Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
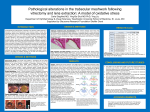
Change in anterior chamber depth following vitrectomy LI Yang1,YANG Chengxun1, QING Guoping1﹡and WEI Wenbin 1﹡ 1. Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University; Beijing Ophthalmology & Visual Sciences Key Lab, Beijing, China. ﹡ Correspondence to Wei Wenbin, MD, PhD, No. 1, Dongjiaominxiang, Dongcheng District, Beijing, 100730, China; Tel: 86-10-5826-9152, Fax: 86-10-5826-9157, E-mail: [email protected]; or Qing Guoping, MD, PhD; No. 1, Dongjiaominxiang, Dongcheng District, Beijing, 100730, China; Tel: 86-10-6717-2733, Fax: 86-10-5826-9930, E-mail: [email protected] Short running title: ACD change after vitrectomy Meeting presentation: none. The authors declare no conflict of interest. Financial support: the Beijing Municipal Health Bureau High-level Medical Professionals Promotion Project (No. 2009-3-32 and 2011-3-044) Word count: abstract 241; text 1720 Keywords: anatomy; anterior chamber depth; vitrectomy; A-scan ultrasound biometry 1 Abstract: Backgound: To characterize the short-term changes of anterior chamber depth (ACD) in eyes after vitrectomy by means of A-scan ultrasound. Methods: A prospective case series study was carried out on 29 eyes of 29 patients who underwent vitrectomy as the sole procedure. ACD was measured using A-scan ultrasound biometry shortly before vitrectomy and 1 week, 1 month, and 3 months after the surgery. Post-operative ACDs were compared with baseline. Results: Twenty-nine patients (16 males and 13 females) were enrolled for the study, with mean age of 50±11 (25-65) years. Twenty-three eyes of 23 patients were vitrectomized for vitreous hemorrhage (VH), and the other six were operated for idiopathic epiretinal membranes (ERM). The mean pre-operative ACD of the VH eyes was 2.98 ± 0.38mm, No significant difference was found between the ACD of the VH eyes and their fellow eyes (P=0.058). The average pre-operative ACD in the ERM eyes was 2.94 ± 0.31mm, which was statistically deeper than that (2.85 ± 0.28) of their fellow eyes (P=0.008). No statistical difference was found in the post-operative average ACDs of the VH eyes compared with baseline. In the ERM group, the post-operative ACD in the surgical eyes were still statistically deeper than the fellow eyes one week later after surgery (P=0.034). However, such statistical difference disappeared at the post-operative 1 month and 3 months (P=0.186 and 0.682). Conclusions: ERM may induce deepening of the ACD, which can be recovered by uneventful vitrectomy. VH does not cause shift of ACD, neither does vitrectomy. 2 Anterior segment morphometry is crucial for ophthalmologists to understand the visual outcomes of cataract surgery, keratorefractive surgery, as well as some other anterior segment disorders1-7. Anterior chamber depth (ACD) is one of the most significant and most widely used parameters among all measurements of the anterior segment2, 3, 8, 9. However, it is not always consistent. It changes with the position and thickness of the lens, angle status, and volume of the vitreous body10, 11. Better understanding of the changes of ACD following surgical treatment is not only beneficial for predicting visual outcomes of the treatment but also helpful to select appropriate surgical candidates. For example, gas tamponade in the vitreous cavity after vitrectomy may lead to shallowing of the anterior chamber and decrease in ACD, thus the surgeons should be more cautious to use gas tamponade in vitrectomy candidates with shallow anterior chamber12, 13. The crystalline lens is one of the most important and frequently measured structures in the eye ball1, 2, 4, 5, 14-17. It is stabilized centrally in the front globe by lens zonules at the circumference and hyaloideocapular ligament of Weiger at the posterior side. The right position and stabilization of the lens is important for good visual acuity14, 18-20. In vitrectomy, however, the Weiger’s ligament is removed with the vitreous as part of the procedure. As a consequence, the posterior support of the crystalline lens vanished after the surgery. Previous reports in literature have shown that ACD may shift slightly after vitrectomy7, 12, 13, 16, 21. As that fluid-air exchange, gas or silicone oil tamponade was not excluded in the surgery of these studies, which may lead to loose of the zonules, it was hard to conclude that the ACD change was a 3 result of vitrectomy and removal of the Weiger’s ligament. In this study, we want to address the over time changes of ACD following uncomplicated vitrectomy as the sole procedure. METHODS A prospective case series of 29 patients (16 males and 13 females) were enrolled for vitrectomy in our institution from 2011 to 2012. Twenty-three patients were diagnosed with vitreous hemorrhage (VH). The other six were identified as having epi-retinal membrane (ERM). Vitrectomy was performed using 23-gauge system shortly after a detailed ophthalmologic examination including VA, best corrected visual acuity (BCVA), intraocular pressure (IOP), slit lamp examination, dilated ophthalmoscopy, B-scan ultrasound, and posterior optic coherence tomography (OCT) if the vitreous body is clear. ACD was measured by means of A-scan ultrasound shortly before surgery with the patients in supine position, and was repeated at post-operative one week, one month, and three months. Each test was repeated 3 times. Accommodation was kept constant by asking the patient to fixate on a distant target while measuring the ACD. The inclusion criteria included a best-corrected visual acuity (BCVA) of less than 20/200 due to VH or ERM in the study eye on admission. The fellow eye was free of ocular diseases or disorders except for mild cataract formation or refractive error (< ±3.0 spherical equivalent diopters). The exclusion criteria included a history of ocular trauma, inflammation, intraocular surgery, laser peripheral iridoplasty or iridotomy, a ciliary cyst or tumor identified by B-scan ultrasound in anyone of the eyes, usage of nonexpansile gas at the end of the surgery, and age below 18 or above 80 years. 4 To avoid inter-personal surgical skill bias, the same doctor (Dr. WWB) performed the procedures in all included patients. Vitrectomy was performed using a 23-gauge system. At the completion of the procedure, tobramycin and dexamethasone ointment (Tobradex, Alcon) were instilled into the conjunctival sac before the eye was patched. Post-operative care included instillation of tobramycin and dexamethasone eye drops four times daily from postoperative days 1 to 28. Statement of Ethics This study was conducted in Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University, Beijing, after the institutional review board and ethics committee approved the study. All patients provided informed consent after detailed information about the procedure was performed. Primary Outcomes The follow-up examinations included VA, BCVA, IOP, slit lamp biomicroscopy, dilated ophthalmoscopy, and measurement of ACD by means of B-scan ultrasound in supine position. Postoperative ACD, VA, BCVA, and IOP were the primary outcome measurements. Statistical Analysis The means of post-operative ACD at post-operative one week, one month, and three months were compared to baseline with paired sample t-test. The average ACD of the study eyes was also compared to that of the fellow eyes. The significance level was set at 5%. All statistical analyses were done using Statistical Package for the Social Sciences 5 (SPSS) version 16.0 (SPSS, Chicago, IL, USA). RESULTS A consecutive case series of 29 (16 males and 13 females) patients were included in this study due to poor vision secondary to either VH or ERM, which required vitrectomy to improve visual acuity. The mean age of the patients was 50 ±11 (25-65) years. Twenty-three patients were diagnosed with VH (13 secondary to proliferative diabetic retinopathy, 10 with branch retinal vein occlusion). The other six were identified as having idiopathic macular ERM. All patients underwent uneventful vitrectomy after admission. Neither silicone oil nor scleral buckle was used at the end of vitrectomy. On admission, the average preo-perative ACD in the study eyes and the fellow eyes were 2.97±0.36 (2.15-3.09) mm and 2.89 ±0.33 (2.13-3.62) mm, respectively. In the VH eyes, the pre-operative ACD was 2.98 ± 0.38mm, which was not significantly different from that of their fellow eyes (2.89±0.33 mm, P=0.058). The average pre-operative ACD in the ERM eyes was 2.94 ± 0.31mm. It was statistically deeper than that of their fellow eyes (2.85±0.28mm, P=0.008). During the follow-up visits at one week, 1 month, and 3 months, the average ACD were 2.97±0.36, 2.96±0.34, and 2.93±0.36mm in the vitrectomized eyes, and 2.90±0.35, 2.93±0.36, and 2.93±0.37mm in the fellow eyes (Table 1). In the ERM group, the difference in average ACD between the study eyes and fellow eyes existed one week later after the surgery (P=0.034), but disappeared on post-operative one month and three months follow-up visits (P=0.186 and 0.682). In VH group, the 6 average ACD at post-operative one week, 1 month, and 3 months were 2.97±0.36, 2.92±0.34, and 2.93±0.36mm in the surgical eyes and 2.89±0.36, 2.90±0.38, and 2.91±0.36mm in the fellow eyes. No statistical significance was discerned between the average ACD between surgical eyes and the fellow eyes at any follow-up visits (P=0.059, 0.060, and 0.127) (Table 2). DISCUSSION In this study we have addressed the changes of ACD following uncomplicated vitrectomy as the sole procedure in VH and ERM eyes. The results demonstrated that idiopathic ERM may lead to deepening of the anterior chamber, and this increase of ACD can be reversed by vitrectomy. VH secondary to either PDR or retinal vein occlusion does not change the ACD, neither does uneventful vitrectomy. In previous studies in literature concerning ACD change after intraocular procedures, the conclusions were generally divided into two categories. One is that ACD increases obviously after cataract extraction and intraocular lens implantation1, 4, 15, 16, 22 . The other is that ACD fluctuate slightly following surgeries other than cataract surgery, mostly vitrectomy12, 13, 21, 23. In lens-sparing vitrectomy, the ACD does not shift obviously though different imaging method was used. One exception is that in threshold retinopathy of prematurity, the ACD deepened obviously after vitrectomy and the refraction shifted to more myopic24. In this study, we have measured pre- and post-operative ACD in 29 patients including 23 VH patients and 6 ERM patients who underwent uneventful lens-sparing vitrectomy. The post-operative ACDs are not statistically different with the baseline as a whole group, which indicates that 7 successful vitrectomy does not affect ACD and the status of the lens in supine position. The results were consistent with that of previous reports. However, when splitting the patients in two groups according to the diagnosis. The condition was different. In VH group, ACD did not change significantly as compared to that of their fellow eyes. The post-operative ACDs was neither statistically different from baseline as shown in the result section. Whereas in ERM group, the average pre-operative ACD was uniformly greater than that of the fellow eyes, which was statistically significant (p=0.034). This asymmetry persisted post-operatively until one month later after the surgery (p=0.186 and 0.682 for 1- and 3-month follow-up, respectively). These changes in ACD indicate that ERM may lead to deepening of the anterior chamber, and such increase in ACD can be reversed by vitrectomy. To the best of our knowledge, it has never been reported in literature that ERM eyes have deeper anterior chamber than their fellow eyes. In this study, however, we have found that the ACD in ERM eyes was unanimously and statistically deeper than that of the fellow eyes, which suggested that ERM formation may lead to backward move of the lens. Although the pathogenesis for idiopathic ERM is still not clear. It is widely accepted that the degree of visual dysfunction is highly associated with the thickness and contraction of the membrane. On the one hand, ERM contraction distorts and detaches the fovea centralis, resulting in marked loss of vision. On the other hand, the fovea centralis serves as a pivot, allowing ERM contraction to draw the vitreous backward, which in turn drags the crystalline lens posteriorly through the Weiger’s ligament. In lens-sparing vitrectomy, the Weiger’s ligament is removed with 8 abnormal vitreous. The adhesion on the posterior aspect of the lens disappears and allows rehabilitation of the anterior chamber after the procedure. This finding may be of clinical significance in that it revealed that ERM eyes may have a discounted anterior chamber after lens-sparing vitrectomy. The surgeons should pay more attention to the angle status of the surgical candidates with pre-operative narrow angles, especially when gas tamponade is considered at the end of the procedure12. The limitation of this study is that it is a small sample-size case series study. Among all enrolled patients, only six patients were identified as having idiopathic ERM. A large sample-size, well designed, prospective study is necessary before wide acceptance can be achieved. In summary, we have found for the first time that idiopathic ERM may lead to deepening of the anterior chamber, and this increase in ACD can be reversed by uneventful vitrectomy. VH secondary to either PDR or retinal vein occlusion does not cause shift of ACD, neither does lens-sparing vitrectomy. References: 9 1. Ahfat FG, Yuen CH, Groenewald CP. Phacoemulsification and intraocular lens implantation following pars plana vitrectomy: a prospective study. Eye 2003; 17: 16-20. 2. Byrne S, Ng J, Hildreth A, Danjoux JP, Steel DH. Refractive change following pseudophakic vitrectomy. BMC ophthalmology 2008; 8: 19. 3. Diaz Lacalle V, Orbegozo Garate FJ, Martinez Alday N, Lopez Garrido JA, Aramberri Agesta J. Phacoemulsification cataract surgery in vitrectomized eyes. Journal of cataract and refractive surgery 1998; 24: 806-809. 4. Grusha YO, Masket S, Miller KM. Phacoemulsification and lens implantation after pars plana vitrectomy. Ophthalmology 1998; 105: 287-294. 5. Iwase T, Sugiyama K. Investigation of the stability of one-piece acrylic intraocular lenses in cataract surgery and in combined vitrectomy surgery. The British journal of ophthalmology 2006; 90: 1519-1523. 6. Kumagai K, Ogino N, Demizu S, Shinjo U, Shioya M, Ueda K et al. Refraction and Anterior Chamber Depth Change After Vitrectomy for Pseudophakia. Japanese journal of ophthalmology 2001; 45: 115-116. 7. Park SP, Ahn JK, Lee GH. Morphologic changes in the anterior segment after phacovitrectomy for proliferative diabetic retinopathy. Journal of cataract and refractive surgery 2009; 35: 868-873. 8. Chalam KV, Gupta SK, Agarwal S, Shah VA. Sutureless limited vitrectomy for positive vitreous pressure in cataract surgery. Ophthalmic Surg Lasers Imaging 2005; 36: 518-522. 10 9. Falkner-Radler CI, Benesch T, Binder S. Accuracy of preoperative biometry in vitrectomy combined with cataract surgery for patients with epiretinal membranes and macular holes: results of a prospective controlled clinical trial. Journal of cataract and refractive surgery 2008; 34: 1754-1760. 10. Atchison DA, Markwell EL, Kasthurirangan S, Pope JM, Smith G, Swann PG. Age-related changes in optical and biometric characteristics of emmetropic eyes. Journal of vision 2008; 8: 29 21-20. 11. Zhou X, Qu J, Xie R, Wang R, Jiang L, Zhao H et al. Normal development of refractive state and ocular dimensions in guinea pigs. Vision research 2006; 46: 2815-2823. 12. Neudorfer M, Oren N, Barak A. High-frequency ultrasound biomicroscopy of the anterior segment morphometry before and immediately after pars plana vitrectomy. European journal of ophthalmology 2011; 21: 173-178. 13. Watanabe A, Shibata T, Ozaki M, Okano K, Kozaki K, Tsuneoka H. Change in anterior chamber depth following combined pars plana vitrectomy, phacoemulsification, and intraocular lens implantation using different types of intraocular lenses. Japanese journal of ophthalmology 2011; 54: 383-386. 14. Chang SW, Yu CY, Chen DP. Comparison of intraocular lens power calculation by the IOLMaster in phakic and eyes with hydrophobic acrylic lenses. Ophthalmology 2009; 116: 1336-1342. 15. Ha BJ, Kim SW, Kim SW, Kim EK, Kim TI. Pentacam and Orbscan II measurements of posterior corneal elevation before and after photorefractive 11 keratectomy. J Refract Surg 2009; 25: 290-295. 16. How AC, Baskaran M, Kumar RS, He M, Foster PJ, Lavanya R et al. Changes in anterior segment morphology after laser peripheral iridotomy: an anterior segment optical coherence tomography study. Ophthalmology 2011; 119: 1383-1387. 17. Marigo Fde A, Zisman M, Nehemy MB, Marigo PV. Ultrasound biomicroscopy in the comparison of the anterior segment morphometry before and after pars plana vitrectomy. Arquivos brasileiros de oftalmologia 2006; 69: 919-922. 18. Findl O, Kriechbaum K, Menapace R, Koeppl C, Sacu S, Wirtitsch M et al. Laserinterferometric assessment of pilocarpine-induced movement of an accommodating intraocular lens: a randomized trial. Ophthalmology 2004; 111: 1515-1521. 19. Ozkurt YB, Sengor T, Evciman T, Haboglu M. Refraction, intraocular pressure and anterior chamber depth changes after Nd:YAG laser treatment for posterior capsular opacification in pseudophakic eyes. Clin Exp Optom 2009; 92: 412-415. 20. Thornval P, Naeser K. Refraction and anterior chamber depth before and after neodymium: YAG laser treatment for posterior capsule opacification in pseudophakic eyes: a prospective study. Journal of cataract and refractive surgery 1995; 21: 457-460. 21. Stifter E, Menapace R, Luksch A, Neumayer T, Sacu S. Anterior chamber 12 depth and change in axial intraocular lens position after cataract surgery with primary posterior capsulorhexis and posterior optic buttonholing. Journal of cataract and refractive surgery 2008; 34: 749-754. 22. Damji KF, Chialant D, Shah K, Kulkarni SV, Ross EA, Al-Ani A et al. Biometric characteristics of eyes with exfoliation syndrome and occludable as well as open angles and eyes with primary open-angle glaucoma. Canadian journal of ophthalmology 2009; 44: 70-75. 23. Wang K, Yuan MK, Jiang YR, Bao YZ, Li XX. Axial length measurements before and after removal of silicone oil: a new method to correct the axial length of silicone-filled eyes for optical biometry. Ophthalmic Physiol Opt 2009; 29: 449-457. 24. Carvounis PE, Poll J, Weikert MP, Wilhelmus K, Lakhanpal RR, Holz ER. Refractive outcomes of lens-sparing vitrectomy for retinopathy of prematurity. Archives of ophthalmology 2011 ; 128: 843-846. 13 Table 1. Over time change in ACD following uneventful vitrectomy VH ERM VH & ERM preoperative 1 week 1 month 3 months 2.98±0.38 2.94±0.31 2.97±0.36 2.97±0.36 2.93±0.30 2.96±0.34 2.92±0.34 2.98±0.44 2.93±0.36 2.93±0.36 2.96±0.41 2.93±0.37 *Values of the mean anterior chamber depth (ACD)±standard deviation(mm) †VH=vitreous hemorrhage; ERM=epiretinal membrane 14 Table 2 Mean ACD following vitrectomy in both eyes during follow-up visits preoperative VH ERM VH & ERM study 2.98±0.38 2.94±0.31 2.97±0.36 1 week fellow 2.90±0.34 2.85±0.28 2.89±0.33 study 2.97±0.36 2.93±0.30 2.96±0.34 1 month fellow 2.89±0.36 2.91±0.33 2.90±0.35 *Values study 2.92±0.34 2.98±0.44 2.93±0.36 3 months fellow 2.90±0.38 2.99±0.44 2.93±0.36 study 2.93±0.36 2.96±0.41 2.93±0.37 of the mean anterior chamber depth (ACD)±standard deviation(mm) †VH=vitreous hemorrhage; ERM=epiretinal membrane 15 fellow 2.91±0.36 2.96±0.41 2.93±0.37