bloodjournal.org by guest on June 15, 2017. For personal use only. PROGNOSTIC FACTORS IN AGGRESSIVE NHL phocyte homing receptor and S phase fraction in non-Hodgkin’s lymphoma. Blood 75: 1549, 1990 68. Jalkanen S, Joensuu H, Soderstrom K-0, Kleimi P Lymphocyte homing and clinical behavior of non-Hodgkin’slymphoma. J Clin Invest 87: 1835, 199 1 69. Horst E, Meijer CJLM, Radaszkiewicz T, Ossekoppele GJ, van Krieken JHJM, Pals ST: Adhesion moleculesin the prognosis of diffuse large-celllymphoma: Expression of a lymphocyte homing receptor (CD44), LFA-I(CD1 la/18), andICAM-I (CD54).Leukemia 4:595, 1990 70.SyMS, Guo Y-J, Stamenkovic I: Distincteffects of two CD44 isoforms on tumor growth in vivo. J Exp Med 174:859, 1991 7 I . Salles G, Zain M, Boussiotis VA, Shipp MA: Alternatively spliced CD44 transcripts in diffuse large cell lymphomas: Characterization and comparison with normal activated B cells and epithelial malignancies. Blood 82:3539, 1993 72. Clayberger C, MedeirosU,Link MP, Warnke RA, Wright A, Koller TD, Smith SD, Krensky AM: Absence of cell surface LFA-I as a mechanism ofescape from immunosurveillance.Lancet 2:533, 1987 73. Medeiros U, Weiss LM, Picker U, Clayberger C, Homing SI, Krensky AM, Warnke RA: Expression of LFA-Iin non-Hodgkin’s lymphoma. Cancer 63:255, 1989 74. Woolidge TN, Grierson HL, Weisenburger DD, Armitage JO, Sanger WC, Collins MM, Pierson JL, Pauza ME, Fordyce R, Purtilo D T Association of DNAcontent and proliferative activity with clinical outcome in patients with diffuse mixed celland large cell non Hodgkin’s lymphoma. Cancer Res 48:6608, 1988 75. Lehtinen T, Aine R, Lehtinen M, Kallioniemi OP, Leino T, Hakala T, Lienikki P, Alavaikko M: Flow cytometric analysis of 199 histologically favourableor unfavourable non Hodgkin’s lymphomas. J Pathol 157:27, 1989 76. Cowan RA, Hanis M, Jones M, Crowther D DNA content in high and intermediate grade non-Hodgkin’s lymphoma-prognostic significance and clincopathological correlations.Br J Cancer 6094,1989 77. Levine EG, Arthur DC, Frizzera G, Peterson BA, Hurd DD, Bloomfield CD: Cytogenetic abnormalitiespredict clinicaloutcome in non-Hodgkin’slymphoma. Ann Intern Med 108: 14, 1988 78. Schouten HC, Sanger WC, Weisenburger DD, Anderson J, Armitage JO: Chromosomal abnormalities in untreated patients with non-Hodgkin’s lymphoma: Associations with histology, clinical characteristics,and treatment outcome. Blood 75: 184 I , 1990 79.Cabganillas F, Pathak S, Grant G, Hagemeister FB,McLaughlin P, Swan F, Rodriguez MA, Trujillo J, Cork A, Butler JJ, Katz R, Bourne S, Freireich U:Refractoriness to chemotherapy and poor survival relatedto abnormalities of chromosomes I7 and 7 in lymphoma. Am J Med 87: 167, 1989 80. Rodriguez MA, Ford RJ, Goodacre A, Selvanayagam P, Cabanillas F, Deisseroth AB Chromosome 17p and p53 changes in lymphoma. Br J Haematol79:575, 1991 81. Yunis JJ, Mayer MC, Arnesen MA, Aeppli DP, Oken MM, Frizzera G: bcl-2and other genomic alterations in the prognosis of large-cell lymphoma. N Engl J Med 320 1047, 1989 82. Offit K, Wong G, Filippa DA, Tao Y, Chaganti RSK Cytogenetic analysis of 434 consecutively ascertained specimens of nonHodgkin’s lymphoma: clinical correlations. Blood 77: 1508, 199 I 83. Tsujimoto Y, Gorham J, Cossman J, Jaffe E, Croce CM: The t( 14; 18) chromosome translocations involved in B-cell neoplasms result from mistakesin VDJ joining. Science 229: 1390, 1985 84. Bakhshi A, Jensen JP, Goldman P, WrightJJ, McBridge OW, Epstein AL, Korsmeyer SI: Cloning the chromosomal breakpointof t( 14; 18)human lymphomas: Clusteringaround JHon chromosome 14 and neara transcriptionalunit on 18. Cell 41:889, 1985 85. Cleary ML, SklarJ: Nucleotide sequence ofa t( 14; 18)chro- 1173 mosomal breakpoint in follicular lymphoma and demonstration of a breakpoint-cluster region near a transcriptionally active locus on chromosome 18. Proc Natl Acad Sci USA 82:7439, 1985 86. Cleary ML,Smith SD, Sklar J: Cloning and structural analysis of cDNAs for bcl-2 and a hybrid bcl-2/immunoglobulin transcript resulting fromthe t( 14; 18)translocation. Cell 47: 19, 1986 87. Seto M, Jaeger U, Hockett RD, Graninger W, Bennett S, Goldman P, Korsmeyer SJ: Alternative promoters and exons, somatic mutation and deregulation of the Bcl-2”Ig fusion gene in lymphoma. EMBO J 7: 123, 1988 88. Hockenbery D, Nunez G, Milliman C, Schreiber R, Korsmeyer SJ: Bcl-2 is an inner mitochondrial membrane protein that blocks programmed cell death. Nature 348:334, 1990 89. Vaux DL, Cory S, Adams JM: Bcl-2 gene promotes haemopoietic cell survivaland cooperates with c-mycto immortalize preB cells. Nature 335:440, 1988 90. Nunez G, London L, Hockenberg D, Alexander M, McKearn JP, Korsmeyer SJ: Deregulated bcl-2 gene expressionselectively prolongs survival of growth factor-derived hemopoietic cell lines.J Immunol 144:3602, 1990 9 I . McDonnell TJ, Korsmeyer SJ: Progression from lymphoid hyperplasia to high-grade malignant lymphoma in mice transgenic for the t( 14; 18).Nature 349:254, 1991 92. Zutter M, HockenbergD, Silverman CA, Korsmeyer SI: Immunolocalization of the bcl-2 protein within hematopoietic neoplasms. Blood 78:1062, 1991 93. Hermine 0,Haioun C, LepageE, d’Agay MF, BriereJ, Tilly H, Fillet G, Coiffier B,Gisselbrecht C, Diebold J, Reyes F, Gaulard Ph:Bcl-2 protein expressioninaggressivenon-Hodgkin’slymphoma (NHL). A new adverse prognostic factor? Lugano, Switzerland, Fifth International Conference on Malignant Lymphoma, June 1993,p 28 (abstr) 94. Miyashita T, Reed JC: Bcl-2 gene transfer increases relative resistance of S49.1and WEH17.2 lymphoid cells to cell death and DNA fragmentation induced by glucocorticoids and multiple chemotherapeutic drugs. Cancer Res 52:5407, 1992 95. Miyashita T, Reed JC: Bcl-2 oncoproteinblocks chemotherapyinduced apoptosis in a human leukemia cell line. Blood8 1:15 I, 1993 96. Gribben JG, Freedman AS, Woo SD, Blake K, Shu RS, Freeman G, Longtine JA, Pinkus CS, Nadler LM: All advanced stage non-Hodglun’s lymphomas with a polymerase chain reaction amplifiable breakpointof bcl-2 have residual cellscontaining the bcl-2 rearrangementat evaluation and after treatment. Blood 78:3275, 1991 97. Gribben JG, Freedman AS, Neuberg D, Roy DC, Blake KW, Woo SD, Grossbard ML, RabinoweSN, Coral F, Freeman GJ, Ritz J, Nadler LM: Immunologic purging of marrow assessed by PCR before autologous bonemarrow transplantation for B-cell lymphoma. N Engl J Med 325: 1525, 1991 98. Offit K, Jhanwar S, Ebrahim SAD, Filippa D, Clarkson BD, Chaganti RSK t(3;22)(q27;ql1): A novel translocation associated with diffuse non-Hodgkin’slymphoma. Blood 74:1876, 1989 99. Bastard C, Tilly H, Lenormand B,BigorgneC, Boulet D, Kunlin A, Monconduit M,PiguetH: Translocations involving band 3q27 and Ig gene regions in NHL. Blood 79:2527, 1992 1 0 0 . Baron BW, Nucifora G, McCabe N, Espinosa111R, LeBeau MM, McKeithan T W Identification of the gene associated with the recurring chromosomal translocations t(3; 14)(q27;q32) and t(3;22Mq27;q1 1) in B-celllymphomas. Proc NatlAcad Sci USA9 0 5262, 1993 101. Ye BH, Rao PH, Chaganti RSK, Dalla-Favera D Cloning of bcl-6, the locus involvedin chromosome translocationsaffecting band 3q27 in B-cell lymphoma. Cancer Res 53:2732,1993 102. Ye BH, Lista F, Lo Coco F, KnowlesDM, Offit K,Chaganti RSK, Dalla-Favera R: Alterations of a zinc finger-encoding gene, bcl-6 in diffuse large-celllymphoma. Science 262:747, 1993 From www.bloodjournal.org by guest on June 15, 2017. For personal use only. 1994 83: 1165-1173 Prognostic factors in aggressive non-Hodgkin's lymphoma: who has "high- risk" disease? MA Shipp Updated information and services can be found at: http://www.bloodjournal.org/content/83/5/1165.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.