Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
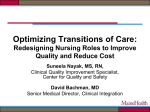
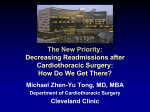
ORIGINAL RESEARCH Risk Factors for All-Cause Hospital Readmission Within 30 Days of Hospital Discharge Robin L. Kruse, PhD, Harlen D. Hays, MPH, Richard W. Madsen, PhD, Matthew F. Emons, MD, MBA, Douglas S. Wakefield, PhD, and David R. Mehr, MD, MS ABSTRACT • Objective: To develop a predictive model of 30-day readmission using clinical and administrative data. • Design: Retrospective cohort study. After dividing data into developmental and validation sets, multivariable logistic regression was performed. • Participants: Adults with data in Health Facts, a database composed of participating hospitals’ electronic medical records. The index hospitalization was a patient’s first qualifying hospital admission between 1 October 2008 and 31 August 2010. We excluded observation stays, admissions with length of stay of 0 days, obstetric stays, and patients whose predominant care setting was a psychiatric or rehabilitation unit. • Measurements: Readmission within 30 days of live discharge from the index hospitalization. • Results: There were 463,351 index admissions to 91 hospitals, with 45,098 (9.7%) patients readmitted. In multivariable modeling, factors associated with readmission included prior hospital admission, low hemoglobin, longer stays, and increasing Charlson index; arthroplasty procedures were associated with lower risk of readmission. Model discrimination was modest in developmental data (c-statistic = 0.668) and slightly lower (0.657) in validation data. • Conclusions: Increased comorbidity and prior hospital exposure are associated with unplanned readmission. Despite the availability of many potentially relevant clinical variables, model performance was modest and few clinical variables were associated with readmission in a multivariable model. Focusing on specific conditions with a narrower set of relevant variables may facilitate identifying patients at particularly high risk for readmission. H ospital readmission has gained increased attention both as a potential reflection of poor health care quality and as a cost driver. The www.jcomjournal.com Medicare Payment Advisory Committee estimated that readmissions resulted in $15 billion in Medicare expenditures annually [1]. The Patient Protection and Affordable Care Act (ACA) includes payment reductions for hospitals with high readmission rates to help control Medicare expenditures [2]. To improve care and avoid financial penalties, hospitals and clinicians need to optimize discharge planning and care coordination. This is particularly salient as health care networks position themselves as accountable care organizations [3]. Better understanding risk factors for readmission can help achieve these aims. Estimates of readmission rates vary widely, particularly by diagnosis and patient age. Among Medicare enrollees, 30-day readmission often exceeds 20%. For example, 25.7% of Medicare fee-for-service enrollees with heart failure were readmitted within 30 days [4] compared with 19.6% of patients in a general Medicare fee-forservice sample [5]. Readmission rates for Medicare fee-for-service patients with pneumonia, heart failure, or myocardial infarction all exceeded 21%, with AfricanAmerican patients and patients in minority-serving hospitals readmitted more often [6]. Other populations also experience high readmission. In a general population of heart failure patients discharged from a single, urban hospital, 24.2% were readmitted within 30 days [7]. Readmission following radical cystectomy for bladder carcinoma was 19.7% in the first 30 days [8]. Given the magnitude and variation in readmission rates, substantial effort has been directed at determining factors that are associated with readmission. A recent review of 26 models [9] reported that most performed poorly. Nine US studies of large population-based data- From the University of Missouri School of Medicine, Columbia, MO (Drs. Kruse, Madsen, Wakefield, and Mehr) and Cerner Corporation, Kansas City, MO (Mr. Hays and Dr. Emons). Vol. 20, No. 5 May 2013 JCOM 203 RISK FOR READMISSION bases or multicenter studies, mostly involving Medicare data or older patients, had c-statistics of 0.55 to 0.65 (the c-statistic varies from 0.5 to 1.0, where 1.0 indicates perfect fit and 0.5 represents results no better than a coin flip). Ross and colleagues [10] reviewed 117 studies of readmission following hospitalization for heart failure and found few patient characteristics consistently associated with readmission. Two models were reported, both with poor discrimination (c-statistic 0.60 for both). Claims data have been extensively used to study readmission; they typically include demographic characteristics, diagnoses and procedures, and insurance information but lack other clinical data that might identify patients during a hospital stay who are at high risk of readmission. Factors such as the use of high-risk medications, critical care exposure, laboratory abnormalities, organ dysfunction, and severity of illness indicators might be more powerful predictors of 30-day readmission than diagnosis. Though often unavailable in claims data, these variables are readily available in electronic health records. We analyzed the Health Facts database (Cerner Corporation, Kansas City, MO), electronic health data aggregated from numerous health systems, to provide insight into additional factors associated with hospital readmissions. Our overall objective was to create a predictive model for all causes of 30-day hospital readmission using variables pertaining to the index hospitalization available at the time of discharge. We considered characteristics of the entire index admission because our focus was risk of future readmission. By relying on data from electronic health records, the model could be refined and embedded in an electronic health record to inform discharge planning. METHODS Using a retrospective cohort design, we identified adults with an acute care hospitalization (index admission) and determined which patients had an inpatient readmission within 30 days following discharge. We compared patients who were and were not re-hospitalized to determine risk factors for readmission. The Health Sciences Institutional Review Board at the University of Missouri deemed the study exempt from review. Health Facts Database We used Health Facts, a database assembled from participating hospitals and health systems’ comprehensive clinical records. Health Facts has been used in several studies 204 JCOM May 2013 Vol. 20, No. 5 of acute myocardial infarction (AMI) outcomes [11–14] as well as surveillance of meningococcal disease in children [15]. Billing and encounter data are integrated with clinical information relating to drug order/dispensing and the results of diagnostic testing. Data are submitted from diverse hospitals and outpatient clinics throughout the United States. Depending on the specific electronic health record components implemented in each facility, different data elements are contributed to Health Facts. Cerner Corporation has established Health Insurance Portability and Accountability Act (HIPAA)–compliant policies and procedures that use statistical methods to deidentify data prior to inclusion in Health Facts. Because patients are de-identified when hospitals contribute their data, readmissions can only be tracked within the same health system. However, in Medicare data, 78% of readmissions are to the same hospital [16]. Inclusion and Exclusion Criteria We included inpatient admissions with at least 1 of each of the following: diagnosis or procedure, medication order, and laboratory order. The index hospitalization was the first qualifying acute care hospital admission for a patient between 1 October 2008 and 31 August 2010. We included patients who were at least 18 years of age at admission and who were discharged alive. We excluded the following: (1) admissions with a length of stay of 0 days; (2) outpatient (observation) stays; (3) patients with primary or secondary diagnosis of pregnancy or complications of pregnancy, childbirth and the puerperium (International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9-CM] diagnosis codes 630–679) or who had primary or secondary procedures that were obstetrical (ICD-9-CM procedure codes 72–75); and (4) patients whose predominant care setting during the admission was a psychiatric or rehabilitation unit. After reviewing distributions of medication orders, we operationalized predominant care setting as a psychiatric or rehabilitation unit if more than 90% of the medication orders originated from that type of unit. We included patients with psychiatric conditions requiring temporary acute care not excluded by the above criterion, such as alcohol detoxification, drug detoxification, or stabilization following a suicide attempt. We did not consider elective admissions following the index admission as readmissions. Elective (planned) readmissions were those so designated by the admitting physician except when the patient was admitted through the emergency departwww.jcomjournal.com ORIGINAL RESEARCH ment. Admissions within 24 hours of discharge from the index admission were combined with the index admission and treated as 1 admission (most were within 3 hours and not likely true discharges). Analysis We used SAS for Windows, version 9.2 (SAS Institute Inc., Cary, NC) for all analyses. Potential risk factors were selected based on the literature, availability in Health Facts, and clinical judgment of the physicianinvestigators. Descriptive statistics including unadjusted odds ratios were calculated; the chi-square statistic was used to determine statistical association of each potential risk factor with 30-day readmission. Because there were nearly 400 candidate variables, they were grouped into categories for initial modeling: patient and hospital characteristics, medications, laboratory results, microbiology results, indicators of organ dysfunction, characteristics of the index admission, treatment, and diagnoses. A complete list of variables is available from the authors. Missing Data Missing data were common among laboratory results. In general, we considered a missing value for a particular laboratory test as indicating that the care team felt there was no reason to order the test. Thus, missing values were assumed to lie within a test’s normal range. For example, 129,061 patients had hematocrit values and 334,290 had no hematocrit value. For the purposes of modeling, we assume that the 334,290 patients had normal hematocrits. “Missing” medications and procedures were assumed not to have been ordered or performed. Hospital exposure in the year prior to the index admission was considered missing if Health Facts had no inpatient or outpatient encounters for the patient during this time. Modeling Process We developed logistic regression models and accounted for nesting of patients within hospitals with generalized estimating equations using the GENMOD procedure in SAS software. During model development and validation we considered effect size, clinical relevance, and statistical significance. We used the c-statistic (area under the receiver operator characteristic [ROC] curve) to assess model discrimination. To assess model calibration, we divided the predicted probabilities into deciles and compared each decile’s median value with the observed proportion of 30-day readmission. www.jcomjournal.com The data were randomly divided into developmental and validation data sets, setting aside 10% of the observations for validation. The developmental data set was further divided into 20 random samples (without replacement). Using chi-square tests for categorical variables and 2-sample t tests for continuous variables, we determined the relationship of each potential predictor to 30-day hospital readmission. Variables within a category that were significant at the 0.0001 level were included in a logistic regression with backward elimination that also used a 0.0001 level. We chose this level in view of the large sample size (about 20,000 observations per sample). Each laboratory result had up to 4 variables: baseline, nadir, peak, and discharge results. As a preliminary step, these 4 variables were compared; the one with the strongest association with readmission was used in the pool of potential predictors. Modeling proceeded on all 20 subsamples. Variables retained in models for at least 10 of the 20 samples were eligible for inclusion in the final model. Within each developmental sample, the collection of category “winners” was used as potential predictors in a logistic regression model with backward elimination at the 0.005 level. The most common “winners” from the 20 developmental sets were estimated in the full developmental data set. To make sure that the modeling process did not exclude important variables, we tested whether including other variables improved model performance. We focused on categories of variables that were not represented in the final model (eg, indicators of impaired immune function and medications) and variables that were dropped late in the process. Adding these other variables back to the model resulted in minimal improvement in the c-statistic (0.01), so we did not include variables beyond the 5 originally selected. Model Validation The variable coefficients from the final model were used to calculate readmission risk for patients in the validation sample. To visualize model discrimination and calibration, we plotted an ROC curve and a calibration plot, respectively. RESULTS Characteristics of the included hospitals are shown in Table 1. There were 91 hospitals included, ranging in size from less than 5 to over 500 beds. All US census regions were represented, with the majority of hospitals Vol. 20, No. 5 May 2013 JCOM 205 RISK FOR READMISSION Table 1. Characteristics of Participating Hospitals Characteristic Hospitals, n (%) n = 91 Patients, n (%) n = 463,351 No. of beds < 100 29 (31.9) 38,948 (8.4) 100–199 16 (17.6) 63,831 (13.8) 200–299 19 (20.9) 85,556 (18.5) 300–399 17 (18.7) 123,574 (26.7) ≥ 500 10 (11.0) 151,442 (32.7) Northeast 36 (39.6) 198,177 (42.8) Midwest 16 (17.6) 78,404 (16.9) South 33 (36.3) 15,4813 (33.4) West 6 (6.6) 31,957 (6.9) Urban 89 (97.8) 462,849 (99.9) Rural 2 (2.2) Census region Location 502 (0.1) Teaching status Teaching 42 (46.2) 329,871 (71.2) Non-teaching 49 (53.8) 133,480 (28.8) in the Northeast and South regions. Almost half (46.2%) were academic health centers. Derivation of the study cohort is depicted in Figure 1. There were 463,351 index hospital stays, with 45,098 (9.7%) patients readmitted within 30 days of discharge from the index hospitalization. Mean patient age was 61 years (95% CI 61.0–61.1), with 27.3% of the population age 75 years or older. Over half (54.6%) were women. Most patients were Caucasian (78.8%) and 15.0% were African American. Patients age 65 years or older with other or unknown insurance were assumed to have Medicare. Almost half (45.1%) of patients had Medicare, 14.2% had commercial insurance, and 4.9% had Medicaid. Insurance status was unknown for 28.3% of patients. The unadjusted associations of individual risk factors with readmission are shown in Table 2. Patients with hospital exposure in the prior 12 months had higher odds of readmission than those with no or unknown hospital exposure. Readmission increased with age, with 12.2% of those age 85 years and older readmitted. Compared with commercial insurance, Medicare and Medicaid were also associated with more frequent readmission, while self-pay patients were less likely to 206 JCOM May 2013 Vol. 20, No. 5 be readmitted. Relative to patients with a Charlson index [17] of 0, patients with scores above 5 were much more likely to be readmitted. Several diagnoses and conditions were associated with readmission, including cancer, end-stage renal disease, and major organ transplantation. Compared with those with lower values, the odds of readmission were more than double for patients with blood urea nitrogen ≥ 35 mg/dL or serum creatinine levels of ≥ 2 mg/dL. Readmission increased with the number of medications ordered and dispensed during the index admission. In particular, high-dose oral corticosteroids and chemotherapy agents were strongly associated with readmission. The multivariable model contains 5 independent variables (Table 3). The adjusted odds of readmission increased with length of stay, the Charlson index, prior hospitalization, and low hemoglobin (nadir of all values). In the model, which controls for comorbidities, patients hospitalized for arthroplasty were about half as likely to be readmitted as other patients. The c-statistic in the developmental data was 0.67. The model performed almost as well in the validation data, with a c-statistic of 0.66 (Figure 2A). The calibration curve (Figure 2B) indicates reasonable performance www.jcomjournal.com ORIGINAL RESEARCH 981,581 admissions in Health Facts • Submitted diagnosis and procedure information, pharmacy, and laboratory data • Discharged 10/01/08 through 9/30/10 202,074 admissions with patients < 18 years old at the time of admission 23,339 in-hospital deaths 2587 admissions with ≥ 90% of orders originating from a rehabilitation unit 3659 admissions with ≥ 90% of orders originating from a psychiatric unit 99,884 admissions with primary or secondary diagnosis pregnancyrelated or obstetrical 666,519 qualifying admissions* 463,362 index (first) admissions • 45,098 readmitted within 30 days • 418,264 not readmitted within 30 days Figure 1. Flow chart showing inclusion and exclusion of inpatient admissions in the analytic cohort. *More than 1 exclusion reason can apply to an admission, therefore the sum of the individual exclusions exceeds the total admissions excluded. across all levels of risk. The lowest and highest estimated individual risk of readmission were 1.9% and 49%, respectively. In the validation data, 3.1% and 21.8% of the patients in the lowest and highest deciles of risk were readmitted, respectively. www.jcomjournal.com DISCUSSION Our model identified increased comorbidity and length of stay, prior hospital exposure, and low hemoglobin as risk factors for all cause readmission in a general adult inpatient population; having a hip or knee arthroplasty Vol. 20, No. 5 May 2013 JCOM 207 RISK FOR READMISSION Table 2. Unadjusted Bivariable Association of Selected Risk Factors with 30-Day Readmission Following Hospital Discharge Patients Who Were Readmitted No. of Patients Number (%) Odds Ratio (95% CI) 18–44 88,747 6548 (7.4) Reference 45–54 75,158 6402 (8.5) 1.17 (1.13–1.21) 55–64 88,409 8213 (9.3) 1.29 (1.24–1.33) 65–74 84,584 8917 (10.5) 1.48 (1.43–1.53) 75–84 80,996 9481 (11.7) 1.66 (1.61–1.72) 85–90 45,457 5537 (12.2) 1.74 (1.68–1.81) 78,325 6046 (7.7) Reference Demographic characteristics Age Insurance Commercial, other Medicare* 208,949 23,845 (11.4) 1.54 (1.50–1.59) Medicaid 22,756 2562 (11.3) 1.52 (1.44–1.59) Self-pay 22,373 1567 (7.0) 0.90 (0.85–0.95) 130,948 11,078 (8.5) 1.10 (1.07–1.14) Married/life partner 179,104 16,557 (9.2) Reference Divorced/separated 41,918 4496 (10.7) 1.18 (1.14–1.22) Single 84,535 8022 (9.5) 1.03 (1.00–1.06) Widowed 63,452 7588 (12.0) 1.33 (1.30–1.37) Unknown 94,342 8435 (8.9) 0.96 (0.94–0.99) 7467 (10.8) 1.13 (1.10–1.16) Unknown Marital status Race/ethnicity African-American Caucasian 69,381 365,039 35,243 (9.6) Reference Hispanic 10,620 932 (8.8) 0.90 (0.84–0.96) Other known 13,795 1238 (9.0) 0.92 (0.87–0.98) 4516 218 (4.8) 0.48 (0.41–0.54) Female 252,927 23,600 (9.3) Reference Male 210,365 21,496 (10.2) 1.11 (1.08–1.13) 338,271 34,887 (10.3) 1.29 (1.26–1.32) Medical 286,997 30,386 (10.6) 1.28 (1.25–1.30) Surgical 147,273 12,497 (8.5) Unknown 27,981 2215 (7.6) 249,014 25,835 (10.4) Reference 25,458 2342 (9.2) 0.88 (0.84–0.92) Unknown Sex (59 unknown) Index hospitalization Urgent or emergent admission Type of admission Reference 0.89 (0.85–0.93) Admission source Emergency department Hospital, other facility Skilled nursing facility, nursing home Other Unknown 208 JCOM May 2013 Vol. 20, No. 5 5527 797 (14.4) 1.46 (1.35–1.57) 166,396 14,709 (8.8) 0.84 (0.82–0.86) 16,956 1415 (8.4) 0.79 (0.74–0.83) www.jcomjournal.com ORIGINAL RESEARCH Table 2. Unadjusted Bivariable Association of Selected Risk Factors with 30-Day Readmission Following Hospital Discharge (continued) Patients Who Were Readmitted No. of Patients Number (%) ≤ 2 days 91,800 5677 (6.2) Reference 2.01–3 days 83,752 6077 (7.3) 1.19 (1.14–1.23) 3.01–4.25 days 99,038 8127 (8.2) 1.36 (1.31–1.40) 4.26–7 days 96,108 10,750 (11.2) 1.91 (1.85–1.98) Over 7 days 92,653 14,467 (15.6) 2.81 (2.72–2.90) Nursing home exposure prior 90 days 5054 1038 (20.5) 2.11 (1.98–2.27) Left hospital against medical advice prior 12 months 4428 707 (16.0) 1.54 (1.42–1.67) 231,399 21,885 (9.46) Reference Odds Ratio (95% CI) Hospital length of stay Prior health care utilization Hospital exposure prior 12 months No Yes 67,492 11,087 (16.4) 1.88 (1.84–1.93) 164,460 12,126 (7.37) 0.76 (0.74–0.78) 0 188,254 11,939 (6.3) Reference 1–5 251,160 28,310 (11.3) 1.88 (1.84–1.92) 23,584 4764 (20.2) 3.74 (3.60–3.88) 353 85 (24.1) 4.69 (3.67–5.99) Unknown Diagnoses and conditions Charlson index 6–10 11–20 Organ system dysfunctions 0 389,745 1 58,236 7498 (12.9) 1.50 (1.46–1.54) 2–5 15,370 2541 (16.5) 2.00 (1.92–2.09) 9531 1608 (16.9) 1.91 (1.81–2.02) 38,321 6627 (17.3) 2.10 (2.04–2.16) Blood dyscrasia Cancer Coronary artery disease 35,059 (9.0) Reference 73,989 8704 (11.8) 1.29 (1.26–1.33) 113,997 13,383 (11.7) 1.33 (1.30–1.36) 10,553 2159 (20.5) 2.45 (2.34–2.58) 100,259 12,556 (12.5) 1.45 (1.42–1.49) 55,420 8298 (15.0) 1.78 (1.73–2.06) 3855 650 (16.7) 1.89 (1.74–1.87) Pneumonia 33,421 4145 (12.4) 1.34 (1.30–1.39) Sepsis 17,652 2639 (15.0) 1.67 (1.60–1.74) 145,623 18,438 (12.7) 1.58 (1.55–1.61) Blood urea nitrogen ≥ 35 mg/dL 64,069 10,670 (16.7) 2.12 (2.07–2.17) Estimated glomerular filtration rate 70,782 11,231 (15.9) 2.00 (1.95–2.04) Diabetes End stage renal disease Fluid or electrolyte imbalance Heart failure Major organ transplantation Laboratory studies Absolute lymphocyte count < 800/µL < 40 mL/min/1.73m2 Hemoglobin (nadir)† < 8 g/dL 34,776 5667 (16.3) 2.34 (2.27–2.42) 8–11 g/dL 161,479 18,924 (11.7) 1.60 (1.56–1.63) > 11 g/dL 267,096 20,507 (7.7) Reference www.jcomjournal.com Vol. 20, No. 5 May 2013 JCOM 209 RISK FOR READMISSION Table 2. Unadjusted Bivariable Association of Selected Risk Factors with 30-Day Readmission Following Hospital Discharge (continued) Patients Who Were Readmitted No. of Patients Number (%) Odds Ratio (95% CI) Platelet count < 100,000/µL 27,786 4560 (16.4) 1.91 (1.85–1.98) Serum creatinine ≥ 2 mg/dL 46,920 7961 (17.0) 2.09 (2.03–2.14) 101,657 15,129 (14.9) 1.93 (1.90–1.98) Serum potassium > 5.5 mmol/L 19,661 3302 (16.8) 1.94 (1.87–2.02) Total bilirubin ≥ 2 mg/dL 19,541 2944 (15.1) 1.69 (1.62–1.76) White blood cells < 4,000/µL 27,595 4143(15.0) 1.70 (1.65–1.76) Serum albumin < 3 g/dL Treatments and procedures No. of medications dispensed 0 190,255 17,259 (9.1) 1–10 98,186 8243 (8.4) 0.92 (0.89–0.94) Reference 11–20 112,771 11,192 (9.9) 1.10 (1.08–1.13) 21–30 44,761 5585 (12.5) 1.43 (1.38–1.48) 31 or more 17,378 2819 (16.2) 1.94 (1.86–2.03) Amiodarone 9407 1478 (15.7) 1.75 (1.66–1.86) Arthroplasty 26,083 1160 (4.4) 0.42 (0.39–0.44) Beers criteria, any agent (age > 74) 22,480 2813 (12.5) 1.08 (1.03–1.12) Blood transfusion 8190 1304 (15.9) 1.78 (1.67–1.89) Chemotherapy agent 2535 700 (27.6) 3.58 (3.28–3.91) Hemodialysis 10,760 2148 (20.0) 2.38 (2.27–2.50) High-dose oral corticosteroid 14,228 2295 (16.1) 1.83 (1.74–1.91) Note: To protect confidentiality, the age of patients over 90 years old was reset to 90. *Includes patients age 65 or older with other or unknown insurance. †Patients with unknown hemoglobin (3.5%) were assumed to have values over 11 g/dL. was associated with lower risk of readmission. Model performance was modest (c-statistic = 0.67). Our model performed as well or better than most models based on claims data. In fact, it performed as well or better than most models that studied a single condition. A recent systematic review of readmission risk models [9] found 26 distinct models. Nine models from large, multicenter US studies reported c-statistics of 0.55–0.65. Of the 6 models with a reported c-statistic of 0.7 or above, 4 were based on European or Australian data and 1 US study was based on heart failure patients at a single center. Coleman’s [18] model using Medicare Current Beneficiary Survey data had good discrimination (c = 0.77) when prior utilization and diagnoses were included; adding self-reported survey items on functional status and vision improved model performance (c = 0.83). 210 JCOM May 2013 Vol. 20, No. 5 Stronger models can undoubtedly be created by including additional clinical and social factors or by restricting the population to more narrowly defined constellations of conditions. We were able to identify 25% of our sample with less than a 6% risk of readmission. In the validation data, 21.8% and 15.1% of the patients in the highest two risk deciles were readmitted. Although far from perfect, such data can help target interventions to prevent readmission to higher risk individuals. Studies of readmission vary widely in terms of case finding and the time period studied. Vest et al [19] conducted a systematic review of preventable readmissions; indicators of complexity or general ill health (eg, Charlson index), increasing length of stay, and Medicare or Medicaid status were the most commonly identified risk factors. In a large, prospective cohort study of all-cause www.jcomjournal.com ORIGINAL RESEARCH Table 3. Multivariable (Adjusted) Association of Independent Risk Factors with All-Cause 30-Day Readmission Following an Acute Hospitalization Risk Factor Charlson index Coefficient Odds Ratio (95% CI) 0.1335 1.14 (1.14–1.15) Length of stay ≤ 2 days Reference 2–3 days 0.1151 1.12 (1.08–1.17) 3–4.25 days 0.2631 1.30 (1.25–1.35) 4.25–7 days 0.4790 1.62 (1.56 –1.67) > 7 days 0.7305 2.08 (2.00–2.15) –0.8014 0.45 (0.42–0.48) 0.1970 1.22 (1.18–1.26) Arthroplasty procedure Hemoglobin (nadir) < 8 g/dL 8–11 g/dL Reference > 11 g/dL –0.2247 0.80 (0.78–0.82) Hospital exposure prior 12 months No Reference Yes 0.3919 1.48 (1.44–1.52) Unknown –0.2252 0.80 (0.78–0.82) C-statistic 0.668 readmission in 11 Ontario hospitals, van Walraven [20] found that length of stay, acuity (emergent admission), comorbidity [17], and emergency department use in the prior 6 months were associated with death or readmission. Prior hospital exposure is a consistent risk factor for readmission [5,7,18,21,22]. Other common risk factors include poor physical functioning [5,21–23] and social factors such as social instability and living alone [7,21– 26]. While a large number of risk factors in our analysis had high odds ratios when considered in bivariable analyses, many occurred infrequently, making them less useful for patient-level prediction in a multivariable model. For example, the odds ratio for readmission was 3.58 among patients who received chemotherapy agents, but only 2535 patients (0.55%) received them. This suggests that analyzing a more homogeneous group of patients (eg, patients with cancer or heart failure) might help identify a more predictive set of risk factors. Readmission rates in large patient samples are often 15% or higher, depending on the population and the definition of readmission [4,5,7,23,27,28]. Patients in our sample had a lower readmission rate than these studies, although van Walraven [20] found a similar rate among general patients in 11 Ontario hospitals (8.0% combined outcome of death www.jcomjournal.com or readmission within 30 days). There are likely several reasons for our relatively low rate. First, in Medicare data, about a fifth of readmissions are to a different hospital [16,29]. In our data, we could only track readmissions to the same hospital system. Second, we restricted index admissions to the first hospitalization during a period. Because the first admission is less likely to have been preceded by a prior admission than subsequent stays, and prior hospital utilization was associated with readmission, this likely reduced our rate. Consistent with this suggestion, individuals with prior hospital exposure had a much higher risk of readmission than the overall sample. We excluded elective admissions from the readmission count; many studies with high readmission rates included elective readmissions [4,5,21,29]. Facilities that contributed data to Health Facts might be early adopters of electronic medical records, which could have affected care delivery. Finally, our data included adults in Medicare managed care plans who are typically excluded from analyses of Medicare claims because hospital claims for those individuals are not submitted. Because patients in managed care are often healthier, their readmission rate could be lower. Although our c-statistic is modest, our model points the way towards several paths to clinically useful point- Vol. 20, No. 5 May 2013 JCOM 211 RISK FOR READMISSION 25 1.0 A 0.8 Sensitivity Actual readmission, % 20 B 15 0.6 10 0.4 5 0.2 0 0 0 5 10 15 20 25 Predicted readmission,% 0 0.2 0.4 0.6 0.8 1.0 1 - Specificity Figure 2. Calibration (Panel A) and receiver operator characteristic (Panel B) plots for logistic model of all-cause 30-day readmissions in the validation data set. of-service rules. For example, other important variables such as functional data, support systems, and health literacy could be collected by hospital personnel during discharge planning to estimate readmission risk. Electronic systems could alert clinicians when patients had developed increased risk due to changes in laboratory results or medication orders. A recent meta-analysis found that individualized discharge plans reduce readmissions over routine discharge care [30]. One example is the Re-Engineered Discharge (RED) program [31], an 11-component intervention that included patient education, organizing postdischarge appointments and services, confirming medications, a written discharge plan, and a postdischarge phone call. In a trial of 749 patients, RED reduced subsequent hospital utilization by 30%. An intervention that provided patients with communication tools, encouraged them to take a more active role in their care, and provided visits and calls from a “transition coach” reduced 30- and 90-day readmissions [32]. With better risk models, graded interventions would be possible, reserving proven but resource-intensive strategies for the highest risk individuals. Thus, our model may serve as a basis for developing more refined models that include social and functional information, allowing hospitals to focus resources on patients at highest risk. 212 JCOM May 2013 Vol. 20, No. 5 Strengths and Limitations We analyzed a large, cross-sectional sample of hospitalized adults from 91 hospitals. In addition to administrative variables, we included clinical information on laboratory results, medications and treatments, and severity of illness. Using data that can be accessed in real time can support predicting readmission at the time of a patient’s discharge. Because we had data on patients regardless of insurance status, our sample included patients in Medicare managed care who are typically absent from Medicare claims data. Ideally, we would want to include information on functional limitations, social support, substance abuse, socioeconomic status, and social instability such as number of address changes [7,22–24,26]. We were unable to track readmissions to hospitals in different health systems or hospitals not included in Health Facts, which undoubtedly reduced the readmission rate in our data. Patients admitted to a different hospital have some differences from those admitted to the same hospital [16]. Nonetheless, because only about 20% of patients are admitted to a different hospital, that is unlikely to have a major effect on our findings. Participating institutions may not be representative of US hospitals in general. In particular, rural hospitals are underrepresented in our study. We were unable to identify discharge medications, which could be an important factor in readmissions. www.jcomjournal.com ORIGINAL RESEARCH CONCLUSION Comorbidity and prior utilization are strong risk factors for readmission in a general population of patients discharged from the hospital. Despite the availability of a large number of potentially relevant clinical variables, model performance was modest. Considering that the proportion of readmissions that are potentially preventable is likely under 25% [28,33], it will be difficult for hospitals to successfully identify and intervene with patients with a high likelihood of readmission. Including information on social support and functional status will likely improve model performance. Specific laboratory abnormalities might be more strongly associated with readmission in relevant subpopulations of patients (eg, infection indicators in pneumonia patients). Using clinical data to predict readmission in more homogeneous groups of patients is worthy of further study. Acknowledgements: The authors would like to acknowledge Jane Griffin, RPh, and Jeffrey Binkley, PharmD, for their facilitation of this project. Preliminary results from this study were presented at the Cerner Health Conference on 10 October 2011. Corresponding author: Robin L. Kruse, PhD, MA306 Medical Sciences Building, University of Missouri School of Medicine, Columbia, MO 65212, [email protected]. Funding/support: This study was partially supported by the Tiger Institute Research Group, a collaborative research effort between the University of Missouri and the Cerner Corporation. The Tiger Institute, wholly owned by the University of Missouri, had no role in conduct of the study; management, analysis, or interpretation of the data; or the preparation, review, or approval of the manuscript. Financial disclosures: Mr. Hays and Dr. Emons are employed by the Cerner Corporation. Author contributions: conception and design, RLK, HDH, MFE, DSW, DRM; analysis and interpretation of data, RLK, HDH, RWM, MFE, DRM; drafting of article, RLK, MFE; critical revision of the article, RLK, RWM, MFE, DSW, DRM; statistical expertise, RWM; administrative or technical support, DRM; collection and assembly of data, RLK, HDH, MFE. REFERENCES 1. Report to the Congress: promoting greater efficiency in Medicare. Washington, DC: Medicare Payment Advisory Commission; 2007 Available at http://www.medpac.gov/ documents/jun07_entirereport.pdf. www.jcomjournal.com 2. Pub. L. No. 111-148 § 124 Stat. 119 (2010). 3. McClellan M, McKethan AN, Lewis JL, et al. A national strategy to put accountable care into practice. Health Aff (Millwood) 2010;29:982–90. 4. Joynt KE, Jha AK. Who has higher readmission rates for heart failure, and why? Implications for efforts to improve care using financial incentives. Circ Cardiovasc Qual Outcomes 2011;4:53–9. 5. Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med 2009;360:1418–28. 6. Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA 2011;305:675–81. 7. Amarasingham R, Moore BJ, Tabak YP, et al. An automated model to identify heart failure patients at risk for 30-day readmission or death using electronic medical record data. Med Care 2010;48:981–8. 8. Stimson CJ, Chang SS, Barocas DA, et al. Early and late perioperative outcomes following radical cystectomy: 90day readmissions, morbidity and mortality in a contemporary series. J Urol 2010;184:1296–300. 9. Kansagara D, Englander H, Salanitro A, et al. Risk prediction models for hospital readmission: a systematic review. JAMA 2011;306:1688–98. 10. Ross JS, Mulvey GK, Stauffer B, et al. Statistical models and patient predictors of readmission for heart failure: a systematic review. Arch Intern Med 2008;168:1371–86. 11. Goyal A, Spertus JA, Gosch K, et al. Serum potassium levels and mortality in acute myocardial infarction. JAMA 2012;307:157–64. 12. Amin AP, Salisbury AC, McCullough PA, et al. Trends in the incidence of acute kidney injury in patients hospitalized with acute myocardial infarction. Arch Intern Med 2012;172:246–53. 13. Salisbury AC, Reid KJ, Alexander KP, et al. Diagnostic blood loss from phlebotomy and hospital-acquired anemia during acute myocardial infarction. Arch Intern Med 2011;171:1646–53. 14. Kosiborod M, Inzucchi SE, Goyal A, et al. Relationship between spontaneous and iatrogenic hypoglycemia and mortality in patients hospitalized with acute myocardial infarction. JAMA 2009;301:1556–64. 15. Berger A, Pelton SI, Klein JO, et al. Clinically based surveillance of invasive meningococcal disease in young children admitted to selected US hospitals between January 2000 and June 2009: A retrospective cohort study. Hum Vaccin Immunother 2012;8:384–9. 16. Kind AJ, Bartels C, Mell MW, et al. For-profit hospital status and rehospitalizations at different hospitals: an analysis of Medicare data. Ann Intern Med 2010;153:718–27. 17. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373–83. 18. Coleman EA, Min SJ, Chomiak A, Kramer AM. Posthospital care transitions: patterns, complications, and risk identi- Vol. 20, No. 5 May 2013 JCOM 213 RISK FOR READMISSION fication. Health Serv Res 2004;39:1449–65. 19. Vest JR, Gamm LD, Oxford BA, et al. Determinants of preventable readmissions in the United States: a systematic review. Implement Sci 2010;5:88. 20. van Walraven C, Dhalla IA, Bell C, et al. Derivation and validation of an index to predict early death or unplanned readmission after discharge from hospital to the community. CMAJ 2010;182:551–7. 21. Hasan O, Meltzer DO, Shaykevich SA, et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med 2010;25:211–9. 22. Evans RL, Hendricks RD, Lawrence KV, Bishop DS. Identifying factors associated with health care use: a hospitalbased risk screening index. Soc Sci Med 1988;27:947–54. 23. Arbaje AI, Wolff JL, Yu Q, et al. Postdischarge environmental and socioeconomic factors and the likelihood of early hospital readmission among community-dwelling Medicare beneficiaries. Gerontologist 2008;48:495–504. 24. Strunin L, Stone M, Jack B. Understanding rehospi talization risk: can hospital discharge be modified to reduce recurrent hospitalization? J Hosp Med 2007;2: 297–304. 25. Rodriguez-Artalejo F, Guallar-Castillon P, Herrera MC, et al. Social network as a predictor of hospital readmission and mortality among older patients with heart failure. J Card Fail 2006;12:621–7. 26. Murphy BM, Elliott PC, Le Grande MR, et al. Living alone predicts 30-day hospital readmission after coronary artery bypass graft surgery. Eur J Cardiovasc Prev Rehabil 2008;15:210–5. 27. Allaudeen N, Vidyarthi A, Maselli J, Auerbach A. Redefining readmission risk factors for general medicine patients. J Hosp Med 2011;6:54–60. 28. van Walraven C, Jennings A, Taljaard M, et al. Incidence of potentially avoidable urgent readmissions and their relation to all-cause urgent readmissions. CMAJ 2011;183:E1067– E1072. 29. Nasir K, Lin Z, Bueno H, et al. Is same-hospital readmission rate a good surrogate for all-hospital readmission rate? Med Care 2010;48:477–81. 30. Shepperd S, McClaran J, Phillips CO, et al. Discharge planning from hospital to home. Cochrane Database Syst Rev 2010;(1):CD000313. 31. Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med 2009;150:178–87. 32. Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med 2006;166:1822–8. 33. van Walraven C, Bennett C, Jennings A, et al. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ 2011;183:E391–E402. Copyright 2013 by Turner White Communications Inc., Wayne, PA. All rights reserved. 214 JCOM May 2013 Vol. 20, No. 5 www.jcomjournal.com