Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Population pharmacokinetic
analysis of sorafenib in
patients with solid tumours
Serge Guzy
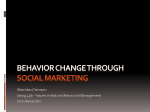
The PK Model
• The final PPK model was a one compartment model
with additional components describing the observed
absorption delay and underlying enterohepatic
circulation(EHC).
• The initial delay in quantifiable plasma concentrations
was adequately described by the GI transit
compartments absorption model. Four transit
compartments, each of them receiving drug from the
antecedent and releasing drug into the subsequent
The PK Model
• transit compartment with a first order rate constant
ka,accommodated the apparent lag time and a highly
variable tmax. EHC was modelled with a semimechanistic model, where a fraction of drug from the
central compartment (Fent) was hepatobiliary
excreted (transferred) into a
The PK Model
• gall bladder compartment with a first order rate kb,
which, in turn, periodically emptied drug into the last
GI transit compartment at a first order rate of kEhc.
For modelling purposes, Fent was logit transformed,
to constrain its value between 0 and 1, and to allow
typical parameters to be estimated as a continuous
function (–infinity to +infinity). The periodic drug
release from the gall bladder compartment was
regulated by the on-off switch ‘Ehc
The PK Model
• associated with use of discontinuous functions such as
step functions or lag times. t′ was the time of
emptying. At times less than t′, the value of EHC was 0
and the gall bladder did not empty and at times
greater than t′ the
The PK Model
• value of EHC was 1 and the gall bladder emptied. The
remaining fraction in the central compartment (1 –
Fent), was eliminated with a first order rate constant
of ke, reflecting hepatic metabolism and any
irreversible loss including the biliary loss which was
not recirculated; ke was parameterized in terms of
apparent clearance (CL/F) and volume of distribution
(V/F).
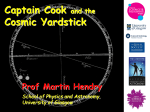
Structural Model
PML code for simulation: Structural
parameters definition
• mtt: The average time spent by sorafenib in travelling from the absorption compartments to the
central compartment (i.e.mean absorption transit time
• test(){
•
•
•
•
•
•
•
•
stparm(ktr=tvktr*exp(nktr))
fixef(tvktr=c(,2.53,))
ranef(diag(nktr)=c(0.1))
mtt = (ntr+1)/ktr
stparm(kehc=tvkehc*exp(nkehc))
fixef(tvkehc=c(,0.857,))
ranef(diag(nkehc)=c(0.1))
Fent
• Fent is the fraction of dose undergoing enterohepatic recirculation
• PML code: We need to constraint Fent between 0 and 1
• fent=ilogit(fentlogit)
• stparm(fentlogit=tvfent+nfent)
• fixef(tvfent=c(,0.0542,))
• ranef(diag(nfent)=c(0.1))
Number of transit compartments minus 1
• ke=Cl/V
• stparm(ntr=tvntr*exp(nntr))
•
• fixef(tvntr=c(,4,))
•
ranef(diag(nntr)=c(0.1))
Dose input (the “graph” parameters are used only
for initial estimates purposes), differential
equations
• Aagraph=Aa
•
ehcgraph=ehc
• transit( Aa, mtt, ntr, max = 50, out = -Aa * ktr )
•
deriv(A4=-ktr*(A4-Aa)+ehc*kehc*agb)
•
deriv(acc=ktr*A4-fent*ke*acc-(1-fent)*Cl/V*acc)
•
deriv(agb=fent*ke*acc-ehc*kehc*agb)
•
agbgraph=agb
•
a4graph=A4
•
accgraph=acc
EHC on off
fcovariate(dosageinterval)
# we assume that all patient have the same and unique dosage interval
# we are off for tlags then on until next dose
sequence{ while(1)
{ehc=0
sleep(tlags)
ehc=1
sleep(dosageinterval-tlags)
ehc=0
}
Dose input
•
•
•
•
•
•
•
•
•
• }
•
dosepoint(Aa)
C = acc / V
error(CEps = 1)
observe(CObs = C *(1+ CEps))
stparm(V = tvV * exp(nV))
stparm(Cl = tvCl * exp(nCl))
fixef(tvV = c(, 213, ))
fixef(tvCl = c(, 8.13, ))
ranef(diag(nV, nCl) = c(0.1, 0.1))
Input template data set
mapping
Output data set