Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
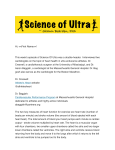
Europace (2004) 6, 222e228 Paroxysmal atrial fibrillation in male endurance athletes. A 9-year follow up Jan Hoogsteena,), Goof Schepb, Norbert M. van Hemelc, Ernst E. van der Walld a Department of Cardiology, Maxima Medical Centre, Dommelstraat Zuid 5, 5500 MB Veldhoven, Netherlands b Department of Sport Medicine, Maxima Medical Centre, Veldhoven, Netherlands c Department of Cardiology, Heart Lung Centre, Utrecht, Netherlands d Department of Cardiology, Leiden University Medical Centre, Leiden, Netherlands Submitted 13 May 2003, and accepted after revision 18 January 2004 KEYWORDS atrial fibrillation; endurance athletes Abstract Aims To study the course and circumstances of atrial fibrillation in endurance sports. Background Atrial fibrillation is the main cause of symptoms in athletes and frequently disturbs the performance during the practising of sport. The course of the arrhythmia is seldom reported in this population. Methods In 1993 and 2002 symptoms and clinical presentation of atrial fibrillation were evaluated in 30 well-trained athletes with a specially designed questionnaire. Results In 1993 paroxysmal atrial fibrillation was present in 30 male athletes at the mean age of 48:1 G 7:8, 3 (10%) of them also had paroxysmal atrial flutter. Three (10%) of the athletes died before 2002. In 2002 paroxysmal atrial fibrillation continued in 15 (50%) athletes, permanent atrial fibrillation emerged in 5 (17%) athletes and 7 (23%) of them showed no further atrial fibrillation. In 1993 paroxysms of atrial fibrillation started at a relatively low level of training intensity compared with the mean maximal training intensity of 11 G 7 versus 8 G 4 h=week (p ! 0:05). The first attack of adrenergically induced paroxysmal atrial fibrillation was more often present in younger athletes (p ! 0:005) and vagally induced paroxysmal atrial fibrillation was more apparent in older athletes (p ! 0:05). In 10 (38%) of the athletes a familiar form of paroxysmal atrial fibrillation was present. Conclusion A small proportion of the athletes (26%) was asymptomatic. Paroxysmal atrial fibrillation remained stable in half of the athletes whereas the arrhythmia changed into permanent atrial fibrillation in a minority of this population. ª 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved. ) Corresponding author. Tel.: D31-40-8888210; fax: D31-40-8888216. E-mail address: [email protected] (J. Hoogsteen). 1099-5129/$30 ª 2004 The European Society of Cardiology. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.eupc.2004.01.004 Atrial fibrillation in male endurance athletes Introduction In general practice atrial fibrillation (AF) is a very common arrhythmia. The incidence is about 0.5% in young patients (!40 years) and more than 5% in patients older than 65 years [1e3]. Atrial fibrillation is one of the most frequent causes of symptoms in athletes and often interferes with strong physical activities. In athletes the arrhythmia shows a prevalence of 0.2% [1]. Some recent data suggest that life-long endurance training may be arrhythmogenic [4], particularly in young male athletes [5e7]. Because the course of symptomatic paroxysmal AF in athletes who continue sporting activities is not well established, the management of the endurance athlete with this arrhythmia is unclear. Therefore, we developed a questionnaire to study the course of AF, the symptoms and relationship of the autonomic nervous system with this arrhythmia. The same group of athletes was asked to fill out the questionnaire both in 1993 and in 2002 disclosing the course of paroxysmal AF and detect possible mechanisms and circumstances of induction of AF. Methods Data collection By means of an advertising campaign in Dutch medical journals, general practitioners and cardiologists were asked to recruit athletes with electrocardiographically documented AF. Athletes were asked to fill out the questionnaire, which addressed medical history, course and level of sporting activities and therapeutic interventions for AF. Athletes with known causes of atrial fibrillation were excluded from the study. In addition, cardiac examination (Holter monitoring included) and results of other medical investigations to determine the cause of AF were retrieved from the cardiologist in charge. In 2002 the same group of athletes was asked again to fill out the same questionnaire. Height, weight and body surface area (BSA) of each athlete were determined. Definitions Athletic performance was defined as 50 min maximal running time for a 10 km circuit or a 90 min maximal cycling time for a 40 km distance. The symptoms caused by AF were categorized ‘‘most severe’’ when the arrhythmia forced an athlete 223 to discontinue sporting activity or daily duty or work, and/or led to hospital admission for treatment of AF. The symptoms were classified ‘‘moderate’’ when AF could be tolerated, normal daily functioning could be continued but sporting activity during atrial fibrillation had to be interrupted. The symptoms were labelled ‘‘mild’’ when sporting activity could be continued because AF was well tolerated. Lone AF was defined as presence of the arrhythmia without detectable heart disease or any other cause. Resting heart rate was assessed in the early morning just before getting up. Paroxysmal AF was defined as self-terminating AF with a duration varying from 10 min to 7 days, and permanent AF was defined as an ongoing arrhythmia despite therapeutic measures. Vagally induced AF was called AF occurring at night, after heavy meals or in the immediate hours after (intensive) exercise [7,18]. Adrenergically induced AF was defined as AF starting during daytime and provoked by exercise, stress or caffeine [7,18]. Overtraining is a mosaic pattern with parasympathetic and/or sympathetic components. Sympathetic overtraining is the condition defined by an elevated resting heart rate, loss of weight, disturbed sleep, elevated resting blood pressure, orthostatic hypotension, susceptibility to infection, and reduced performance. Parasympathetic overtraining is the condition characterized by a low resting heart rate, a tendency to hypoglycaemia, phlegmatic behaviour and reduced performance [25,26]. Statistical analysis Statistical analysis was performed with the 2 sample pooled t test for difference in means and unknown variances and the Chi-square test [9]. A value of p ! 0:05 was considered statistically significant. Results Athletes’ profile Thirty athletes responded in 1993 and 27 filled out the questionnaire in 2002. Seven athletes (23%) were medical practitioners. Female athletes could not be included due to lack of response to the advertising campaign. Between 1993 and 2002 height, weight, BSA and resting heart rate of the athletes did not change significantly (Table 1). The mean duration of sporting practice was 16:5 G 9:3 years. The mean age of the athletes at the first attack of symptomatic atrial fibrillation 224 Table 1 J. Hoogsteen et al. Anthropometrical characteristics of the athletes in 1993 and 2002 (means G SD) Number of athletes Age (years) Age of first complaint (years) Height (cm) Weight (kg) BSA (m2) Resting heart rate (bpm) 1993 2002 30 48.1 G 7.8 41.7 G 11.4 182.5 G 6.2 81.1 G 5.4 2.03 G 0.09 49 G 10 (n ¼ 25) 27 57.1 G 7.5 was 41:7 G 11:4; all athletes had more than 10 years of sporting practice at that time. The running time increased in 2002 by 15.9 min but the difference was not significant compared with 1993. The 40-km cycling time significantly increased by 19.4 min (p ! 0:005) (Table 2). Symptoms: onset and termination of atrial fibrillation In 1993 symptomatic paroxysmal AF was present in 29 athletes, of whom 3 (10%) also had paroxysmal atrial flutter. Only 1 athlete had asymptomatic AF (Fig. 1). Nine years later, symptomatic paroxysmal AF continued to occur in 15 (56%) athletes, in 7 (26%) athletes no symptoms of AF were observed, whereas in 5 (18%) athletes paroxysmal AF had evolved to become permanent. In 1993 almost all the athletes were treated medically with a single antiarrhythmic drug or with a combination of antiarrhythmic drugs: sotalol 37% (n ¼ 11), flecainide 20% (n ¼ 6), amiodarone 10% (n ¼ 3), digoxin 10% (n ¼ 3), quinidine 3% (n ¼ 1); in 2002, sotalol 30% (n ¼ 8), flecainide 22% (n ¼ 6), amiodarone 7% (n ¼ 2), digoxin 11% (n ¼ 3) in combination with a betablocker or verapamil. The familiar form of lone AF was apparent in 10 (38%) of the athletes. Training intensity at the time of the first attack of symptomatic AF in 1993 was significantly less than the maximal training intensity in hours per week (8 G 4 versus 11 G 7 h, p ! 0:05) (Fig. 2). During follow up 3 (10%) athletes underwent pacemaker implantations, 3 (10%) athletes underwent AF catheter ablative therapy and 3 (10%) athletes underwent Maze p 182.5 G 6.4 80.9 G 8.4 2.02 G 0.13 53 G 15 (n ¼ 22) ns ns ns ns surgery and were without symptoms postoperatively. All continued sport activity. Three (10%) athletes died between 1993 and 2002: 1 athlete in whom examination prior to this event had ruled out cardiac disease died suddenly. One athlete on warfarin therapy died from a cerebral haemorrhage, and 1 athlete, not anticoagulated, died from an ischaemic cerebral infarction. In 1993 and 2002 7 (23%) and 2 (7%) athletes, respectively, had symptomatic attacks of AF during maximal sporting activity, whereas 10 (33%) and 8 (30%) athletes in 1993 and 2002, respectively, had attacks of symptomatic AF only at night. A termination manoeuvre such as resting was successful in 2 (7%) and 6 (22%) athletes in 1993 and 2002, respectively, whereas a termination attempt such as sporting activity succeeded in termination of AF in 6 (22%) and 3 (11%) athletes in 1993 and 2002, respectively. A vagal manoeuvre to terminate AF was only successful in 1 athlete in 1993. It was not possible to terminate AF in 17 (57%) and 12 (44%) athletes in 1993 and 2002, respectively. Concerning symptoms due to AF: in 1993 12 (40%) and in 2002 16 (59%) athletes had mild symptoms allowing continuation of sporting activity, whereas in 1993 18 (60%) and in 2002 11 (41%) athletes had moderate or severe symptoms, requiring termination of all sporting activities (Table 3). Vagally induced atrial fibrillation Vagally induced AF was present in 1993 and 2002 in 10 (33%, n ¼ 30) and 10 (37%, n ¼ 27) athletes, respectively (Fig. 3; Table 3). The mean age, height, weight, BSA, weekly training schedule in Table 2 Athletic performance expressed as cycling time for a 40 km distance and running time for 10 km circuit (means G SD) Running Cycling Athletic performance 1993 Time (min) 2002 Time (min) p 10 km 40 km N ¼ 22 N ¼ 20 40.0 G 5.0 66.0 G 9.0 N ¼ 14 N ¼ 18 55.9 G 13.0 85.4 G 18.6 ns !0.005 Atrial fibrillation in male endurance athletes N=30 1993 Death N=3 225 Adrenergically and vagally induced atrial fibrillation in 1993 and 2002 2002 Number of athletes N=27 14 13 15 10 10 10 adrenergically 7 vagally 3 5 unclassified 0 1993 No symptoms N=7(26%) PAF N=15(55%) Chronic AF N=5(19%) Figure 1 Distribution of athletes with paroxysmal atrial fibrillation 1993e2002. hours and sporting activity over the years were not significantly different from the other athletes. The resting heart rate in the group with vagally induced symptomatic AF did not differ from the rest of the group with symptomatic AF; 48:2 G 9:6 bpm versus 47:1 G 9:0 bpm, respectively. In the group with vagally induced paroxysmal AF in 1993 (n ¼ 10), chronic AF became apparent in 2 athletes, 1 athlete became asymptomatic, 1 athlete died suddenly, and in 6 athletes vagally induced symptomatic AF persisted over the years (Fig. 4). In this group of 6 athletes there was a tendency for there to be a longer period of sporting activity (in years) in comparison with the rest of the group i.e. 22:7 G 6:6 versus 17:2 G 10:7 years but the difference was not significant. Adrenergically induced atrial fibrillation Hour / week Adrenergically induced AF occurred in 7 (23%) athletes in 1993 and in 3 (11%) athletes in 2002 (Fig. 3). These athletes were significantly younger than those with vagally induced AF and the other 20 18 16 14 12 10 8 6 4 2 0 Maximal intensity Intensity first attack of AF 8±4 N=30 n=29 Figure 3 Distribution of vagally, adrenergically and mixed triggers of atrial fibrillation. athletes: aged 40:4 G 8:2 versus 50:8 G 6:8 and 50:3 G 5:7, respectively (p ! 0:05 and p ! 0:005). The mean age of the athletes with the first symptomatic attack of adrenergically induced AF was significantly lower than that of the other athletes: aged 31:3 G 13:3 versus 46:6 G 6:6 (p ! 0:005). However, the age did not differ significantly from the group with vagally induced AF. Height, weight, BSA, years of sporting activity and the weekly training schedule (in hours) were not significantly different in the adrenergically induced AF group in comparison with the rest of the group. Of the 7 athletes with symptomatic adrenergically induced AF observed in 1993, paroxysmal AF continued in 5 athletes in 2002, in 3 athletes fewer or no symptoms of AF were noticed, and 1 athlete showed some progression in symptoms of the arrhythmia (Fig. 4). In only 1 athlete adrenergically induced AF changed into vagal AF; he became symptomfree after a Maze procedure. One athlete had an ischaemic cerebral vascular accident and died. One athlete stopped his sporting activity but the arrhythmia persisted. Adrenergically induced AF persisted in 3 athletes over a period of 9 years. Table 3 Symptoms and course of paroxysmal atrial fibrillation in athletes P<0.05 11±7 2002 Figure 2 Maximal training intensity in hours per week and training intensity at the first attack of atrial fibrillation. Asymptomatic Tolerable and continue sporting activity Stop sporting activity and normal function in day to day life Sick and not able to work Progressive illness and/or admission to hospital 1993 (N ¼ 30) 2002 (N ¼ 27) 1 11 10 6 12 9 4 2 2 226 J. Hoogsteen et al. Vagally induced atrial fibrillation 1993 N=10 PAF N=6 2002 Chronic.AF N=2 no AF N=1 Death N=1 Adrenergically induced atrial fibrillation N=7 1993 PAF N=5 2002 Figure 4 no AF N=1 Athletes with vagally and adrenergically induced paroxysmal atrial fibrillation 1993e2002. Atrial fibrillation, mental stress and relation with sport In 1993 20 (74%, n ¼ 27) and in 2002 15 (68%, n ¼ 22) athletes presumed a causal relationship between atrial fibrillation and mental stress (Table 4). In 1993 18 (67%, n ¼ 27) and in 2002 13 (59%, n ¼ 25) athletes had experienced a causal relationship of AF and sporting activity. Two athletes in 1993 and 2 athletes in 2002 benefited from sport for the termination of AF. Discussion This study aimed at disclosing the course, symptoms, inducing circumstances and dependency of the autonomic nervous system in 30 athletes with paroxysmal AF over a 9-year period. In half of the athletes paroxysmal AF continued, paroxysmal AF converted to permanent AF in 5 individuals and 7 athletes had no symptoms of AF. Two of the 3 athletes died from causes not directly related to AF. The mean age of the athletes with the first attack of atrial fibrillation was 41:7 G 11:4 and the training intensity at the time of the AF onset Table 4 Death N=1 was significantly lower than the maximal training intensity in their sporting careers. The majority of the athletes presumed a causal relationship between paroxysmal AF and both mental stress and sporting activity. Atrial fibrillation related to the autonomic nervous system Atrial fibrillation in young healthy athletes can be initiated by vagal or adrenergic predominance or their combined form [5,6,18] and all types can be associated with the overtraining syndrome. Interruption of training for a certain period of time could eradicate this overtraining syndrome [5]. It is reported that adrenergically induced atrial fibrillation is more common in subjects with structural heart disease [18] and therefore this type might be expected to occur more frequently in older athletes. Our study showed that vagally induced paroxysmal AF occurred in 10 (33%) and adrenergically induced paroxysmal AF occurred in 7 (23%) athletes. In contrast to the literature previously published, we observed that athletes with adrenergically induced paroxysmal AF were significantly younger than athletes with vagally The subjective causal relation of atrial fibrillation and sport activity Effect of mental stress 1993 2002 Relation to sport (subjective) 1993 2002 Improvement Indifferent Light arousal Strong arousal Unknown 0 7 11 9 0 0 7 7 8 4 Therapeutic Indifferent Light causal Intermediate causal Strong causal 2 7 12 3 3 2 10 8 3 2 N ¼ 27 N ¼ 26 N ¼ 27 N ¼ 25 Atrial fibrillation in male endurance athletes induced AF (p ! 0:05). Moreover, the first attack of paroxysmal AF emerged in athletes at a significantly earlier age than in other athletes (p ! 0:005). Mont [7] demonstrated that in the majority (72%) of the sporting individuals, he studied, with paroxysmal AF vagal dependency could be determined. This could not be confirmed in our study although the mean age of our athletes with a first attack of vagally induced AF did not differ from that in the study of Mont [7] (42:7 G 11:2 versus 39:5 G 13:2). The same holds for the years of sporting practice: (17:6 G 8:6, Mont [7] versus 23:7 G 10:9, in this study). Speculations on the mechanism of vagally induced AF involve cardiac adaptations characterized as the ‘‘athletic heart syndrome’’ [10e17]. Atrial dilatation and remodelling belong to this syndrome and reflect structural changes. One can assume that atrial dilatation progresses and at a certain level this benign adaptation to intensive sporting activities creates pathological changes leading to unfavourable fibrosis/collagen deposits, and sometimes to right atrial dysplasia [8]. These structural changes cause abnormal and heterogeneous conduction properties. Eventually, the enhanced vagal tone, promoting shortening of atrial refractory period, could serve as the trigger for the induction of AF in this abnormal atrial substrate. Mont [7] could not show any causal relationship between sporting activity and atrial dimension, but only 6 (19%) of his individuals were endurance athletes and the remainder performed other sports such as weight lifting, soccer and swimming. In addition, the mean left atrial dimension in the small group of endurance athletes with paroxysmal AF was within normal limits. Unfortunately, echocardiographic data were not sufficiently available for our study to elaborate this point. Atrial fibrillation and training intensity Long and intense periods of training could generate substantial shifts in body fluids due to changes in volume regulation, and changes in potassium and sodium levels. In these circumstances with high body temperature, hourly loss of 1 or 2 l of body fluids is not exceptional [19,20]. Inappropriate fluid intake can lead to dehydration triggering atrial arrhythmias [21]. In addition, long-lasting training schedules can induce a significant loss in magnesium and without proper supplementation, chronic hypomagnesemia can induce arrhythmias [22]. In our study the majority of the athletes presumed a causal relationship between paroxysmal AF and sporting activity. Thirty percent and 11% of the 227 athletes in 1993 and 2002, respectively, experienced reduction of attacks of AF by reducing sporting activity, but 43% and 52% of the athletes in 1933 and 2002, respectively, did not notice any relationship. Moreover, AF started at a relatively low level of training intensity compared with the mean and maximal training intensity (p ! 0:05) (Fig. 1), ruling out dehydration, hypomagnesemia or sympathetic and parasympathetic overtraining as a trigger for AF. Atrial fibrillation and heart disease In particular, adrenergically induced AF could be the first sign of heart disease. Forty percent of the athletes with WolffeParkinsoneWhite syndrome or a concealed atrioventricular bypass tract show periods of AF [23,24], the arrhythmia could manifest hypertrophic cardiomyopathy or arrhythmogenic right ventricular cardiomyopathy [5]. None of our athletes, including the 3 deceased individuals had overt cardiac disease. Limitations The study group had a small sample size and a selection bias due to the fact that only athletes with more serious symptoms of AF responded, of whom 23% were physicians being intrinsically more aware of rhythm disturbances. Because characteristics of AF were derived from the questionnaire, the true incidence of AF remains unclear, as AF can occur without symptoms and there could also be some overlap between the syndromes of vagally and adrenergically induced AF. In addition, it is possible that rate and irregularity of AF and thus, the awareness and tolerance of AF might have changed over the years. Conclusions This study showed that in half of the endurance athletes with paroxysmal AF this arrhythmia continued, whereas in a minority permanent AF became apparent. In only 7 of 30 athletes AF disappeared. A familiar form of atrial fibrillation was present in 10 athletes (38%). Vagally and adrenergically induced AF could be determined in 10 athletes (33%) and 7 athletes (23%), respectively. Sixty percent of vagally induced AF continued over the years. Adrenergically induced AF was clearly more often present in younger athletes than in older athletes. The majority of the athletes presumed a causal relationship between paroxysmal 228 AF and mental stress as well as sporting activity. Our study revealed that AF causes serious symptoms that disturb sporting activity and reduce exercise tolerance and hence more attention should be paid to preventing arrhythmia during endurance training. References [1] Furlanello F. Atrial fibrillation in top-level athletes. In: Olsson S, editor. Atrial fibrillation: mechanisms and therapeutic strategies. Armonk, New York, USA: Futura; 1994. p. 203e9. [2] Selzer A. Atrial fibrillation revisited. N Engl J Med 1982; 306:1044e5. [3] Godtfredsen J. Atrial fibrillation. Etiology, course and prognosis: a follow up study of 1212 cases. Thesis, University of Copenhagen, Munksgaard; 1975. [4] Jensen-Urstad K. High prevalence of arrhythmias in elderly male athletes with a lifelong history of regular strenuous exercise. Heart 1998;79:161e4. [5] Furlanello F. Atrial fibrillation in elite athletes. J Cardiovasc Electrophysiol 1998;9(Suppl):63e8. [6] Coumel P. Atrial fibrillation: one more sporting inconvenience? Eur Heart J 2002;23:431e3. [7] Mont L. Long-lasting sport practice and lone atrial fibrillation. Eur Heart J 2002;23:477e82. [8] Guiraudon C. The pathology of drug resistant lone atrial fibrillation in eleven surgically treated patients. In: Kingma JH, van Hemel NM, Lie KI, editors. Atrial fibrillation a treatable disease? Developments in cardiovascular disease, vol. 139. Dordrecht, Netherlands: Kluwer Academic Publishers; 1992. p. 41e57. [9] Douglas C, Montgomery G. Applied statistics probability for engineers. New York, USA: John Wiley; 1999. [10] Shapiro L. Morphologic consequences of systemic training. Cardiol Clin 1992;10:219e26. [11] Maron BJ. Structural features of the athlete heart as defined by echocardiography. J Am Coll Cardiol 1986;7: 190e203. J. Hoogsteen et al. [12] Bryan G. Athletic heart syndrome. Clin Sports Med 1992;11: 259e72. [13] George KP. The athletic heart syndrome. A critical review. Sports Med 1992;11:300e30. [14] Huston TP, Puffer JC, Rodney WM. The athletic heart syndrome. N Engl J Med 1985;313:24e32. [15] Levine B, Lane LD, Buckey JC, Friedman DB, Blomqvist CG. Left ventricular pressure volume and FrankeStarling relations in endurance athletes. Circulation 1991;84: 1016e23. [16] Galbo H. Endocrine factors in endurance. In: Shepard RJ, Åstrand P, editors. Endurance in sport. Oxford: Blackwell Scientific Publications; 1992. p. 116e26. [17] Hoogsteen J, Schep G, Huige MC, Hoogeveen A, Mosterd WL, Panhuyzen-Goedkoop NM. Atriumfibrilleren bij duursport. Cardiologie 1997;12:506e9. [18] Coumel P. Paroxysmal atrial fibrillation: a disorder of autonomic tone? Eur Heart J 1994;15(Suppl A):9e16. [19] Schep G. Eerste hulpproblemen bij triathlon en andere duursporten. Aard en omvang, risico inschatting, preventie en behandeling. Vlaams tijdschrift sportgeneeskunde. Sportwet 1993;54:101e26. [20] Sawka M. Effects of body water loss on physiological function and exercise performance. Perspectives in exercise science and sports medicine 1990;3:1e38. [21] Edwards JD, Wilkins RG. Atrial fibrillation precipitated by acute hypovolaemia. Br Med J (Clin Res Ed) 1987;294: 283e4. [22] McDonald R. Iron, zinc and magnesium nutrition and athletic performance. Sports Med 1988;5:171e84. [23] 26th Bethesda conference. Recommendations for determining eligibility for competition in athletes with cardiovascular abnormalities. Med Sci Sports Exerc 1994; 26(No 10 Suppl). [24] Al-Sheikh T, Zipes DP. Guidelines for competitive athletes with arrhythmias. In: Bayes de luna, Furianello F, Maron BJ, Zipes DP, editors. Arrhythmias and sudden death in athletes. Developments in cardiovascular disease. Dordrechti Kluwer Academic Publishers, 2000;232:119e51. [25] Lehman M. Trainingeovertraining. A prospective, experimental study with experienced middle- and long-distance runners. Int J Sports Med 1991;12:444e52. [26] Kuiper H, Keizer H. Overtraining in elite athletes. Review and directions for the future. Sports Med 1988;6:79e92.