Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
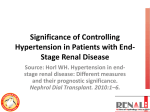
Nephrol Dial Transplant (1999) 14: 1976–1981 Nephrology Dialysis Transplantation Original Article Blood pressure variability as an adverse prognostic risk factor in end-stage renal disease Masahiko Tozawa1, Kunitoshi Iseki2, Shinichiro Yoshi3 and Koshiro Fukiyama1 1Third Department of Internal Medicine, and 2Dialysis Unit, University of The Ryukyus, 3Okinawa Dai-ichi Hospital, Okinawa, Japan Abstract Background. Prospective and case-control studies show that blood-pressure variability is an independent risk factor for severe organ damage and cardiovascular events in hypertensives. We prospectively studied the association between systolic blood pressure variability and cardiovascular mortality and mortality from all causes in end-stage renal disease patients. Methods and results. The subjects were 144 patients (86 men, 58 women; mean age±SD, 52±13 years) who underwent dialysis in the same dialysis centre and were examined for blood-pressure variability. The study period was 38 months beginning in January 1995, during which six cardiovascular and seven noncardiovascular fatalities occurred. Coefficient of variation in systolic blood pressure in 1994, as an indicator of systolic blood pressure variability, ranged from 7.8 to 14.6%. Cumulative incidence of death from all causes was related to coefficient of variation in systolic blood pressure. The difference between the maximum and minimum systolic blood pressure (DSBP) in 1994 ranged from 44 to 146 mmHg (mean±SD, 78±13 mmHg) and correlated significantly with coefficient of variation in systolic blood pressure (r= 0.65, P<0.0001). Cox regression analysis was used to identify the independent predictors for mortality. The hazard ratio for death from all causes increased 1.63 times per 1% increase in coefficient of variation in systolic blood pressure (hazard ratio; 95% confidence interval: 1.63; 1.05–2.53) and 1.03 times per 1 mmHg increase in DSBP (1.08; 1.03–1.14). Conclusion. These results suggest that systolic blood pressure variability may be a significant prognostic factor in end-stage renal disease. Key words: blood pressure; haemodialysis; kidney; risk factor; variability Correspondence and offprint requests to: Masahiko Tozawa MD, Third Department of Internal Medicine, University of The Ryukyus, 207 Uehara, Nishihara-cho, Okinawa 903–0215, Japan. Introduction The 1-year mortality rate for patients on dialysis in Okinawa, Japan between 1971 and 1990 was 11.6%, which was higher than that for the general population (0.45%). Cardiovascular and cerebrovascular diseases accounted for 45.1% of dialysis patient deaths [1]. Recent work suggest that blood pressure variability is a risk factor for cardiovascular complications in essential hypertension [2], and hypertension in the elderly [3] and a risk factor for complications in pregnant women [4]. The relation between blood pressure variability and prognosis of dialysis patients, however, has not been clarified. This study prospectively examines the association between systolic blood pressure variability and fatal events in patients with end-stage renal disease ( ESRD). Subjects and methods Subjects At the start of 1995, 144 patients who were undergoing regular dialysis three times per week in a single dialysis unit of Okinawa, Japan were selected. The subjects were 86 men (60%) and 58 women (40%) with a mean age of 52±13 years (range 22–83). This dialysis unit is one of those included in the Okinawa Dialysis Study (OKIDS) [1]. Some patients received dialysis in the morning and others received it in the evening; however, each patient always underwent dialysis in the same manner at the same time (morning or evening). The patients underwent dialysis three times a week in 4-h sessions. Haemodialysis was performed with a cellulose membrane (surface area 1.0–2.0 m2) and a dialysate containing 140 mEq/l sodium, 100 mg/dl glucose, 30 mEq/l bicarbonate, and 8 mEq/l acetate. During the follow-up period, the regimen was changed when a patient suffered from heart failure, pulmonary oedema or insufficient dialysis. The number of these cases were small and were usually associated with the end of life. The coefficient of variation in systolic blood pressure was calculated from complete patient records of 1994 (January to December) and all patients selected had been introduced to chronic haemodialysis therapy by the end of 1993. Some patients were given antihypertensive medicines. The © 1999 European Renal Association–European Dialysis and Transplant Association BP Variability and prognosis of ESRD time of their administration varied from patient to patient and several types of drug were used over the study period in different patients; however, the patients were encouraged to take their medicine at a set recommended time every day. Patients in this cross-sectional study were evaluated from 1 January 1995 to 28 February 1998 (38 months). We reviewed all medical records and registered the cases in the OKIDS. Baseline demographic data other than blood pressure were obtained in January 1994. Systolic blood pressure variability Immediately before each routine haemodialysis session, blood pressure was taken in the right or left arm with the patient assuming the supine position 5 min prior to measurement. These reading were performed by trained nurses or paramedical staff using a standard mercury sphygmomanometer. We previously verified the correlation between a single BP measurement and the 1-month average BP in the dialysis unit; the coefficient of correlation was 0.81 for one-point SBP and 1-month average SBP and 0.72 for 1-point DBP and 1month average DBP [5]. We used the coefficient of variation (CV: standard deviation/mean×100%) in systolic blood pressure as an indicator of systolic blood pressure variability. Coefficients of variation in SBP measured before the dialysis session were analysed from complete 1994 records which included 156 records per person. The difference between the maximum and minimum systolic blood pressure in 1994 (DSBP) was calculated in each patient and also used as an index of systolic-blood-pressure variability. Risk factors for vascular disease Diabetes mellitus defined in one of our previous reports [6 ]. Total cholesterol and other biochemical data were determined in January 1994. Stroke events Newly developed cerebrovascular disease was diagnosed by both clinical symptoms and brain CT scan. Brain CT scan was performed in all patients who were at risk for stroke. Causes of death Cause of death was confirmed from medical records. Classification of cause of death in dialysis patients was defined previously [7]. In this paper, we modified this classification as shown in Table 1. Statistical analysis Descriptive statistics are reported as frequency and percent for categorical data and as mean and SD or range for continuous data. Percentages were compared by x2 test. Student’s t-test was used to compare continuous variables. Cumulative incidence curves were compared with the logrank test. Cox regression analysis was used to evaluate the significance of risk factors for mortality due to cardiovascular events and to all causes. Significant risk factors for the model were chosen from a set of variables that included a coefficient of variation in systolic blood pressure, gender, age, smoking, diabetes, duration of haemodialysis, antihypertensive medication, systolic blood pressure, diastolic blood pressure, body weight gain between dialysis sessions, total cholesterol, serum 1977 Table 1. Causes of death in 13 patients during the follow-up period (1 January, 1995 to 28 February, 1998) Cardiovascular Stroke Cerebral haemorrhage Cerebral infarction Myocardial infarction Congestive heart failure Sudden death Withdrawal from dialysis Infection Other Total Smaller SBPCV range 7.8–10.1 n=72 Larger SBPCV range 10.2–14.6 n=72 1 0 0 0 0 1 0 1 3 1 0 0 3 1 2 1 2 10 SBPCV: coefficient of variation in systolic blood pressure. albumin, and serum creatinine. Hazard ratio and 95% confidence interval are reported. Statistical test results having a probability of <0.05 were considered statistically significant. Results The mean duration of follow-up was 35.2±8.1 months. Mean duration of haemodialysis was 87.5±60.0 months. Twenty-five (17%) patients were diabetic. Forty-five patients (32%) had a history of smoking (current or past) and 36 patients (26%) had a history of moderate to excessive alcohol consumption (current or past). Mean systolic and diastolic pressures were 144±15 mmHg and 77±7 mmHg respectively. Mean cholesterol concentration was 174±41 mg/dl. Mean albumin and creatinine concentrations were 3.8±0.3 g/dl and 14.1±2.9 mg/dl respectively. The coefficient of variation in systolic blood pressure, the mean was 10.2±1.5%, median was 10.1%, and range was 7.8–14.6%. The demographic data for patients in each half of the coefficient of variation in systolic blood pressure range are shown in Table 2. We subdivided the study population into two equal subgroups on either side of the median coefficient of variation in systolic blood pressure value. The demographic data of the two groups were compared univariately ( Table 2) and non-parametrically ( Figure 1). No significant differences in the prevalence of antihypertensive medication and erythropoietin therapy were found between the groups ( Table 2). In addition, there was no difference between the two groups with respect to the types of antihypertensive medication used ( Table 3). Systolic blood pressure variability and clinical outcomes Three (2%) of the 144 patients underwent renal transplantation during the follow-up period. By Cox hazards model, the hazard ratio can be analysed even when subjects are withdrawn for various reasons during the course of the study [8]. Therefore, we 1978 M. Tozawa et al. Table 2. Demographic and clinical characteristics of patients divided into two groups based on the coefficient of variation in systolic blood pressure Smaller SBPCV 9.0% (7.8–10.1%)a n=72 Age (years) Female (%) Duration of dialysis (months) Causes of renal failure (%) Chronic glomerulonephritis Diabetes mellitus Polycystic kidney disease Systemic lupus erythematosus Nephrosclerosis Miscellaneous Smoker (%) Alcohol consumer (%) Antihypertensive medication (%) Erythropoietin therapy (%) Body mass index (kg/m2) Systolic blood pressure (mmHg) Diastolic blood pressure (mmHg) DBW (kg) Total cholesterol (mg/dl ) Albumin (g/dl ) Creatinine (mg/dl ) 49±12b 32 93±61 81 10 0 3 3 3 39 26 67 71 22±3 146±12 78±6 2.1±0.7 172±44 3.8±0.2 14.6±2.8 Larger SBPCV 11.1% (10.2–14.6%)a n=72 P 55±13 49 82±59 0.013 0.061 0.291 62 25 3 0 4 6 25 26 63 78 22±4 142±17 75±8 2.0±0.7 177±38 3.7±0.3 13.4±2.7 0.016 0.028 0.476 0.476 0.999 0.677 0.082 – 0.727 0.445 0.827 0.101 0.023 0.198 0.524 0.106 0.001 aValues are median (range). bMean±SD. SBPCV: coefficient of variation in systolic blood pressure. DBW: body-weight gain between dialysis sessions. The coefficient of variation in systolic blood pressure was calculated from 156 records per person in 1994. Fig 1. Cumulative incidence of cardiovascular death ( left panel ) and death from all causes (right panel ) during the follow-up period for patients in the two SBPCV groups: lower half of the range and upper half of the range. The follow-up period was from 1 January 1995 to 28 February 1998. included the patients’ data when analysing the hazard ratio. Of the 144 patients, 13 (9%) died during the follow-up period. Causes of mortality in these patients are shown in Table 1 (6 cardiovascular and 7 noncardiovascular deaths occurred ). None of the patients suffered from myocardial infarction during the followup period. Patients in the group with the greater coefficient of variation in systolic blood pressure were more likely to develop a cardiovascular fatal event (5 of 72, 7%) than patients in the first half of the range (1 of 72, 1%; P=0.211). Cox regression analysis failed to show that coefficient of variation in systolic blood pressure is a significant independent predictor for cardiovascular mortality (adjusted hazard ratio; 95% confidence interval: 1.78; 0.94–3.37), but revealed that it is an independent predictor for mortality from all causes (1.63; 1.05–2.53) ( Table 4). DSBP ranged from 44 to 146 mmHg (mean±SD, 78±13 mmHg) and correlated significantly with coefficient of variation in systolic blood pressure (see Figure 2). One outlier in DSBP was identified statistically by Grubbs–Smirnov test. We excluded the patient’s data when analysing the hazard ratio of DSBP. Cox regression analysis failed to show that DSBP is a BP Variability and prognosis of ESRD 1979 Table 3. Types of antihypertensive medications used by the patients Calcium-channel blockers Beta blockers ACE inhibitors Centrally acting drugs Alpha blockers Smaller SBPCV range 7.8–10.1% n=72 Larger SBPCV range 10.2–14.6% n=72 P 38(53)a 22 (31) 6 (8) 3 (4) 2 (3) 35 (49) 22 (31) 10 (14) 1 (1) 0 (0) 0.738 — 0.426 0.612 0.476 aNumbers of patients (percentage) are shown. SBPCV: coefficient of variation in systolic blood pressure. Table 4. Cox regression analysis of cardiovascular mortality and mortality from all causes Parameter Cardiovascular mortality SBPCV (%) D SBP (mmHg) Mortality from all causes SBPCV (%) D SBP (mmHg) Crude hazard ratio (95% CI ) Adjusted hazard ratioa (95% CI ) 1.93 (1.16–3.21) 1.10 (1.04–1.16) 1.78 (0.94–3.37) 1.75 (0.82–3.73) 1.70 (1.20–2.41) 1.07 (1.03–1.11) 1.63 (1.05–2.53) 1.08 (1.03–1.14) aAdjustments were made for age, gender, duration of dialysis, diabetes, smoking habit, antihypertensive medication, systolic blood pressure, diastolic blood pressure, body weight gain between dialysis sessions, total cholesterol, serum albumin, and serum creatinine. CI, confidence interval; SBPCV, coefficient of variation in systolic blood pressure, DSBP, the difference between the maximum and minimum systolic blood pressure in 1994. diabetes, smoking, blood pressure, and cholesterol, which were risk factors for cardiovascular disease, and albumin, which has been shown to be a risk factor for death in patients with ESRD [9–12]. Other clinical factors such as duration of haemodialysis and antihypertensive medication used were also not significant. The cumulative incidence of cardiovascular death in the patients with the higher range of coefficient of variation in systolic blood pressure was greater than that for patients with the lower range, but the difference was not significant (P=0.092, see Figure 1, left panel ). The cumulative incidence of death from all causes for patients in the larger coefficient of variation in systolic blood pressure group was significantly higher than that for patients in the smaller coefficient of variation in systolic blood pressure group (P=0.039, see Figure 1, right panel ). Fig 2. Correlation between the difference between minimum and maximum systolic blood pressure in 1994 (DSBP) and the coefficient of variation in systolic blood pressure (SBPCV ). significant independent predictor for cardiovascular mortality (adjusted hazard ratio; 95% confidence interval: 1.75; 0.82–3.73), but revealed that it is an independent predictor for mortality from all causes (1.08; 1.03–1.14) ( Table 4). These results correspond to the hazard ratio for death from all causes, which increased 1.63 per 1% increase in coefficient of variation in systolic blood pressure and 1.08 per 1 mmHg increase in DSBP. No significant results were obtained for age, gender, Discussion This study extends previous analyses in case-control studies of hypertensives [2,3] and pregnant women [4] and shows prospectively that there is a relation between systolic blood pressure variability and mortality in patients with ESRD. A large number of papers [13–18] have described seasonal variation of blood pressure. Therefore we calculated the coefficient of variation in SBP from the complete year records of SBP in this study. We analysed coefficient of variation in systolic blood pressure but not coefficient of variation in diastolic blood 1980 pressure because SBP correlates better than DBP does with epidemiological end-points [19,20]. The incidence of acute myocardial infarction in dialysis patients in Okinawa, Japan was 1.1 per 1000 cases/year between April 1988 and March 1991 [21]; in other words, the rate was only 0.5 per 141 persons over 3 years. No myocardial infarction occurred in our study patients during the follow-up period, which was compatible with the statistics in Okinawa, Japan. Our method of BP sampling was different from those used in previous studies. Frattola et al. [2] and Ayala et al. [4] took hour-to-hour circadian blood pressure, Hata et al. [3] used month-to-month measurements for a year, and we took three measurements per week for a year. Although the BP sampling methods differed, all these reports showed a positive association between BP variability and adverse events. Determination of coefficient of variation in systolic blood pressure calculated from complete records of a full year of sessions may not be realistic for general use. Therefore, we introduced DSBP as an index of the variability of SBP and as an alternative to coefficient of variation in systolic blood pressure. Although the adjusted hazard ratio of DSBP is lower than that of coefficient of variation in systolic blood pressure for mortality from all causes, the hazard ratio is significant ( Table 4). This suggests that DSBP is a feasible, acceptable variable for predicting prognosis in endstage renal disease. Relative hypotension [22] and low diastolic blood pressure [23] are risk factors for mortality in dialysis patients. In our univariate and non-parametric analyses, patients whose coefficient of variation in systolic blood pressure was in the range above the median had lower DBP and a worse prognosis than those in the range below the median. Cox regression analysis with an adjustment for multiple factors, however, showed that DBP was not a significant risk factor. In previous studies with a short-term follow-up period, the effect of blood pressure on mortality was not found to be significant [9,24] which is agreement with our findings. Although the pathogenesis is not clearly understood, increased risk of cardiovascular disease is associated with recombinant human erythropoietin therapy for renal anaemia in chronic dialysis patients. This has been demonstrated in both retrospective [25] and prospective studies [26 ]. In our study, the percentage of patients using erythropoietin was not significantly different between the two groups. The mechanisms by which blood pressure variability increases the risk of mortality remains uncertain. One possible mechanism is that a change in the volume gain between dialysis sessions may affect blood pressure variability because the blood pressure of dialysis patients is largely volume dependent [27] and controlled by adequate dialysis [28]. In this study, bodyweight gain between dialysis sessions was taken into account during statistical analysis. This factor, however, was not different between the two groups and was not an independent risk factor for mortality by Cox analysis. Disorders of the autonomic nervous M. Tozawa et al. system may also be a possible factor in this situation because sympathetic overactivity is a common finding in end-stage renal disease and it correlates with the increase in both vascular resistance and systemic blood pressure [29]. Afferent signals from the kidney may be the mechanism for this overactivity [29]. However, all 144 patients in this study had end-stage renal disease. If a disorder of the autonomic nervous system was involved, the degree of disorder suffered by the patients should be different between the two coefficient of variation in systolic blood pressure groups, and this was not the case. Finally, sodium sensitivity also may be a mechanism that contributes to this relation because sodium sensitivity is an independent risk factor for cardiovascular events in essential hypertension [30] and the daily variability of sodium intake may influence the variability of blood pressure. Limitations of the present study include the relatively short duration of follow-up (38 months), the small patient numbers and the late stage in the entire course of dialysis treatment (average 80 months). An analysis of subsets such as elderly patients or patients in the early stages of dialysis could not be performed. All the patients survived while on haemodialysis through all of 1994 and, therefore, these patients may have a better prognosis than other ESRD patients. In summary, the present study suggests that patients with increased systolic blood pressure variability are more likely to develop fatal events. Further study is needed to establish methods of risk reduction. Acknowledgements. We acknowledge the secretarial assistance of Ms Chiho Iseki and the cooperation of other secretarial and nursing staff in Okinawa Dai-ich Hospital. References 1. Iseki K, Kawazoe N, Osawa A, Fukiyama K. Survival analysis of dialysis patients in Okinawa, Japan. Kidney Int 1993; 43: 404–409 2. Frattola A, Parati G, Cuspidi C, Albini F, Mancia G. Prognostic value of 24-hour blood pressure variability. J Hypertens 1993; 11: 1133–1137 3. Hata Y, Kimura Y, Fukiyama K et al. Predictors of cardiovascular accidents in elderly hypertensive patients with nested casecontrol study [Abstract]. Hypertens Res 1997; 20: 311 4. Ayala DE, Hermida RC, Mojón A, Fernández JR, Iglesias M. Circadian blood pressure variability in healthy and complicated pregnancies. Hypertension 1997; 30 [part 2]: 603–610 5. Tozawa M, Iseki K, Fukiyama K. Hypertension in dialysis patients: a cross-sectional analysis. Jpn J Nephrol 1996; 38: 129–135 6. Sunagawa H, Iseki K, Nishime K et al. Epidemiologic analysis of diabetic patients on chronic dialysis. Nephron 1996; 74: 361–366 7. Mailloux LU, Bellucci AG, Wilkes BM et al. Mortality in dialysis patients: analysis of the causes of death. Am J Kidney Dis 1991; 18: 326–335 8. Lagakos SW. Statistical analysis of survival data. In: Bailar J III, Mosteller F, eds. Medical Uses of Statistics. Massachusetts Medical Society, Boston, 1992; 281–291 9. Iseki K, Kawazoe N, Fukiyama K. Serum albumin is a strong predictor of death in chronic dialysis patients. Kidney Int 1993; 44: 115–119 10. Lowrie EG, Lew NL. Death risk in hemodialysis patients: The predictive value of commonly measured variables and an evalu- BP Variability and prognosis of ESRD 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. ation of death rate differences between facilities. Am J Kidney Dis 1990; 15: 458–482 Degoulet P, Legrain M, Reach I et al. Mortality risk factors in patients treated by chronic hemodialysis. Report of the Diaphane collaborative study. Nephron 1982; 31: 103–110 Acchiardo SR, Moore LW, Latour PA. Malnutrition as the main factor in morbidity and mortality, of hemodialysis patients. Kidney Int 1983; 24 [Suppl 16 ]: S199–S203 Imai Y, Munakata M, Tsuji I et al. Seasonal variation in blood pressure in normotensive women studied by home measurements. Clin Sci 1996; 90: 55–60 Woodhouse PR, Khaw KT, Plummer M. Seasonal variation of blood pressure and its relationship to ambient temperature in an elderly population. J Hypertens 1993; 11: 1267–1274 Jenner DA, English DR, Vandongen R, Beilin LJ, Armstrong BK, Dunbar D. Environmental temperature and blood pressure in 9-year-old Australian children. J Hypertens 1987; 5: 683–686 Khaw KT, Barrett-Connor E, Suarez L. Seasonal and secular variation in blood pressure in man. J Cardiac Rehabil 1984; 4: 440–444 Brennan PJ, Greenberg G, Miall WE, Thompson SG. Seasonal variation in arterial blood pressure. Br Med J 1982; 285: 919–923 Hata T, Ogihara A, Maruyama A et al. The seasonal variation of blood pressure in patients with essential hypertension. Clin Exp Hypertens [A] 1982; 4: 341–354 Kannel WB, Gordon T, Schwartz MJ. Systolic versus diastolic blood pressure and risk of coronary heart disease. The Framingham study. Am J Cardiol 1971; 27: 335–345 Tomita J, Kimura G, Inoue T et al. Role of systolic blood pressure in determining prognosis of hemodialyzed patients. Am J Kidney Dis 1995; 25: 405–412 1981 21. Iseki K, Kinjo K, Kimura Y, Osawa A, Fukiyama K. Evidence for high risk of cerebral hemorrhage in chronic dialysis patients. Kidney Int 1993; 44: 1086–1090 22. Foley RN, Parfrey PS, Harnett JD, Kent GM, Murray DC, Barre PE. Impact of hypertension on cardiomyopathy, morbidity and mortality in end-stage renal disease. Kidney Int 1996; 49: 1379–1385 23. Iseki K, Miyasato F, Tokuyama K et al. Low diastolic pressure, hypoalbuminemia, and risk of death in a cohort of chronic hemodialysis patients. Kidney Int 1997; 51: 1212–1217 24. Churchill DN, Taylor W, Cook RJ et al. Canadian hemodialysis morbidity study. Am J Kidney Dis 1992; 19: 214–234 25. Iseki K, Nishime K, Uehara H et al. Increased risk of cardiovascular disease with erythropoietin in chronic dialysis patients. Nephron 1996; 72: 30–36 26. Besarab A, Bolton WK, Browne JK et al. The effects of normal as compared with low hematocrit values in patients with cardiac disease who are receiving hemodialysis and epoetin. N Engl J Med 1998; 339: 584–590 27. Vertes V, Cangiano JL, Berman LB, Gould A. Hypertension in end-stage renal disease. N Engl J Med 1969; 18: 978–981 28. Charra B, Calemard E, Laurent G. Importance of treatment time and blood pressure control in achieving long-term survival on dialysis. Am J Nephrol 1996; 16: 35–44 29. Converse RL Jr, Jacobsen TN, Toto RD et al. Sympathetic overactivity in patients with chronic renal failure. N Engl J Med 1992; 327: 1912–1918 30. Morimoto A, Uzu T, Fujii T et al. Sodium sensitivity and cardiovascular events in patients with essential hypertension. Lancet 1997; 350: 1734–1737 Received for publication: 5.11.98 Accepted in revised form: 23.4.99