Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
American Journal of Epidemiology
Copyright O 1996 by The Johns Hopkins University School of Hygiene and Public Health
All rights reserved
Vol. 144, No. 1
Printed In L/.S.A
Correlation Between Systolic Blood Pressure and Physical Development in
Adolescence
Masazumi Akahoshi,1 Midori Soda,1 Randolph L. Carter,2 Eiji Nakashima,2 Katsutaro Shimaoka,1
Shinji Seto,3 and Katsusuke Yano3
Although the close relation between blood pressure and physical development in adolescence has been
established in cross-sectional and comparative cross-sectional studies, the entire trend of systolic blood
pressure (SBP) during adolescence has not been elucidated in conjunction with physical development in a
longitudinal study. Blood pressure (mmHg), body weight (kg), and body height (m) were measured annually for
418 subjects in Hiroshima and Nagasaki, Japan, from age 10 (1955 or 1956) through 18 years (1963 or 1964).
The Gompertz growth model was used to determine the velocity of weight increase (VEL) during that age
period. The relations between SBP from age 10 to 18 and VEL, weight, height, body mass index (BMI;
weight/height2, kg/m2), and the age at which the measurements were made were investigated individually
using random-coefficient growth-curve analysis. The SBP trend for the 10- to 18-year age period could be
shown by the following prediction equations: for the 163 Hiroshima males, SBP = 82.38 + 0.89 VEL at age
1.15 years prior to the current examination (VEL (age - 1.15)) + 1.40 BMI; for the 57 Nagasaki males, SBP =
92.70 + 1.07 VEL (age - 1.15) + 0.79 BMI; for the 148 Hiroshima females, SBP = 104.88 + 1.63 VEL (age
- 1.15) + 0.05 BMI; for the 50 Nagasaki females, SBP = 113.62 + 1.67 VEL (age - 1.15) - 0.59 BMI. VEL
1.15 years prior to the current examination was significantly and positively related to SBP in each city by sex
group (p < 0.01), and current BMI was significantly related to SBP for males in Hiroshima (p < 0.01) and nearly
so in Nagasaki (p = 0.06), but not for females in either city (p = 0.84 and 0.13, respectively). Because the plot
of VEL was a convex curve, SBP peaked approximately 1-2 years after the peak in VEL and then decreased
in both sexes. The entire SBP trend during adolescence can be expressed as an equation of VEL and BMI in
males and of VEL in females. SBP does not increase linearly with age. Am J Epidemiol 1996; 144:51-8.
adolescence; blood pressure; body mass index; body weight; growth
Cross-sectional studies have shown that adolescent
blood pressure is closely associated with body weight,
body mass index (BMI, weight/height2) and standing
height (1-6). Comparative cross-sectional studies conducted at intervals of several years to review the
relation between intervening changes in blood pressure and changes in weight and BMI have also shown
that the rate of weight (7-10) or BMI (11-15) increase
is positively related to the rate of blood pressure increase and is predictive of subsequent high blood
pressure. Thus, the level of blood pressure is related to
body size and the change in blood pressure to the
change in body size, suggesting the close relation
between adolescent blood pressure and physical development.
In many cross-sectional and comparative crosssectional studies, adolescent blood pressure is reported
to increase with age (16-20). In spite of the close
relation between blood pressure and physical development, however, the trends of blood pressure in these
studies were determined by plotting blood pressure
level, averaged across individuals, simply as a function of age without taking physical development into
consideration. Therefore, the question of whether or
not the blood pressure increase with age represents the
actual blood pressure trend naturally arises because the
degree of physical development and the age at spurt of
physical development differ among individuals (21).
To elucidate the blood pressure trend in view of
individual degree and trend of physical development,
we studied whether the entire blood pressure trend
during adolescence in individuals can be expressed as
Received for publication April 17, 1995, and accepted for publication October 25, 1995.
Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; SBP, systolic blood pressure; VEL, velocity of weight increase.
1
Department of Clinical Studies, Radiation Effects Research
Foundation, Nagasaki, Japan.
2
Department of Statistics, Radiation Effects Research Foundation, Hiroshima, Japan.
3
The Third Department of Internal Medicine, Nagasaki University
School of Medicine, Nagasaki, Japan.
Reprint requests to Dr. Masazumi Akahoshi, Department of Clinical Studies, Fiadiation Effects Research Foundation, 8-6 Nakagawa
1-chome, Nagasaki 850, Japan.
51
52
Akahoshi et a).
a function of weight, height, the BMI, and the velocity
of the weight increase (VEL) as an index of weight
increase in a longitudinal follow-up study. For this
purpose, we selected subjects whose blood pressure,
weight, and height had been measured annually from
ages 10 to 18 years and determined the individual VEL
for that period using the Gompertz growth model. We
then investigated the relation of blood pressure to
VEL, weight, height, BMI, and age individually
and annually from age 10 to 18 years by randomcoefficient growth-curve analysis and determined the
blood pressure trend using the prediction equation
obtained.
MATERIALS AND METHODS
The subjects were 509 individuals born in Hiroshima or Nagasaki between August 6, 1945 (Hiroshima) (or August 9, 1945 (Nagasaki)), and May 31,
1946, who were considered to have suffered no effects
of atomic bomb exposure because their mothers were
not in the city at the time of the bombing. The subjects
were examined at the Hiroshima or Nagasaki Radiation Effects Research Foundation (formerly the
Atomic Bomb Casualty Commission) annually on or
about their birthday starting at age 9 (1954 or 1955) up
to age 18 (1963 or 1964). Only data from age 10,
obtained after the subjects had become familiar with
the site and the examination procedure, were used.
Measurements of blood pressure, height, and weight
were included in the examination.
Standing height (m) was measured without stockings, and body weight (kg), with underwear. Blood
pressure (mmHg) was measured with a standard mercury sphygmomanometer (left arm, subject sitting).
One of two kinds of cuff was used depending on the
size of the upper arm. The first Korotkoff phase was
used for the systolic blood pressure (SBP).
The following steps were taken at each examination
to minimize the effects of the subject's emotional state
and to obtain basal blood pressure with the subject in
a relaxed state:
1. Subjects were transported to and from the clinic
by automobile.
2. They were examined in the same, quiet outpatient clinic each time, after a sufficient period of
sedentary waiting (at least 10-15 minutes after
arrival).
3. Blood pressure was measured by a pediatrician
with subjects in the sitting position after at least
5 minutes of rest.
4. The pediatrician assumed a calm attitude, which
helped the subject to relax.
Data for 422 subjects, who were examined four times
or more during the 9-year period, were analyzed.
STATISTICAL METHODS
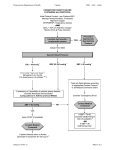
We used a double-exponential Gompertz model (table 1) for each of these 422 individuals to describe
mean weight as a function of age (22). The growth
dynamics of the model for a typical individual are
shown in figure 1. The first and second derivatives of
the resulting prediction equations were used to calculate the predicted velocity and acceleration of weight
increase at each age of measurement and at the lagged
ages. The nonlinear least squares procedure used to
estimate weight as a function of age failed to converge
for two individuals. Data for the remaining 420 individuals were used in random-coefficient growth-curve
analyses (23) to relate SBP to VEL, weight, height,
BMI, and chronologic age. Details for randomcoefficient growth-curve analyses are shown in the
Appendix. Because random-coefficient growth-curve
analysis fit 418 of the 420 subjects, the analysis was
based on the data for 418 subjects.
In figures 2-5, the correspondence between growth
dynamics and change in SBP during adolescence is
shown. The velocity and weight curves therein were
obtained from data pooled across individuals within
city by sex group. These pooled data were used in a
nonlinear regression analysis that ignored dependence
among within-individual observations to obtain a
Gompertz growth curve that described growth for a
typical individual in each group (figures 2-5). For our
purposes, least squares nonlinear regression analyses
by city and sex group were adequate.
TABLE 1. Gompertz growth model*
Growth
w = ft + &-***
Velocity
dw
—
Acceleration
d2w
— _
da1
_ -,
Zero at a = - /
the age of the maximum velocity of weight increase.
Third derivative
_ n
_
Zeroes at a = (0.96 - ft^fe and a = (-0.96 the ages of maximum and minimum accelerations of
weight increase.
* w, weight; a, age.
Am J Epidemiol
Vol. 144, No. 1, 1996
Adolescent Growth and Blood Pressure
53
Hiroshima Female
10
12
14
16
111
Age (years)
FIGURE 1. Weight (upper panel), velocity of weight Increase (middle panel), and acceleration of weight increase (lower panel) from
ages 10 through 18 years for a typical Individual, as determined by
the Gompertz growth model. The ages of the maximum velocity of
weight increase and maximum and minimum accelerations of
weight increase are shown.
RESULTS
Patterns of adolescent physical development and
changes in SBP for typical individuals in each city by
sex group are described by the equations in table 2.
VEL at age minus 1.15 years, VEL (a — 1.15), was
significantly positively related to SBP in each city by
sex group (p ^ 0.01). The BMI was significantly
related to SBP for males in Hiroshima (p - 0.0001)
and nearly significant in Nagasaki (p = 0.06), but was
not significant for females in either city (p = 0.84 and
0.13, respectively). SBP curves varied significantly
with the city by sex group. Significant main effects of
city (p = 0.0004) and sex (p = 0.0001) on SBP curves
were found overall. The city effect was due primarily
to the higher initial SBP in Nagasaki. The sex effect
was due primarily to a difference in the initial SBP
levels and to a difference in the effect of BMI on SBP
(p = 0.0001). The effects of lagged VEL on SBP for
Am J Epidemiol
Vol. 144, No. 1, 1996
FIGURE 2. Trends in systolic blood pressure (SBP) (upper panel),
velocity of weight increase (middle panel), and body mass index
(lower panel) from ages 10 through 18 years for a typical Hiroshima
female. The age of maximum velocity of weight increase is indicated. The SBP peaks approximately 1-2 years after the peak In
velocity of weight increase.
males and females differed only marginally (p =
0.06). The effect of VEL on changes in SBP during
adolescence appears to be relatively consistent across
the city-by-sex groups. The city-by-sex-interaction effects on the SBP curves were not significant (p >
0.23).
The relation between SBP and VEL during adolescence is illustrated by the city-by-sex groups in figures
2-5. The ages at which maximum VEL occurred for a
typical individual in each group are indicated. Because
BMI also affects change in the SBP, although not
significantly in females, the SBP peak is not exactly
1.15 years after the VEL peak; it is later than 1.15
years in males and in Hiroshima females because the
coefficient for BMI is positive, whereas, it is earlier
than 1.15 years in Nagasaki females because the coefficient is negative. In any case, SBP increases with
VEL, peaks approximately 1-2 years after the peak of
54
Akahoshi et al.
12
14
Age ( years )
Age (years )
FIGURE 3. Trends in systolic blood pressure (SBP) (upper panel),
velocity of weight increase (middle panel), and body mass index
(tower panel) from ages 10 through 18 years for a typical Hiroshima
male. The age of maximum velocity of weight increase is indicated.
The SBP peaks approximately 1-2 years after the peak in velocity of
weight increase.
FIGURE 4. Trends In systolic blood pressure (SBP) (upper panel),
velocity of weight increase (middle panel), and body mass index
(lower panel) from ages 10 through 18 years for a typical Nagasaki
female. The age of maximum velocity of weight increase Is Indicated. The SBP peaks approximately 1-2 years after the peak in
velocity of weight Increase.
VEL, and decreases thereafter. The decrease is greater
in females than in males, but this merely reflects the
influence of increasing BMI with age. Acceleration of
weight increase was not significantly related to SBP,
regardless of VEL. Thus, it appears that among the
potential explanatory variables studied, VEL 1.15
years prior to and BMI at the time of examination are
the most important factors related to changes in SBP
during adolescence.
consistent with the research results reported to date. A
number of cross-sectional and comparative crosssectional studies have shown that in adolescence levels
of weight and habitus are related to blood pressure
levels (1-4, 16), that changes in weight or habitus are
related to changes in blood pressure (7-14), but that
height was not related to blood pressure when weight
was taken into consideration (16, 24), and that age is
not a determinant of blood pressure in adolescence
even though blood pressure increases with age (7-11,
14).
Puberty is an important factor when discussing
blood pressure in adolescence. There is one report that
blood pressure is unrelated to sexual maturation or
menarche (25). However, Tell (26) reported that blood
pressure in both sexes is underestimated at ages 11-12
and overestimated at ages 15-16 if age is not corrected
DISCUSSION
By evaluating the relation between SBP and VEL,
weight, height, BMI, and age individually and annually for the ages of 10-18, we have shown for the first
time that the entire SBP trend for this age period is
expressible as an equation of VEL (a — 1.15) and BMI
in males and VEL (a — 1.15) in females. This is
Am J Epidemiol
Vol. 144, No. 1, 1996
Adolescent Growth and Blood Pressure
Nagasaki Male
21
20
it
u
10
12
14
16
IS
Age ( y e a r s )
FIGURE 5. Trends in systolic blood pressure (SBP) (upper pane)),
velocity of weight Increase (middle panel), and body mass index
(lower panel) from ages 10 through 18 years for a typical Nagasaki
male. The age of maximum velocity of weight increase is indicated.
The SBP peaks approximately 1-2 years after the peak In velocity of
weight increase.
for the sexual maturation stage. She recommended that
developmental age, assessed by the sex-maturity ratings formulated by Tanner, rather than chronologic
age, be used in epidemiologic studies of blood pressure in adolescence. Heredity also plays an important
role in adolescent blood pressure inasmuch as children
of parents with high blood pressure also have high
blood pressure (27-29). Neither puberty nor parental
blood pressure was included in die analysis reported
here, but these factors should be included in future
studies.
Another important finding in our study is that SBP
in adolescence does not increase linearly with age but
rather has a convex curve with a peak approximately
1-2 years after the peak of VEL. Many studies have
indicated that blood pressure in adolescence increases
with chronologic age (6, 16, 17, 30-33). This result,
however, comes mainly from cross-sectional studies
Am J Epidemiol
Vol. 144, No. 1, 1996
55
(6, 16, 32, 33) or comparative cross-sectional studies
(17, 30, 31) in which SBP levels, averaged across
individuals, were plotted as a function of age without
taking physical development into consideration, in
spite of the close relation between adolescent blood
pressure and physical development. However, Voors
et al. (4) reported the absence of an increase in SBP
with age when height was adjusted. Prineas et al. (5)
and Voors et al. (6) also reported that there is no
relation between blood pressure and age when BMI
and height are considered. Using the prediction equation obtained by evaluating the relation between SBP
and physical development individually, we demonstrated for the first time that SBP in adolescence does
not increase linearly with age but instead exhibits a
convex curve.
Because VEL contributed closely to the convex
curve of SBP, the biologic significance of SBP trend
observed in this study depends on the biologic significance of the VEL estimated by the Gompertz model.
VEL for females was 1.0-2.0 kg/year at 10 years old,
reached a maximum (5.0 kg/year) at 12.23 years old in
Hiroshima and at 12.36 years in Nagasaki, and decreased to 1.0 kg/year at 18 years old. VEL for males
was 0.5 kg/year at 10 years old, reached a maximum
(6.0 kg/year) at 13.35 years old in Hiroshima and at
13.57 years old in Nagasaki, and decreased to 1.0-1.5
kg/year at 18 years old. These results did not differ
from the trends of VEL reported to date: VEL for
females was 2.0-3.0 kg/year at 10 years old, reached
a maximum (5.0-6.0 kg/year) at 12.0-13.0 years old,
and decreased to 1.0-2.0 kg/year at 18 years old; and
VEL for males was 2.0 kg/year at 10 years old,
reached a maximum (6.0-7.0 kg/year) at 14.0-14.5
years old, and decreased to 1.0 kg/year at 18 years old
(34, 35). We consider, therefore, that the trends of both
VEL and SBP in this study have biologic significance.
Even if the SBP trend was determined in conjunction with physical development, we would not have
obtained the present results if the raw data of SBP used
for analysis had increased linearly with age. Shock
(36), who measured the blood pressure of 50 boys and
50 girls semiannually from age 11.5 to 17.5 years,
reported that SBP increased with age up to 14 years,
but not from age 14 to 16.5 in boys, and that it
decreased from age 14 to 15.5 in girls. His results are
consistent with ours in that they show that SBP does
not necessarily increase with age. Shock's study and
ours differ from other studies reported in the literature
in the following ways: 1) a fixed population was
followed for a long period, 2) blood pressure always
was measured at the same clinic, and 3) subjects were
brought to the clinic by automobile. It is important to
alleviate anxiety and to provide peace of mind when
56
Akahoshi et al.
TABLE 2.
Prediction equations for systolic blood pressure based on data from 10-18 year olds*
Standard deviation
Subjects
Equation
V E L ( a g e - 1.15)
Hiroshima females (n = 148)
Weight (kg)
SBP (mm Hg)
24.20 + e 3 ^
104.88 + 1.63 VELfage - 1.15) + 0.05(q)
0.26
0.23
Hiroshima males (n = 163)
Weight (kg)
SBP (mm Hg)
26.08 + a *
82.38 + 0.89 VEL{age - 1.15) + 1.40(q)
0.25
0.24
Nagasaki females (n = 50)
Weight (kg)
SBP (mm Hg)
24.48 + e ^ 3 113.62 + 1.67 VEL(age - 1.15) - 0.59(g)
0.45
0.39
Nagasaki males (n = 57)
Weight (kg)
SBP (mm Hg)
26.79 + e 3 - 5 3 - " - 0 4 " 8 *
92.70 + 1.07 VEL(age - 1.15) + 0.79(q)
0.42
0.41
• SBP, systolic blood pressure; VEL{age - 1.15), velocity of weight increase 1.15 years prior to examination; q, body mass index at the
time of examination.
measuring the blood pressure of children (18), and the
conditions that exist prior to blood pressure measurement should be uniform in the population and cohort
study. We believe that the facts that the subjects were
familiar with the site and examination procedure and
that physical activity before blood pressure measurement was calm and uniform also contributed to the
reliability of the data obtained.
The reported research results based on comparative
cross-sectional studies have shown consistently that
weight change is related to change in blood pressure;
a weight increase is associated with a blood pressure
increase and vice versa (7-14). Our results, however,
showed that SBP decreased even when weight increased, a possibility suggested by results of the longitudinal follow-up program of the Muscatine Study in
which 4,313 children were examined on three to six
occasions between 1970 and 1981 (13). Values for
blood pressure and body size (weight, relative weight,
height, and triceps skinfold thickness) were expressed
as percentile ranks, with a line describing changes in
the percentiles over time being calculated and the
slope of that line being defined as a trend. The authors
found a correlation between the average blood pressure rank and average body size rank, as well as
between the blood pressure trend and body size trend
percentiles, and suggested the importance of the relative rate of growth in establishing the rank order of
blood pressure. Although the authors did not discuss
absolute values, the possibility exists that blood pressure decreases with the decrease in percentile rank of
weight and that it exceeds the blood pressure increase
associated with the weight increase in cases in which
the absolute value of weight increases with age but the
percentile weight rank decreases.
Although not shown in Results, diastolic blood pressure (DBP) trends during adolescence could not be
expressed as an equation of VEL and BMI in males
and females in either city. In the present study, however, we encountered the following problem in DBP
measurements. Although the difference between mean
Korotkoff fourth phase (K4) and fifth phase (K5) DBP
is from 6.5 to 9.2 mmHg depending on the age of
children (37), from the beginning of the study it was
left to the discretion of the pediatrician whether to use
K4 or K5 as the indicator for DBP. It was reported
recently that reliable and repeatable blood pressure
measurements in childhood are best achieved with K5
as the indicator for DBP (37). Therefore, the evaluation of the relation between the entire DBP trend
during adolescence and physical development are left
for future studies using K5 as DBP.
In conclusion, the evolution of SBP in adolescence,
from 10 to 18 years of age, was determined from the
velocity of weight increase 1.15 years prior to current
measurement and the current BMI in males and by the
velocity of weight increase 1.15 years prior to current
measurement in females. In both sexes, SBP increased
approximately 1-2 years after the peak in velocity of
weight increase and decreased thereafter.
ACKNOWLEDGMENTS
This research was conducted at the Radiation Effects
Research Foundation (RERF), Hiroshima and Nagasaki,
Japan. RERF is a private foundation funded equally by
the Japanese Ministry of Health and Welfare and the US
Department of Energy through the National Academy of
Sciences.
Am J Epidemiol
Vol. 144, No. 1, 1996
Adolescent Growth and Blood Pressure
REFERENCES
1. Kotchen JM, Kotchen TA, Schwertman NC, et al. Blood
pressure distributions of urban adolescents. Am J Hygiene
1974;99:315-24.
2. Lauer RM, Filer LJ Jr, Reiter MA, et al. Blood pressure, salt
preference, salt threshold, and relative weight. Am J Dis Child
1976; 130:493-7.
3. Florey C du V, Uppal S, Lowy C. Relation between blood
pressure, weight, and plasma sugar and serum insulin levels in
schoolchildren aged 9-12 years in Westland, Holland. Br Med
J 1976;1:1368-71.
4. Voors AW, Webber LS, Frerichs RR, et al. Body weight and
body mass as determinants of basal blood pressure in
children—the Bogalusa Heart Study. Am J Epidemiol 1977;
106:101-8.
5. Prineas RJ, Gillum RF, Horibe H, et al. The Minneapolis
Children's Blood Pressure Study part 2: multiple determinants
of children's blood pressure. Hypertension 1980;2(Suppl I):I25-8.
6. Voors AW, Foster TA, Frerichs RR, et al. Study of blood
pressure in children, ages 5-14 years, in a total biracial
community—the Bogalusa Heart Study. Circulation 1976;54:
319-27.
7. Miall WE, Bell RA, Lovell HG. Relation between change in
blood pressure and weight. Br J Prev Soc Med 1968;22:
73-80.
8. Heyden S, Bartel AG, Hames CG, et al. Elevated blood
pressure levels in adolescents, Evans County, Georgia, sevenyear follow-up of 30 patients and 30 controls. JAMA 1969;
209:1683-9.
9. Kuller LH, Crook M, Almes MI, et al. Dormont High School
(Pittsburgh, Pennsylvania) blood pressure study. Hypertension
1980;2(Suppl I):I-109-16.
10. Visser MC, Grobbee DE, Hofman A. Determinants of rise in
blood pressure in normotensive children. J Hypertens 1987;5:
367-70.
11. Clarke WR, Woolson RF, Lauer RM. Changes in ponderosity
and blood pressure in childhood: the Muscatine Study. Am J
Epidemiol 1986; 124:195-206.
12. Mahoney LT, Clarke WR, Burns TL, et al. Childhood predictors of high blood pressure. Am J Hypertens 1991 ;4:
6O8S-1OS.
13. Lauer RM, Clarke WR, Beaglehole R. Level, trend, and variability of blood pressure during childhood: the Muscatine
Study. Circulation 1984;69:242-9.
14. Higgins MW, Keller JB, Metzner HL, et al. Studies of blood
pressure in Tecumseh, Michigan. II. Antecedents in childhood
of high blood pressure in young adults. Hypertension 1980;
2(SupplI):I-l 17-23.
15. Lauer RM, Burns TL, Clarke WR, et al. Childhood predictors
of future blood pressure. Hypertension 1991 ;I8(Suppl I):I74-81.
16. Londe S. Blood pressure in children as determined under
office conditions. Clin Pediatr 1966;5:71-8.
17. Zinner SH, Margolius HS, Rosner B, et al. Stability of blood
pressure rank and urinary kallikrein concentration in
childhood: an eight-year follow-up. Circulation 1978;58:
908-15.
18. Task force on blood pressure in children. Report of the second
task force on blood pressure control in children. Pediatrics
1987,79:1-25.
19. Uhari M, Nuutinen EM, Turtinen J, et al. Blood pressure in
children, adolescents and young adults. Ann Med 1991 ;23:
47-51.
20. Sanchez RG, Labarth DR, Forthofer RN, et al. National standards of blood pressure for children and adolescents in Spain:
international comparisons. Int J Epidemiol 1992;21:478-87.
21. Tanner JM. Growth at adolescence. 2nd ed. London, England:
Blackwell Scientific Publications, 1962.
22. Deming J. Application of the Gompertz curve to the observed
pattern of growth in length of 48 individual boys and girls
Am J Epidemiol
Vol. 144, No. 1, 1996
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
57
during adolescent cycle of growth. Hum Biol 1957;29:
83-122.
Vonesh EF, Carter RL. Efficient inference for randomcoefficient growth curve models with unbalanced data. Biometrics 1987;43:617-28.
Hofman A, Valkenburg HA. Determinants of change in blood
pressure during childhood. Am J Epidemiol 1983;117:
735-43.
Londe S, Johanson A, Kronemer NS, et al. Blood pressure and
puberty. J Pediatr 1975;87:896-9O0.
Tell GS. Cardiovascular disease risk factors related to sexual
maturation: the Oslo Youth Study. J Chron Dis 1985;38:
638-42.
Beresford SAA, Holland WW. Levels of blood pressure in
children: a family study. Proc R Soc Med 1973;66:1009-11.
Brandao AP, BrandiSo AA, Araujo EM. The significance of
physical development on the blood pressure curve of children
between 6 and 9 years of age and its relationship with familial
aggregation. J Hypertens 1989;7(Suppl I):S37-9.
Grobbee DE. Predicting hypertension in childhood: value of
blood pressure measurement and family history. J Am Coll
Nutr 1992;ll:S55-9.
Oberman A, Lane NE, Harlan WR, et al. Trends in systolic
blood pressure in the thousand aviator cohort over a twentyfour-year period. Circulation 1967;36:812-22.
Beaglehole R, Salmond CE, Eyles EF. A longitudinal study of
blood pressure in Polynesian children. Am J Epidemiol 1977;
105:87-9.
Szklo M. Epidemiologic patterns of blood pressure in children. Epidemiol Rev 1979; 1:143-69.
de Man SA, Andre1 JL, Bachmann H, et al. Blood pressure in
childhood: pooled findings of six European studies. J Hypertens 1991;9:109-14.
Tanner JM. Use Aid abuse of growth standards. In: Falkner F,
Tanner JM, eds. Human growth. Vol 3, 2nd ed. New York,
NY: Plenum Press, 1986:95-109.
Roche AF, Himes JH. Incremental growth charts. Am J Clin
Nutr 1980;33:2041-52.
Shock NW. Basal blood pressure and pulse rate in adolescents.
Am J Dis Child 1944;68:16-24.
Uhari M, Nuutinen M, Turtinen J, et al. Pulse sounds and
measurement of diastolic blood pressure in children. Lancet
1991;338:159-61.
APPENDIX
The random-coefficient growth-curve model is a
two-stage model. One stage describes responses (e.g.,
SBP) within an individual as a function of withinsubject covariates (e.g., velocity of weight increase
and BMI), and the other relates the coefficients of the
first stage to between-subject variables (e.g., city, sex).
Written in general form, the two stages are
= X.7; + eh
(1)
and
(2)
where y,- is the vector of repeated observations of the
response variable from the j 0 1 individual; X,, the matrix of observations of the within-subject explanatory
variables from the Ith individual; -y,, a column vector of
coefficients that relates the response to the explanatory
58
Akahoshi et a).
variables; y\, the row vector formed from y,\ Z'iy a row
vector of observations of the between-subject explanatory variables; A, the matrix of the parameters that
relate the random-coefficient vectors, y,., to the
between-subject variables, Z,; and et, and £, are
random-error variables. We assume that et are independently and identically distributed with a mean of 0
and a variance matrix of <x2/ and that £, are independently and identically distributed with a mean of 0 and
a variance matrix of ip.
The primary objective is to estimate A, the matrix of
parameters that relate the mean of the random coefficients, yt, to the between subject covariates, Z,, by use
of a two-stage estimation procedure. First, ordinary
least-squares regressions of yt on X; are performed
separately for each individual to estimate y, and of for
each i. Then, a2 is estimated as a pooled estimate from
&? and 4> from the individual estimates of y,. Next, A
is estimated by the multivariate linear regression technique using & and \\i. The prediction equation for y{ is
given by
Si = x,A r z,,
(3)
Initially, single-variable random-coefficient growthcurve models are fitted. (See Equations 1 and 2 for the
general definition of such models.) The X, matrices
are formed by concatenating a column of ones with a
column of weights, heights, BMIs, ages, VEL, and
VEL evaluated at 8 lagged ages chosen to determine
the best lag, 8. Of all the fits, the VEL evaluated at age
minus 1.15 produced the smallest pooled estimate of
a 2 (d-2 = 65.28); therefore, the VEL evaluated at age
minus 1.15 years was used in Equation 1. We do not
show the confidence interval of this lagged estimate
because there is no goodness of fit statistic (e.g.,
likelihood) for our method.
Random-coefficient models with two variables were
fit next for six choices of X, formed by [1, VEL (a), q],
[1, VEL (a - 1.15), q], [1, VEL (a - 1.15), h], [1,
VEL (a - 1.15), w], [1, VEL (a - 1.15), a], and (1,
a, a2), where 1 denotes a column of ones; VEL (x), a
column of VEL values evaluated at x; q, a column of
values of BMI; h, a column of heights; w, a column of
weights; and a, a column of ages at which the Ith
subject was observed. Models involving VEL (a —
1.15) all produced smaller pooled estimates for a2
than the two models without VEL (a - 1.15). The
mean coefficient on VEL (a — 1.15) in each of these
models was significant (p < 0.05) for each city by sex
group, but the coefficient of the third variable was
only significant in at least one city by sex group when
the third variable was BMI. Further model fitting
showed that no additional, fourth, variable was significant. We therefore fit the three-variable model with
X, = [1, VEL (a - 1.15), q] in the final analysis. This
model yielded d 2 = 59.19.
Am J Epidemiol
Vol. 144, No. 1, 1996