Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Auditory processing disorder wikipedia , lookup
Speech perception wikipedia , lookup
Hearing loss wikipedia , lookup
Sound localization wikipedia , lookup
Olivocochlear system wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
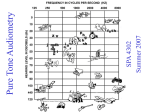
Auditory Assessment Bastaninejad, Shahin, MD, ORL-HNS Assistant Prof., TUMS Amiralam Hospital Acknowledgment: I would like to appreciate Prof. Borghei, for preparing this presentation CHL SNHL Auditory Assessment Subjective tests 1. Tuning fork tests (TFT) 2. Pure tone audiometry (PTA) 3. Speech audiometry Objective tests 1. 2. 3. 4. Impedance audiometry (Tym,AR) Auditory Brainstem Response (ABR) Otoacoustic Emission (OAE) ... Tuning Fork Tests (TFT) 1. Rinne’s test 2. Weber’s test 3. Absolute Bone Conduction (ABC) Rinne’s Test Tuning Fork Tests (TFT) Rinne’s Test Principal: AC>BC Rinne +: AC>BC, normal hearing or sensorineural hearing loss Rinne -: AC<BC, conductive HL False Rinne –: unilateral deep SNHL, due to cross over phenomena ,this can be avoided with masking Weber’s Test Tuning Fork Tests (TFT) Weber’s Test Principal: compares the BC of the two ears Normal: hears equal on both sides or does not hear at all Conductive HL: lateralized to the more affected side SNHL: lateralized to the less affected side Tuning Fork Tests (TFT) Absolute Bone Conduction test (Schwabach test) Compares the BC of the examiner with the patient • Normal: equal to the examiner • CHL: longer than the examiner • SNHL: less than the examiner Pure Tone Audiometry (PTA) It is the graphic record of hearing Quantitatively & Qualitatively Pure tones are delivered by headphone for AC & by a vibrator for BC • X-Axis: Frequency range 125 – 12000 Htz (routinely depicted from 250-8000 Htz) • Y-Axis: Intensity of sound in decibels (dB) A decibel is the smallest change in the intensity of sound which can be recognized by normal human ear Pure Tone Audiometry (PTA) Pure Tone Audiometry (PTA) Normal Audiogram Pure Tone Audiometry (PTA) Range of hearing loss Pure Tone Audiometry (PTA) Conductive Hearing Loss (CHL) Pure Tone Audiometry (PTA) Sensori-Neural Hearing Loss (SNHL) Pure Tone Audiometry (PTA) Mixed Hearing loss Masking To prevent ‘crossover’ phenomena Crossover happens with • 40-60 dB AC difference in two ears • 0-20 dB BC difference in two ears Masking problem • Masking dilemma; in bilateral CHL or Bilateral Mixed HL • Overmasking masking noise crosses over to the other side Speech Audiometry Recorded voice is used Speech Detection threshold(SDT) An intensity level at which a listener can barely discern the presence of a speech signal in 50% of the time It is equal to the PTA average obtained at 500,1000,2000Hz Speech Reception Threshold (SRT) Two syllabus words (Spondee) With different intensities The intensity at which 50% of the presented words can be repeated Measured in dB (it is usually 8-9dB more than SDT) Speech Audiometry Speech Discrimination Score (SDS) Mono syllable words At 50dB higher than SRT Percentage of words recognized correctly is noted • Normal: 96-100% • CHL: 90-100% • SNHL: low • Retro cochlear: very low Impedance Audiometry Objective test Includes : 1. Tympanometry 2. Acoustic Reflex 3. External Canal Volume (ECV) Tympanometry Record of resistance of conductive mechanism of ear against pressure changes of external canal 1. Type A: normal 2. Type B: OME, TM perforation, unfit probe, middle ear mass 3. Type C: Eustachian tube dysfunction 4. Type As: otosclerosis, tympanosclerosis 5. Type Ad: ossicular dislocation, or Atrophic TM 6. Type D: Scarred TM, or normal hypermobile TM Tympanometry Peak between -100 to +100 Tympanometry Peak usually in-150 to -200 Tympanometry Peak is under -300 Tympanometry Acoustic Reflex Stapedial muscle contraction in response to loud noise 70-100 dB above hearing threshold Particularly useful for DDx between Cochlear and Retrocochlear lesions Afferent : cochlear (8th) nerve Efferent : facial (7th)nerve Acoustic Reflex Absent bilaterally when tested ear has CHL BC must be better than 60dB to elicit this reflex AR negative in tested ear but + in the contralateral Retrocochlear lesion AR Positive in Ipsi., but negative in Contra. Brain Stem lesion It also demonstrate level of facial nerve lesion ABR Surface recording of the electrical activity of auditory pathway in response to sound Sensitive for Retro-cochlear lesion Wave Wave Wave Wave 1 & 2: cochlear nerve 3: cochlear nucleus complex 4: Superior olivery complex 5: lateral leminiscus Middle and Long Latency Response (MLR,LLR) Lateral lemniscus 5th ABR 3rd 1st and 2nd 4th Cochlear nucleus Sup. Olivary Complex ABR Oto-Acoustic Emission (OAE) Normal cochlea generate a sound Due to the biological activity of outer hair cells They are of 2 types: I. Spontaneous emission (Spont.OAE5070% of people) II. Evoked otoacoustic emission