Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
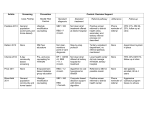
A 59F diagnosed with HTN 8 years ago comes to the clinic for BP check. She is currently taking HCTZ 25 mg/d, lisinopril 40 mg/d and amlodipine 10 mg/d. While she reports good compliance, she submits that her home BP ranges between 150-162/95-100 mmHg. She is also a diagnosed diabetic and is taking metformin. She has no other medications. The lowest BP in the clinic (after 3 measurements) is 155/90. Latest lab work showed normal kidney function. What is the best diagnosis for this patient’s condition? A. B. C. D. Essential HTN, well controlled Secondary HTN “Difficult-to-control” HTN Resistant HTN Define resistant HTN Identify etiologic factors Discuss treatment strategies and options Resistant HTN › failure to achieve goal BP › with maximum doses of 3 anti-HTN meds, including a diuretic, taken with good adherence › not synonymous with “uncontrolled” HTN › does not apply to recently diagnosed HTN Only 58% of treated hypertensives reach BP <140/90 mmHg Only <40% of patients with DM and CKD achieve good BP control Sarafidis and Bakris. J Am Coll Cardiol. 2008;52:1749-57. Increase BP by a mean of 5 mmHg Inhibit renal prostaglandin decrease renal blood flow sodium and fluid retention Also interfere with action of BP meds (except CCB) Large amounts (i.e. >3 drinks/day) have a dose-dependent effect on BP, in both hypertensive and normotensive people A 64M presents to the clinic for follow up; he has missed his last 2 appointments. Medical history is remarkable for HTN and OA of both knees. His medication list includes metoprolol 25 mg BID, losartan 50 mg/d, amlodipine 10 mg/d and hydralazine 50 mg QID and ibuprofen 800 mg TID. However, he cannot confirm taking all of them and adds that “my meds have been changed so many times”. Upon being told by the nurse that his present BP is 165/98 mmHg, he reports that his BP when taken at the pharmacy 4 months ago was 130/85. Physical exam is unremarkable aside from bilateral ankle pitting edema. What is the most appropriate diagnosis? A. B. C. D. Uncontrolled HTN Pseudo-resistant HTN Resistant HTN “Difficult-to-control” HTN Lack of BP control with appropriate treatment in a patient who does not have resistant HTN Sarafidis and Bakris. J Am Coll Cardiol. 2008;52:1749-57. Inadequate rest prior to BP check Taking single instead of triple readings Using cuffs that are too small Recent smoking Not fully holding arm at heart level (i.e. midpoint of the sternum while seated) Not baring the arm Back not supported and legs crossed Ambulatory BP reading (ABP) › Validated equipment › BP measured Q15-30 mins.; 50-100 total readings/24 hours › Mean daytime, nightime, 24-hr. BP › Approved for use by Medicare and Medicaid for suspected WCH › Evaluates diurnal BP rhythm • Nightime BP drops by at least 10% from daytime BP • Patients with non-dipping patern may be at increased risk for HTN complications • Nightime BP may be best predictor of CV risk Pickering ,et al. Circulation. 2005;111:697-716. Sarafidis and Bakris. J Am Coll Cardiol. 2008;52:1749-57. A 76F hypertensive presents for follow up. She was diagnosed approx. 15 years ago and has achieved good control (usual home BP =130/80 mmHg) with HCTZ 25 mg/d, diltiazem 180 mg BID and nifedipine XL 90 mg/d. She has no other medical conditions and takes her medications with good adherence. Vital signs are: BP 142/95 mmHg, HR 65 beats/min; the rest of her physical exam is unremarkable. Review of recent labs showed an estimated GFR of 38 mL/min (it was 50 mL/min about 1 year ago). What is the most appropriate treatment approach for this patient? A. B. C. D. Add lisinopril 10 mg/d Add metoprolol 25 mg BID D/C HCTZ and start bumetanide 1 mg/d Continue HCTZ and increase dose to 50 mg/d Sarafidis and Bakris. J Am Coll Cardiol. 2008;52:1749-57. Volume expansion is the most frequent pathogenetic finding in resistant HTN Diuretics can help >60% of patients achieve good control Note kidney function HCTZ: effective from doses of 12.5 mg/d (in normal kidney function); increases up to 50 mg/d may improve BP Chlorthalidone: 25 mg/d may be superior to HCTZ 50 mg/d; instant benefit Study: Switch from HCTZ to chlorthalidone resulted in 8 mmHg drop in SBP HCTZ > 50 mL/min Chlorthalidone = 40 mL/min Loop <40 diuretics mL/min Vasodilating BB may be added to 3-drug combo (if pulse rate not too low) May add complementary CCB to 3-drug combo with another CCB Adding ARB to ACE-I less effective than adding diiuretic or CCB; adding DRI results in small BP drop Adding spironolactone as 4th drug may lead to mean 25/12 mmHg reduction, especially in obese patients As 5th drug, consider cenrtal alpha-agonists (clonidine) or vasodilators (hydralazine or minoxidil) › No positive long-term outcome data Hirsch. Cleve Clin J Med. 2007;52:449-56. A 70M with resistant HTN is back in the clinic for close follow up. He also has PAD and well-controlled COPD. Since his diagnosis, medications have been added incrementally to include valsartan 320 mg/d, diltiazem 360 mg/d and HCTZ 50 mg/d. Other meds include ASA 81 mg/d, cilostazol 100 mg BID, fluticasone + salmeterol and tiotropium inhalers. His clinic and home BP readings are consistently between 145-151/9297 mmHg; HR is 85-90 beats/min. On exam, he has no JVD, rales or wheezes, and edema. Blood markers are within normal. What is the best treatment strategy? A. B. C. D. Start metoprolol 15 mg BID Start lisinopril 10 mg/d Start torsemide 10 mg/d Start amlodipine 5 mg/d Recognize resistant and pseudo-resistant HTN Check contributory factors, with emphasis on medications, diet (i.e. salt, alcohol) and patient adherence Perform a new physical exam at every visit Consider different and appropriate drug combinations Know when to refer