Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
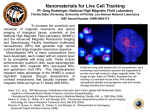
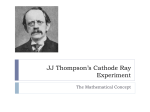
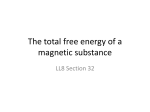
BJOG: an International Journal of Obstetrics and Gynaecology August 2004, Vol. 111, pp. 784 –792 DOI: 1 0 . 1 1 1 1 / j . 1 4 7 1 - 0 5 2 8 . 2 0 0 4 . 0 0 1 4 9 . x Comparison of ultrasound and magnetic resonance imaging in 100 singleton pregnancies with suspected brain abnormalities E.H. Whitby,a M.N.J. Paley,a A. Sprigg,b S. Rutter,c N.P. Davies,c I.D. Wilkinson,a P.D. Griffithsa Objective To compare the diagnostic accuracy of the current reference standard-ultrasound with in utero magnetic resonance imaging, in a selected group of patients. Design Prospective study. Setting Five fetal maternal tertiary referral centres and an academic radiology unit. Sample One hundred cases of fetuses with central nervous system abnormalities where there has been diagnostic difficulties on ultrasound. In 48 cases the women were less than 24 weeks of gestation and in 52 cases later in pregnancy. Methods All women were imaged on a 1.5 T clinical system using a single shot fast spin echo technique. The results of antenatal ultrasound and in utero magnetic resonance were compared. Main outcome measures The definitive diagnosis was made either at autopsy or by postmortem magnetic resonance imaging, in cases that went to termination of pregnancy, or a combination of postnatal imaging and clinical follow up in the others. Results In 52 of cases, ultrasound and magnetic resonance gave identical results and in a further 12, magnetic resonance provided extra information that was judged not to have had direct effects on management. In 35 of cases, magnetic resonance either changed the diagnosis (29) or gave extra information that could have altered management (6). In 11 of the 30 cases where magnetic resonance changed the diagnosis, the brain was described as normal on magnetic resonance. Conclusions In utero magnetic resonance imaging is a powerful tool in investigating fetal brain abnormalities. Our results suggest that in selected cases of brain abnormalities, detected by ultrasound, antenatal magnetic resonance may provide additional, clinically useful information that may alter management. INTRODUCTION The majority of women in the United Kingdom have detailed ultrasound imaging studies of their fetus at 18– 20 weeks after their last menstrual period. The ultrasound has several purposes, including detection of fetal anomalies. It follows that the information gained from imaging must be accurate in detecting the presence of an abnormality and must, within the limitations of the technique, be able to define the extent of the abnormality. Ultrasonography has many advantages over other imaging methods in as much as it does not use ionising radiation (unlike plain films or X-ray computed tomography), the images have high anatomical a Academic Unit of Radiology, University of Sheffield, UK Department of Paediatric Radiology, Sheffield Children’s Hospital, UK c Department of Obstetrics and Gynaecology, Jessop Wing, Sheffield, UK b Correspondence: Dr E. H. Whitby, Academic Unit of Radiology, University of Sheffield, Floor C, Royal Hallamshire Hospital, Glossop Road, Sheffield S10 2JF, UK. D RCOG 2004 BJOG: an International Journal of Obstetrics and Gynaecology resolution and are real time, which allows dynamic assessment of the fetus. Recent work using in utero magnetic resonance imaging has suggested that in some anatomical systems and disease processes magnetic resonance may have advantages over ultrasound.1 – 4 Our early work highlighted the likely usefulness of in utero magnetic resonance imaging in the clinical setting where there are difficulties or concerns over the antenatal ultrasound for detecting some brain and spine abnormalities.5 There have been few large studies, however, that have performed detailed follow up in order to confirm or refute the antenatal diagnoses and even fewer that have attempted to look at effects on clinical management. In this article, we compared the diagnostic capability of ultrasonography and in utero magnetic resonance imaging of 100 singleton pregnancies, referred from several tertiary centres, in which ultrasound has shown a possible brain abnormality. We obtained the relevant combinations of clinical investigations, postnatal imaging, autopsy and postmortem magnetic resonance imaging in order to produce a definitive diagnosis for the abnormality. In addition, we have attempted to judge the effect on clinical management made by performing in utero magnetic resonance. www.blackwellpublishing.com/bjog ULTRASOUND VERSUS MRI IN PREGNANCIES WITH SUSPECTED ABNORMALITIES 785 Table 1. A histogram and table showing the gestational age of 100 women at the time of in utero magnetic resonance imaging of their fetus in intervals of two weeks. Gestation 16/17 18/19 20/21 22/23 24/25 26/27 28/29 30/31 32/33 34/35 36/37 38/39 No. cases 1 3 18 26 15 4 7 9 7 4 7 3 METHODS The study was undertaken with the approval of the South Sheffield Ethics Committee. All the procedures were carried out after fully informed, written consent was obtained from the mother. Women were recruited from five fetal anomaly units in the North of England but all of the magnetic resonance studies were performed in Sheffield. All magnetic resonance examinations were performed within four days of referral from the obstetric ultrasonographer. In many cases, further ultrasound examinations and other investigations were made before referral to magnetic resonance. Fortyeight of the cases were imaged by magnetic resonance before 24 weeks (Table 1). The remainder were cases where the anomaly was detected by ultrasound later in pregnancy (21 cases were referred after 31 weeks of gestation) and in those cases the magnetic resonance examination was usually performed within two days of referral. All of the patients had abnormalities of the fetal brain reported or queried on the antenatal ultrasound examinations (but normal spines) and a provisional ultrasound report was available to the magnetic resonance reviewers (PDG, EW) at the time of the in utero magnetic resonance examination. All the ultrasounds were performed in fetal maternal speciality units using ultrasound machines used in their normal daily practise by either specialists in fetal maternal medicine or obstetric radiologists. The ultrasound report at the time of referral was used for comparison and no specific proforma was used. D RCOG 2004 Br J Obstet Gynaecol 111, pp. 784 – 792 All magnetic resonance examinations were performed on the same standard 1.5 T clinical system (Eclipse — Philips Medical Systems, with 27 mT/m gradients) using Single Shot Fast Spin Echo (SSFSE) sequences to produce highresolution T2-weighted images obtained in short scan times. The protocol consisted of twenty 5-mm-thick SSFSE images (TR 24,000 ms, TE 75 ms, echo train length 132, field of view 25 cm, matrix 212 256, acquisition time 20 seconds) obtained in the three natural, orthogonal planes. Those images were supplemented by twenty 3-mm-thick SSFSE images (TR 38,000 ms, TE 156 ms, echo train length 140, field of view 25 cm, matrix 256 256, acquisition time 30 seconds) acquired in the axial and sagittal planes. Neither maternal sedation nor muscular blockade of the fetus was performed in any of the cases. A report on the magnetic resonance examination was made within 24 hours of the magnetic resonance examination, which was prefixed by the fact that the magnetic resonance examination had been performed as part of a research study. In cases of apparent significant disagreements between ultrasound and magnetic resonance, the referring ultrasonographer was contacted as soon as possible and the in utero magnetic resonance findings were discussed. Corroboration of the anatomical abnormalities defined in utero was done by a variety of means appropriate to the clinical situation. All fetuses aborted or stillborn later in pregnancy had autopsy and/or postmortem magnetic resonance imaging. Postmortem magnetic resonance appears 786 E.H. WHITBY ET AL. Table 2. A histogram showing the number of cases falling into each of the outcome categories defined in the table below and in the text. Categories 3 and 4 include cases (35%) in which in utero magnetic resonance was judged likely to have had an effect on clinical management. In some cases, this was due to the in utero magnetic resonance detecting abnormalities not possible to detect by ultrasound for technical reasons. Group No. of cases 1. Magnetic resonance ¼ ultrasound 2. Magnetic resonance additional information 3. Magnetic resonance additional information that could have helped/altered management 4. Magnetic resonance changed the diagnosis 5. Ultrasound additional information to magnetic resonance 6. Magnetic resonance gave incorrect diagnosis to be a robust method of obtaining information on structural fetal CNS abnormalities.6,7 In cases where the pregnancy continued to term, postnatal clinical examination was performed along with appropriate neuroimaging. Autopsy information was obtained in the few cases that died in the neonatal period. From those definitive diagnoses, the cases were grouped into one of five categories depending on the antenatal ultrasound and in utero magnetic resonance findings: 1. Ultrasound and magnetic resonance gave comparable results and agreed with the final diagnosis. 2. The diagnosis was not fundamentally changed but magnetic resonance provided extra information that would not have affected management or counselling. 3. The diagnosis was not fundamentally changed but magnetic resonance provided extra information that could have affected management or counselling. 4. The diagnosis was changed on the basis of magnetic resonance imaging and found to be correct in the final analysis. 5. Any case in which ultrasound provided more information than magnetic resonance. 6. Magnetic resonance gave incorrect information. RESULTS The 100 fetuses reported here were taken from a group of 101 women referred for the study. We acknowledge that this is a selected group where there have been difficulties 52 13 6 29 0 0 establishing a definitive diagnosis at ultrasound for patient or technical factors. However, this is the group that in utero magnetic resonance will be used for in clinical practice (Table 4a and b). Weight range 50 – 135 kg, mean of 73.9 kg. The position of the fetus was variable as expected Table 3. Number of cases where the magnetic resonance and ultrasound were in agreement (Table 3a, group 1) or the additional information obtained from the ultrasound did not affect management (Table 3b, group 2). Categorised by referring diagnosis. a. Cases where the ultrasound and magnetic resonance were in agreement (Group 1). Suspected diagnosis or reason for referral Hypogenesis or agenesis of the corpus callosum Ventriculomegaly Cerebellar or posterior fossa abnormality Family history of previous fetal abnormality Microcephaly Other (includes abnormal shaped head, PROM, midline clefts, cortical dysplasia) No. of cases 4 19 6 8 5 10 b. Cases where magnetic resonance gave additional information, (Group 2). Abnormality Hypogenesis or agenesis of the corpus callosum Ventriculomegaly Cerebellar abnormality or posterior fossa abnormality Porencephalic cyst No. of cases 7 3 2 1 D RCOG 2004 Br J Obstet Gynaecol 111, pp. 784 – 792 ULTRASOUND VERSUS MRI IN PREGNANCIES WITH SUSPECTED ABNORMALITIES 787 Table 4. Antenatal ultrasound, in utero magnetic resonance and final diagnosis for each case where the in utero magnetic resonance provided clinically useful information (Table 4a, group 3) or changed the diagnosis (Table 4b, group 4). Case: Gestational age at imaging Antenatal ultrasound diagnosis In utero magnetic resonance diagnosis a. Cases where magnetic resonance provided clinically useful information (Group 3). 1: 21 Parietal encephalocoele Superficial arteriovenous malformation 2: 21 Isolated mild ventriculomegaly Ventriculomegaly, due to a germinal matrix haemorrhage 3: 24 Lobar Holoprosencephaly Septo-optic dysplasia, schizencephaly 4: 22 Interhemispheric cyst Agenesis of corpus callosum 5: 33 Calcified periventricular lesion Haemorrhage with ventriculomegaly 6: 22 Isolated mild ventriculomegaly Ventriculomegaly and absent septum pellucidum Final diagnosis: method As in utero MR: Histology As in utero MR: US As As As As in in in in utero utero utero utero MR: MR: MR: MR: PM MR US MR b. Cases in which in utero magnetic resonance were judged likely to have had a direct effect on clinical management which consists of cases where in utero magnetic resonance provided extra information to the antenatal ultrasound (Group 3, a) and cases where the diagnosis was changed by in utero magnetic resonance (Group 4, b). 7: 22* Isolated mild ventriculomegaly Ventriculomegaly, ACC and As in utero MR: PMMR, autopsy interhemispheric cyst 8: 21* Isolated mild ventriculomegaly Semilobar holoprosencephaly As in utero MR: autopsy 9: 35 Ventriculomegaly, ACC Ventriculomegaly, and periventricular As in utero MR: US leukomalacia 10: 36 Asymmetric ventriculomegaly Hemimegalencephaly As in utero MR: MR 11: 32 Isolated mild ventriculomegaly Ventriculomegaly and parenchymal As in utero MR: repeat US haemorrhage at 33 weeks 12: 36 Isolated mild ventriculomegaly Ventriculomegaly and Sinus thrombosis, As in utero MR: MR venous infarctions 13: 25* Talipes, normal brain Bilateral band heterotopia As in utero MR: autopsy 14: 21 Isolated mild ventriculomegaly Ventriculomegaly, ACC As in utero MR: MR 15: 36 Dandy-Walker malformation ACC, ethmoidal encephalocoele As in utero MR: MR 16: 30 Isolated ventriculomegaly Ventriculomegaly, Dandy-Walker Dandy-Walker, polymicrogyria: MR malformation 17: 24 Occipital encephalocoele Meningocoele, normal brain As in utero MR: clinical and MR 18: 22* Isolated mild ventriculomegaly Ventriculomegaly, Vein of Galen aneurysm As in utero MR: autopsy 19: 23* Isolated mild ventriculomegaly Ventriculomegaly, ACC As in utero MR: PMMR, autopsy 20: 23* Dandy Walker variant Dural fistula, massive torcula As in utero MR: PMMR, autopsy 21: 33* Isolated severe ventriculomegaly Ventriculomegaly, Ruptured arteriovenous As in utero MR: PMMR, autopsy malformation 22: 25 Isolated severe ventriculomegaly Ventriculomegaly, parenchymal Follow up US haemorrhage 23: 31* Isolated mild ventriculomegaly Ventriculomegaly, ACC As in utero MR: PMMR, autopsy 24: 20* Isolated severe ventriculomegaly Al lobar holoprosencephaly As in utero MR: PMMR, autopsy 25: 20 Isolated mild ventriculomegaly Normal Normal: Clinical and MR 26: 16 Isolated borderline ventriculomegaly Normal Normal: Clinical and MR 27: 36 Dandy-Walker malformation Normal Normal: Clinical and MR 28: 27 ACC Normal Normal: Clinical and MR 29: 29 Dandy-Walker malformation Normal Normal: Clinical and MR 30: 20* Small occipital encephalocoele Normal brain, scalp dermoid As in utero MR: MR and histology 31: 30 Dandy-Walker malformation Normal Normal: Clinical and MR 32: 32 ACC Normal Normal: Clinical and MR 33: 23 Frontal encephalocoele, Normal brain Normal Normal: Clinical and MR 34: 29 ACC, interhemispheric cyst Normal Normal: Clinical and MR 35: 31 Small frontal encephalocoele Normal Normal: Clinical and MR In these cases the in utero magnetic resonance was shown to be correct by the specified corroborative method: A ¼ autopsy; PMMR ¼ postmortem magnetic resonance imaging; CE ¼ clinical examination; MR ¼ postnatal magnetic resonance imaging; US ¼ follow up ultrasonography (in utero or postnatal). ACC in the diagnosis columns stands for agenesis of the corpus callosum. Mild ventriculomegaly 15 mm, severe ventriculomegaly 15 mm. * Patients had a termination of pregnancy. at different gestational ages. In three cases in the third trimester the unfavourable position of the fetus was partly responsible for the referral for magnetic resonance. In the second trimester, repeat ultrasound was used for unfavourable position of the fetus and this did not account for any D RCOG 2004 Br J Obstet Gynaecol 111, pp. 784 – 792 referrals for magnetic resonance unless there were additional uncertainties. One woman was claustrophobic and would not enter the scanner. The gestational ages of the 100 women at the time of magnetic resonance imaging are shown in Table 1. 788 E.H. WHITBY ET AL. Fig. 1. In utero magnetic resonance imaging of the brain at 20 weeks of gestation. (a) Ultrasound scan demonstrating the suspected occipital encephalocele. (b) Axial section in utero magnetic resonance and (c) parasagittal section SSFSE images show that the calvarium is intact and the brain is normal. There is a 6 mm swelling in the subcutaneous tissues in the occipital region (arrowed). At birth the region corresponded to a hairless patch on the scalp. The swelling was removed at 12 months of age after imaging confirmed no intracranial involvement and a diagnosis of a dermoid was made on histology (case 30, Table 4b). In utero magnetic resonance imaging produced examinations of good diagnostic quality in all cases. The median table occupancy time was 20 minutes; interquartile range 9 minutes (16 –25 minutes). Table 2 shows the distribution of cases into the six categories based on comparison of the results of antenatal ultrasound and in utero magnetic resonance with the definitive diagnoses. Groups 1 and 2 Table 3a and b summarises the findings of cases falling into groups 1 and 2. In 52 cases, the in utero magnetic resonance and antenatal ultrasound agreed (group 1) and in 51/52 those diagnoses agreed with the definitive diagnoses. In 1/52 both antenatal D RCOG 2004 Br J Obstet Gynaecol 111, pp. 784 – 792 ULTRASOUND VERSUS MRI IN PREGNANCIES WITH SUSPECTED ABNORMALITIES ultrasound and magnetic resonance demonstrated a DandyWalker malformation, confirmed ex utero, but did not detect the bilateral frontal polymicrogyria shown on postnatal magnetic resonance imaging (Fig. 3). In 13 cases, in utero magnetic resonance provided extra information over the ultrasound (all confirmed by the definitive diagnosis) but were judged not to have had any direct influence on clinical management (group 2). 789 Groups 3 and 4 Table 4a and b summarises the findings of groups 3 and 4 in which magnetic resonance was judged to have an effect on clinical management. Two cases are shown in Figs 1 and 2. In six cases, in utero magnetic resonance provided sufficient extra information to have had an effect on clinical management (group 3, Table 4a), all of which Fig. 2. This case is the only one of the 100 in which the in utero magnetic resonance did not show the full abnormality when compared with postnatal imaging. The fetus was scanned at 19 weeks of gestation and was reported as normal. The mother was re-examined at 30 weeks because of reduced movements. This showed the features of a Dandy-Walker malformation, which was confirmed on in utero magnetic resonance (a, b) and subsequently on postnatal imaging. (Dandy-Walker malformation: cystic dilatation of the fourth ventricle, enlarged posterior fossa and hydrocephalus). However, postnatal imaging showed bifrontal polymicrogyria (c) not shown on the antenatal ultrasound or in utero magnetic resonance. D RCOG 2004 Br J Obstet Gynaecol 111, pp. 784 – 792 790 E.H. WHITBY ET AL. Fig. 3. In utero magnetic resonance demonstrating agenesis of the corpus callosum. (a) Coronal section: the absence of the bridge between the two hemispheres. (b) Sagittal section: the corpus callosum is absent. were corroborated by the definitive diagnoses. In 29 cases, in utero magnetic resonance imaging changed the diagnosis (group 4, Table 4b), which were confirmed by the corroborative methods. In no cases did ultrasound show true positives that were not shown on magnetic resonance (group 5), or magnetic resonance provide an incorrect diagnosis (group 6). The diagnostic ability of in utero magnetic resonance, in cases where there were difficulties with the ultrasound, is high and in this population could have helped clinical management in 35% (groups 3 and 4). In 11 cases (in group 4), the ultrasound examination suggested possible brain abnormalities that were not con- firmed on in utero magnetic resonance or on the definitive diagnoses (cases 25 –35). In at least two of these cases the parents had decided on termination if the magnetic resonance confirmed the ultrasound findings. They continued the pregnancy after the magnetic resonance. DISCUSSION In this article, we have described our experience in evaluating a new magnetic resonance method designed to assess fetal brain abnormalities (in a selected group) against the D RCOG 2004 Br J Obstet Gynaecol 111, pp. 784 – 792 ULTRASOUND VERSUS MRI IN PREGNANCIES WITH SUSPECTED ABNORMALITIES current clinical reference standard — antenatal ultrasound. We previously reported the first 20 brain and spine anomalies performed in our unit using a similar, but lower resolution magnetic resonance method.5 In that article we showed disagreements between the magnetic resonance and ultrasound findings in 40% of cases and magnetic resonance was shown to be correct on detailed postnatal follow up. A number of criticisms could be made against that study, significantly, the women studied were comparatively late in pregnancy at the time of magnetic resonance. Ideally, we would like to be able to have the information before 24 weeks. There is no doubt that a biased population was investigated in the earlier study as the ultrasonographers referred their difficult cases that could exaggerate the possible benefit of magnetic resonance. In the present study, we have attempted to correct for some, but not all, of those shortcomings as well as increase numbers and improve our magnetic resonance methodology. Almost half (48) of the cases in the present study were imaged earlier than 24 weeks of gestation, one as early as 16 weeks. We do not advocate scanning that early based on our continuing experience and consider 20 weeks to be the earliest time that magnetic resonance can be performed reliably. Just over half of the cases (52) were imaged after 24 weeks in the present study. We have not been able to address the issue of selection bias in this study. A completely unbiased study would consist of performing magnetic resonance on every fetus who had a detailed anomaly ultrasound scan or at least all those where a brain abnormality was detected. This was not the case. The fetal anomaly experts referred cases where there were difficulties with the antenatal ultrasound for technical or patient related reasons. We would argue that the distribution of the problems in this study is a fair representation of those that would be referred if in utero magnetic resonance were available in clinical practice. The case for improved diagnostic ability in delineating CNS abnormalities by in utero magnetic resonance is compelling in this subgroup of patients, based on our results reported here and in the evolving related literature.8 – 10 In our present study, we have not been able to assess the direct effects of magnetic resonance on clinical management. The primary reasons for this was the ethical issue concerning use of data from a non-proven method (in utero magnetic resonance11) in a clinical setting. In this study, we can only report the effects the new technique might have on clinical management as observed by the authors and this could have introduced bias into the 35% of cases where management could have been altered by performing new in utero magnetic resonance technique. It is possible that a prospective study of independent fetal anomaly experts using an ‘intention-to-treat ’ basis may be the only way to eliminate this form of bias. However, the major differences between ultrasound and magnetic resonance reported in this study indicate that there is a role for in utero magnetic resonance in clinical practice. There are no known risks of D RCOG 2004 Br J Obstet Gynaecol 111, pp. 784 – 792 791 in utero magnetic resonance but it is essential that the specific absorption ratio (a measure of heat dissipation in the tissues) and number of sequences obtained is kept as low as possible. We need to further evaluate the role of in utero magnetic resonance in detecting brain malformations. We do not advocate that magnetic resonance should become the screening method for all pregnancies but should be reserved for further assessment of difficult suspected abnormalities defined by ultrasound. It is likely that the ultrasound diagnosis of isolated ventriculomegaly should be supplemented by in utero magnetic resonance. The observation that half of the cases listed in Table 4a and b were ultrasound diagnosed isolated ventriculomegaly and the range of true abnormalities described in in utero magnetic resonance attest that this is a group where in utero magnetic resonance is clinically very helpful and often diagnoses of the cause of ventriculomegaly was not apparent on ultrasound due to the limitations of the technique. Similarly for abnormalities of the posterior fossa or the corpus callosum (Fig. 3) as in utero magnetic resonance allows direct visualisation of structures in the midline in the sagittal plane. It is also likely that in utero magnetic resonance in the later stages of pregnancy will detect cortical abnormalities not possible to detected by ultrasound. In 11 of the 35 cases where magnetic resonance could have affected clinical management were ultrasound false positives (i.e. the brain was normal). It is not possible to conclude what would have been the outcome in these patients but we are aware that at least two were considering termination. It is likely that in some of the cases the referral was due to parental anxiety after an ultrasound abnormality was suggested even if a further examination had failed to confirm this, unfortunately, this information was not available to us and we have used the referring ultrasound reason in our analysis. Despite the bias and the above assumptions, we suggest that in cases where there are diagnostic difficulties at ultrasound due to patient size, gestational age, fetal lie and technical limitations in utero magnetic resonance should be considered. CONCLUSION In utero magnetic resonance is a tertiary referral centre technique where, if the diagnosis by ultrasound is restricted either by patient or by technical factors, additional information may be obtained that could influence patient management. In this study, we have shown that in such a subgroup of patients with CNS anomalies, in utero magnetic resonance provided additional information in 48%. Some of these findings may be inferred from the ultrasound but if confirmation is obtained by in utero magnetic resonance we may see benefits in patient management, reduction in parental anxiety and costly medico-legal cases may be avoided. 792 E.H. WHITBY ET AL. Acknowledgements The authors would like to thank SPARKS, Sir Jules Thorn and The United Sheffield Hospitals Special Trustees for financial support of EW and the project; the five referring hospitals, Leeds General Infirmary, The City Hospital Nottingham, Jessop Wing Sheffield, St Mary’s Hospital Manchester and Hull; the Radiographers at the University of Sheffield for scanning the patients; and Barbara Skevington for arranging appointments and sorting the paper work. References 1. Levine D. Ultrasound versus magnetic resonance imaging in fetal evaluation. Top Magn Reson Imaging 2001;12(1):25 – 38. 2. Levine D, Barnes PD, Edelman RR. Obstetric MR imaging. Radiology 1999;211(3):609 – 617. 3. Merzoug V, Ferey S, Andre C, Gelot A, Adamsbaum C. Magnetic resonance imaging of the fetal brain. J Neuroradiol 2002;29(2):76 – 90. 4. Levine D, Barnes PD, Madsen JR, Li W, Edelman RR. Fetal central 5. 6. 7. 8. 9. 10. 11. nervous system anomalies: MR imaging augments sonographic diagnosis. Radiology 1997;204(3):635 – 642. Whitby E, Paley MN, Davies N, Sprigg A, Griffiths PD. Ultrafast magnetic resonance imaging of central nervous system abnormalities in utero in the second and third trimester of pregnancy: comparison with ultrasound. Br J Obstet Gynaecol 2001;108(5):519 – 526. Griffiths PD, Variend D, Evans M, et al. Postmortem MR imaging of the fetal and stillborn central nervous system. AJNR Am J Neuroradiol 2003;24(1):22 – 27. Huisman TA, Wisser J, Stallmach T, Krestin GP, Huch R, Kubik-Huch RA. MR autopsy in fetuses. Fetal Diagn Ther 2002;17(1):58 – 64. Ertl-Wagner B, Lienemann A, Strauss A, Reiser MF. Fetal magnetic resonance imaging: indications, technique, anatomical considerations and a review of fetal abnormalities. Eur Radiol 2002;12(8): 1931 – 1940. Glastonbury CM, Kennedy AM. Ultrafast MRI of the fetus. Australas Radiol 2002;46(1):22 – 32. Levine D. Magnetic resonance imaging in prenatal diagnosis. Curr Opin Pediatr 2001;13(6):572 – 578. Stevenson DK, Goldworth A. Ethical considerations in neuroimaging and its impact on decision-making for neonates. Brain Cogn 2002; 50(3):449 – 454. Accepted 12 February 2004 D RCOG 2004 Br J Obstet Gynaecol 111, pp. 784 – 792