Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
1041
Correlates of Left Ventricular Mass in a
Population Sample Aged 36 to 37 Years
Focus
on
Lifestyle and Salt Intake
Markku Kupari, MD; Pekka Koskinen, MD; Juha Virolainen, MD
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
Background Echocardiographically determined left ventricular (LV) mass predicts adverse cardiovascular events in
the general population. We have assessed the correlates of LV
mass in a population-based study focusing on lifestyle and salt
intake.
Methods and Results A random sample of 120 persons born
in 1954 was invited; 93 (42 men) entered the study. The subjects'
physical activity and alcohol, tobacco, and coffee consumption
were quantified by 2-month diary follow-up, and sodium intake
was quantified by 7-day food records. Blood pressure was averaged for casual cuff measurements made 2 months apart. LV
mass was determined by M-mode echocardiography, and stroke
volume was determined by Doppler. Hematocrit and serum
insulin were measured. In multiple linear regression analysis, LV
mass was related positively and independently (P<.05) to body
weight, systolic blood pressure, stroke volume, sodium intake,
hematocrit, and energy expenditure in leisure-time physical
activity. Additional analyses showed that the relation of LV mass
chocardiographically measured left ventricular
(LV) mass is an important predictor of adverse
cardiovascular events in the general population.12 Knowledge of its determinants could help design
individual and population strategies to prevent or reverse LV hypertrophy. The Framingham Heart Study
has shown that age, sex, body size, blood pressure,
obesity, and valvular or coronary heart disease have the
most influence on the variation of LV mass across the
population.3-7 Although leisure-time physical activity,4
alcohol consumption,5 smoking,5 and diabetes6 also had
some effect, their role was less consistent and depended
on sex or on both sex and age. Other echocardiographic
studies have suggested that sodium intake,8-10 LV stroke
volume and contractility,1""2 serum insulin,13 and blood
viscosity14 may also contribute to the variation of LV
mass. However, these studies involved clearly more
selected groups of hypertensive and normotensive persons, and their results are of less universal applicability.
Potentially important as it is, the association of LV mass
with dietary salt has never been evaluated in any
general population. We have studied a fully random
sample of people born in 1954 to assess further the
factors associating with the echocardiographic LV mass
in univariate and multivariate analyses. Additional distinctive features of our study are that we focused on the
E
Received July 13, 1993; revision accepted December 4, 1993.
From the Division of Cardiology (First Department of Medicine), Helsinki University Central Hospital, Helsinki, Finland.
Correspondence to Dr Markku Kupari, Division of Cardiology,
Helsinki University Central Hospital, FIN-00290 Helsinki, Finland.
to daily sodium intake depended on blood pressure (P<.001 for
the interaction); the multiple regression coefficient (±SE) was
0.41 ±0.11 g. mEq' d-1 (P=.001) in subjects with systolic blood
pressure above the population median but statistically nonsignificant (-0.15±0.10 g mEq1' d'1) in those with lower blood
pressure. LV mass was clearly elevated only in persons with both
blood pressure and sodium intake above the population medians.
Conclusions Body weight, blood pressure, stroke volume,
sodium intake, physical activity, and hematocrit are independent predictors of LV mass among unselected persons aged 36
to 37 years. The synergistic interaction of dietary salt with
blood pressure suggests that high sodium intake may sensitize
the heart to the hypertrophic stimulus of pressure load.
Prospective studies are needed to confirm these cross-sectional
associations. (Circulation. 1994;89:1041-1050.)
Key Words * left ventricle * lifestyle * blood pressure
sodium
1.
role of such factors as salt intake, physical activity,
smoking, and alcohol consumption and looked systematically for interactions between the different explanatory variables.
Methods
Subjects
All persons living in Helsinki and born in 1954 (3730 men
and 4250 women) were eligible for our study. Of them, the
Central Population Registry took a random sample of 120
individuals (55 men and 65 women) whom we invited by a
letter explaining the aims and course of our work. If necessary,
a second letter was mailed 2 to 3 weeks later. A total of 112
persons could be contacted, and 95 were willing to participate.
Of those declining, 7 did not specify any reason, 5 were busy at
work, 3 had medical examinations under way elsewhere, and 2
were pregnant. Each potential participant had a personal
appointment with a research nurse who explained the study
procedures in detail and recorded the subject's medical history, use of drugs, and presence of hypertension in next-of-kin.
Details of the subject's daily work also were recorded, and the
occupational physical activity graded as minimal, light, moderate, or heavy. Ninety-three persons (51 women and 42 men,
78% of the original sample) decided to enter the study. Two of
them had chronic schizophrenia, and 1 had myasthenia. Seven
persons had mild allergic diseases or asthma, but none used
sympathomimetics or steroids regularly. Several subjects had
been in surveillance for high blood pressure, but none received
drugs for it. No subject had a known heart disease. One man
reported effort-related chest pain, but his exercise ECG (performed by us) showed no myocardial ischemia.
Circulation Vol 89, No 3 March 1994
1042
Study Design
The study started with a prospective collection of lifestyle
data. Each participant was given a pocket diary for recording
of daily physical activity and consumption of alcohol, tobacco,
and coffee. Another diary was given for a complete 7-day food
record. The subjects were asked not to change their lifestyle
because of participation. After 2 months, they returned the
diaries and underwent blood tests; measurement of height and
weight; physical examination; 12-lead ECG; complete twodimensional, M-mode, and Doppler echocardiographic studies; and tests for blood pressure variability. The data were
subjected to statistical analyses targeted to identify the independent correlates of echocardiographic LV mass in the study
population. The protocol was accepted by the local ethics
committee.
Lifestyle Diary and Data Analysis
Physical Activity
Each day, the subjects recorded the type of physical activity
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
they had practiced (eg, walking, jogging, swimming, gardening,
and so on) and its exact duration. Only leisure-time activities
were noted. The energy expended was calculated as suggested
by Wilson et al'5 by multiplying the metabolic equivalent value
(MET; 1 MET=the energy expended by a person at rest, ie,
z1 kcal kg` * h-') of each activity by the time (hours) spent
in it. The MET values of different activities were adopted from
published tables.'5 The average energy expenditure per day of
follow-up was used as a physical activity index. Supporting its
usefulness, the physical activity index (MET. h/d) correlated
inversely with body mass index (r= -.27, P=.010) and resting
heart rate (r= -.23, P=.039) and directly with the average
daily energy intake calculated from the food records (see
below) (r=.24, P=.028).
.
Alcohol, Tobacco, and Coffee Consumption
The subjects entered into the diary the types and exact
amounts of alcoholic beverages, the number of cigarettes, and
the number of standard-size cups of coffee they consumed
each day. The alcoholic drinks were converted to grams of
absolute ethanol. The average use of ethanol, tobacco, and
coffee was determined by dividing the respective total consumption by the number of follow-up days. Supporting the
representativeness of the data, the calculated average daily
ethanol consumption correlated directly with serum y-glutamyltransferase measured at the end of the diary follow-up
period (r=.40, P=.001).
Diet Records and Data Analysis
The data on diet were collected by means of a 7-day food
record. The days were selected by the investigators and distributed evenly over the 2-month follow-up period. Each day of the
week was covered once, but holidays were skipped. In addition to
blank forms for recording, the subjects had model forms and
written and illustrated instructions prepared by a nutritionist to
ensure accurate completion of the records. The subjects returned
the records to the nutritionist, who checked the food consumption entries for adequacy and asked supplemental questions if
necessary. The records were analyzed for energy, nutrient, and
mineral intake using commercial software (UNILEVER DIETARY
ANALYSIS PROGRAM, Unilever Inc) and a database on the nutrient and mineral composition of Finnish foods.'6 The average
daily intake of sodium (mEq) was calculated for the analyses of
the present work.
Laboratory Tests
Venous blood was sampled after the subjects fasted overnight. Peripheral blood count, hematocrit, blood glucose,
serum electrolytes, serum creatinine, and liver enzymes were
determined immediately, and the remaining serum was stored
at -20°C. The serum insulin concentration was measured later
using a commercial radioimmunoassay kit (Pharmacia).
Blood Pressure Measurements
The brachial artery blood pressure (Korotkoff phases I and
V) was measured after a 15- to 30-minute rest using a
sphygmomanometer with the subject in a sitting position. The
measurement was made on the subject's first visit to our unit
and repeated twice at the echocardiographic study about 2
months later. The means of all three measurements of systolic
and diastolic blood pressure were used in the analyses.
Continuous noninvasive finger arterial pressure recordings
were made using an Ohmeda 2300 Finapres device'7 and
commercial software (CAFTS, Medikro Inc). The aim was to
quantify the variability and reactivity of blood pressure in
addition to its level at rest. Continuous finger arterial pressure
signal was loaded into a computer first during 5 to 10 minutes
of controlled respirations (15 min-') at supine rest and then
during a standardized Valsalva maneuver (+40 mm Hg for 15
seconds). For our purposes, the following indexes of systolic
finger blood pressure were computed: 5-minute average at
rest, peak value in the overshoot phase of the Valsalva test,
and the total spectral power over frequencies from 0 to 0.5 Hz
(representing the beat-to-beat blood pressure variance). The
details and validation of our recording technique and power
spectral analyses are available elsewhere.'8'19
Echocardiography
All echocardiographic studies were made with a commercially available ultrasonograph (Aloka SSD 830) equipped
with a 2.5-MHz phased-array transducer and a strip-chart
recorder. The subjects were in a postabsorptive state and
rested supine for 10 to 15 minutes before the recordings.
Throughout the ultrasound study, they were lying in an
individual left lateral position.
Determination of LVMass
Two-dimensional imaging and color Doppler examinations
were made first to look for valve diseases and segmental
abnormalities of LV function. A standard M-mode LV study
was recorded thereafter as detailed elsewhere.20 The recordings were taken at a speed of 50 mm/s together with an ECG
and a phonocardiogram. The tracings were analyzed later on
an x-y digitizer to determine the LV cavity dimension and wall
thicknesses at end diastole.20 All measurements were made by
the leading edge-to-leading edge technique and averaged
over five cycles. The analyzer had no knowledge of the
subject's other data. The LV mass was calculated using the
cube formula2' and the correction equation of Devereux et
al.22 The LV mass data were also normalized to body area and
body height, but all correlative and regression analyses were
made using the uncorrected LV mass.
Determination of Stroke Volume and Peripheral
Arterial Resistance
LV stroke volume was determined as the product of the
cross-sectional area and the velocity-time integral in the LV
outflow tract.23 The diameter of the outflow tract was determined in parasternal two-dimensional views as the average of
three measurements; the area was calculated by circular
geometry. Pulsed wave Doppler was used to record the systolic
velocities at three adjacent sites in the outflow tract as detailed
elsewhere.24 The modal velocities were traced on the x-y
digitizer, and the velocity-time integral was averaged over all
measured cycles (five cycles per measurement site). Peripheral
arterial resistance was calculated as 103 *MBP/HR SV, where
MBP is the computed 5-minute average of finger arterial mean
pressure at echocardiography (mm Hg), HR is heart rate
(beats per minute), and SV is stroke volume (mL).
Kupari et al Correlates of Left Ventricular Mass
Reproducibility
The reproducibility of our M-mode echocardiographic technique has been validated earlier.20 To confirm the reproducibility
of the key measurements in this work, the ultrasound study was
repeated 3 weeks later in six subjects. The standard deviations of
the differences between the paired data were 23.5 g for the LV
mass and 7.5 mL for stroke volume. The absolute difference as
percentage of the mean of the two measurements was 10.8±5.3%
for the LV mass and 12.7±8.7% for the stroke volume.
Statistical Analysis
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
Group mean values were compared by Student's t test,
ANOVA, or Mann-Whitney U test. Associations between the
studied variables were tested by calculating bivariate Pearson's
product-moment or Spearman's rank correlation coefficients.
To find out the independent correlates of LV mass, multiple
linear regression analyses were made. Before the analyses, all
continuous variables were tested for normal distribution by
Kolmogorov-Smirnov one-sample test. If the distribution was
nonnormal, the data were transformed to their natural logarithms or square roots, whichever method moved the distribution closer to normality. A basic multiple regression model was
first constructed for the prediction of LV mass in the total
study population and in men and women separately; the
variables included in these analyses are listed in "Results."
Additional analyses were performed thereafter in the total
population by substituting related variables of body size or
blood pressure in the basic equation. Interactions between any
two explanatory variables were assessed by correlating their
product term with the residuals of the model. Because an
interaction of systolic blood pressure and sodium intake was
found, the LV mass data were analyzed also after stratification
by the median values of blood pressure and sodium intake.
When necessary, the LV mass data were adjusted for factors
other than sodium intake and blood pressure using the multiple regression coefficients of the basic model. The group data
are given as mean+SD or as median (range), and the associations are reported as bivariate correlation coefficients, partial
correlation coefficients, and multivariate regression coefficients (b) ±SE. Squared multiple correlation coefficients (R2)
were also calculated. Values of P<.05 were considered statistically significant. All analyses were performed on a microcomputer using commercially available statistical software (SYSTAT
Version 5.2, Systat Inc).
Results
Of the 93 participants, all except two women completed the study. The mean diary follow-up time was 64
days (range, 13 to 74 days). High-quality echocardiographic recordings were obtained in 89 subjects (42
men), and the diet records were sufficiently exact for
calculation of salt intake in 85 subjects (40 men).
Study Population Characteristics
Clinical, Hemodynamic, and Echocardiographic Data
All subjects were aged 36 to 37 years. Their anthropometric characteristics are shown in Table 1. The body
mass index was <20 kg/M2 in 11 subjects, 20 to 25 kg/m2
in 49, 25 to 30 kg/M2 in 25, and >30 kg/m2 in 6 subjects.
Twenty-two participants (12 men) had a family history
of hypertension. Clinical examination did not suggest
heart disease in any subject. None had signs of significant mitral or aortic valve disease at echocardiography,
but incipient dilated cardiomyopathy was considered
possible in one man.
The hemodynamic and echocardiographic data are
shown in
Table 2.
All
and
women,
including ratios of mass to height and
men
LV
measurements
were
different
in
1043
TABLE 1. Anthropometric Characteristics of
Study Population
All Subjects Mean
Women
P*
Measurement
(n=91)
(n=42)
(n=49)
Height, cm
171+10
178±7
165±6
<.001
Weight, kg
70±14
78±11
64±13 <.001
Body area, m2t
1.81±0.20 1.96±0.15 1.69±0.16 <.001
Body mass index,
23.9±3.9 24.4±2.8 23.5±4.5 .240
kg/m2t
Values are mean±SD.
*P values for the sex difference.
tBody area=0.007184. (weight in kg)0425 (height in cm)0725.
tBody mass index= (weight in kg)/(height in m)2.
mass to body area. After adjustment for height and weight
in a linear regression model, sex (male, 0; female, 1) had
significant influence on stroke volume (b= -6.1±2.9 mL,
P=.042), septal thickness (b=-1.4±0.4 mm, P=.001),
and free wall thickness (b=1.1±0.5 mm, P=.025) but not
on end-diastolic diameter or peripheral arterial resistance.
Lifestyle Characteristics and Laboratory Data
Fifty subjects (22 men) were nonsmokers, 24 (10
men) consumed 1 to 10 cigarettes per day, and 17 (10
men) smoked more than 10 cigarettes per day (P=.21
for the sex difference). Occupational physical workload
was graded minimal in 42 persons, light in 21, moderate
in 22, and heavy in 3; 3 persons were not in active work.
The other lifestyle data and the key laboratory measurements are summarized in Table 3. Men drank more
alcohol and had higher physical activity and higher
hematocrit than women. Their salt intake was also
higher, but the difference was not statistically significant
when the intake was calculated per body weight. All
subjects had normal peripheral blood counts, serum
electrolytes, creatinine, and fasting blood glucose (data
not shown).
Correlates of LV Mass in Univariate Analyses and
After Adjustment for Sex and Body Size
Participants with a family history of hypertension had
an LV mass of 186±60 g compared with 162±42 g in the
remaining population (P=.050 for sex-adjusted difference). Table 4 shows the correlation of LV mass with
the anthropometric and lifestyle characteristics, and
Table 5 shows the correlation with the hemodynamic
and laboratory measurements. The partial correlations
given in Tables 4 and 5 represent the residual association of LV mass with the studied variables after adjustment for sex, weight, and height, alone or in combinations. Table 4 shows that LV mass was related more
closely to weight than to height or body mass index.
Sodium intake, stroke volume, hematocrit, brachial
artery systolic pressure, and peak systolic finger arterial
pressure at the Valsalva test correlated statistically
significantly with the LV mass even when the variation
related to sex and body size was taken out (Tables 4 and
5). The association of LV mass with physical activity was
significant only after adjustment for weight (Table 4).
By contrast, LV mass was related to serum insulin in
univariate analysis but not after adjustment for weight
(Table 5).
1044
Circulation Vol 89, No 3 March 1994
TABLE 2. Hemodynamic and Echocardiographic Measurements in Study Population
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
All Subjects
Men
Variable
(n=91)
(n=42)
Heart rate, bpm
67+10
65+1 1
Brachial artery blood pressure, mm Hg
Systolic
125±14
129±14
Diastolic
81±9
80+9
Finger arterial systolic pressure, mm Hg
5-Min average
137±18
141±16
Square-root total power
4.4±1.2
4.4±1.2
Peak value at Valsalva test
179+32
184±35
Stroke volume, mL
56±11
63±12
Peripheral arterial resistance, mm Hg* L-' min-1
26±6
24±5
Left ventricular
End-diastolic diameter, mm
49.5±4.1
51.2±4.6
9.1±1.7
Septal thickness, mm
10.0±1.8
Posterior wall thickness, mm
9.6±1.8
10.5±1.8
Mass, g
168±48
197±45
Mass/height, g/mt
97±25
110±25
Mass/body area, g/m2§
92±20
101±21
bpm indicates beats per minute. Values are mean±SD.
*P values for the sex difference.
tn=47 for the echocardiographic left ventricular measurements.
tLeft ventricular mass/height3 exceeded 102 g/m in 7 women and 143 g/m in 4 men.
§Left ventricular mass/body area22 exceeded 1 10 g/m2 in 3 women and 134 g/m2 in 3 men.
Multiple Regression Analyses
Basic Model
To find out the independent correlates of LV mass,
multiple linear regression analyses were performed with
the following variables: sex (male, 0; female, 1), height,
weight, body mass index category (<20 kg/m2, -1; 20 to
25 kg/M2, 0; 25 to 30 kg/M2, 1; >30 kg/M2, 2), family
history of hypertension (negative, 0; positive, 1), squareroot physical activity index, occupational physical workload (minimal, 0; light, 1; moderate, 2; heavy, 3), smoking
(nonsmoker, 0; 1 to 10 cigarettes per day, 1; > 10 cigarettes
per day, 2), square-root daily ethanol consumption, daily
coffee consumption, daily sodium intake, systolic brachial
Women
(n=49)t
68±8
P
121±14
79±10
.011
.309
134±18
4.4±1.3
174±29
51±7
28±6
.080
.830
.135
<.001
.001
48.1±3.0
8.4+1.3
8.9±1.4
142±33
86±19
84±16
<.001
<.001
<.001
<.001
.093
<..001
<.001
artery pressure, stroke volume, peripheral arterial resistance, hematocrit, and log serum insulin. The analyses
were made both in all subjects and separately in men and
women. The statistically significant correlates of LV mass
are shown in Table 6. It is noteworthy that sex was not an
independent predictor of LV mass. The factors included
in the model (Table 6, all subjects) were also tested for sex
interactions, but none were found, suggesting that the
regression slopes were not statistically significantly different between men and women.
Substitutes for Weight and Systolic Blood Pressure
To study further the association of LV mass with
obesity, height and body mass index were substituted
TABLE 3. Lifestyle Characteristics and Laboratory Data in Study Population
All Subjects
Men
Characteristic
(n=91)
(n=42)
Physical activity index, MET. h/d
2.2 (0-14)
Ethanol consumption, g/d
14.6 (0-84)
Ethanol consumption/weight, g. kg-' d-1
0.21 (0-1.2)
Coffee consumption, cups per day
3.5 (0-11.9)
Sodium intake, mEq/dt
158+50
Sodium intake/weight, mEq kg-' d-1
2.3+0.6
Blood hematocrit, %
42±4
Serum insulin, mU/L
4.7 (1.5-30.4)
MET indicates metabolic equivalent (:1 kcal kg-1 . h-1).
Values are median (range) of nonnormally distributed data and mean±SD
*P value for the sex difference.
tSodium intake could be estimated in 85 subjects (40 men).
2.4 (0.2-14)
29.6 (0-84)
0.35 (0-1.2)
3.6 (0-11.9)
182+51
2.4+0.6
44±3
5.4 (1.5-30.4)
Women
(n=49)
1.7 (0-8.8)
7.5 (0-65)
0.13 (0-1.0)
3.4 (0-11)
134+38
2.2+0.6
39±3
4.2 (1.6-19.4)
of normally distributed data.
p*
.025
.005
.037
.584
<.001
.093
<.001
.159
Kupari et al Correlates of Left Ventricular Mass
1045
TABLE 4. Correlation of Left Ventricular Mass With Anthropometric and Lifestyle Characteristics
Partial Correlation Coefficient After Adjustment for
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
Bivariate Correlation
Sex and Height
Characteristic
Coefficient
Sex
Height
Weight
Sex and Height
and Weight
Sex
-.41
-.36t
-.59*
Height
.19
.24*
.52t
Weight
.53*
.66t
.55t
.53t
Body mass index
-.28*
-.22*
.48*
.50*
.43t
.51t
Physical activity index§
.17
.02
.27*
.06
.33t
.03
.11
Occupational physical workload
.05
-.01
.18
.01
.14
Smoking
.07
.06
.09
.03
.04
.06
Ethanol consumption§
.20
.17
.06
.15
.08
.05
Coffee consumption
.01
.09
-.01
-.02
.06
.05
Sodium intake
.41*
.43*
.45*
.59t
.35t
.43t
Results are based on data in 89 subjects (42 men) regarding all other variables except sodium intake, which was available in 83
subjects (40 men). The bivariate correlation coefficients are Pearson's product-moment coefficients (continuous variables) or
Spearman's rank correlation coefficients (categorical variables).
*P<.05, tP<.01, *P<.001.
§Square-root transformed data.
Values assigned to categorical variables-sex: male, 0; female, 1; smoking: nonsmoker, 0; 1 to 10 cigarettes per day, 1; >10
cigarettes per day, 2; occupational physical workload: minimal, 0; light, 1; moderate, 2; heavy, 3.
together for weight in the model for LV mass in all
subjects (see Table 6). The regression of LV mass on the
obesity category was statistically significant (b=13.3+5.2
g, P=.012), but the regression on height was not. The
significance of all other factors persisted, and model R2
was .685. The role of blood pressure measurements other
than the brachial artery systolic pressure was studied by
substituting them one at a time for the latter in the basic
equation (Table 6, all subjects). Diastolic brachial artery
blood pressure was fully interchangeable with systolic
blood pressure; the regression of LV mass was statistically
significant (b= 1.28+0.39 g/mm Hg, P=.002), as were all
other regressions resulting in a model R2 of .690. Both the
5-minute average of the systolic finger blood pressure
(b=0.39+0.21 g/mm Hg, P=.058; model R2=.660) and its
peak at the Valsalva test (b=0.27+0.12 g/mm Hg, P=.023;
model R2=.665) were somewhat weaker correlates of LV
mass. The power of the systolic finger blood pressure did
not predict LV mass regardless of whether it was used
instead of or in addition to the systolic brachial blood
pressure.
Interaction Between Sodium Intake
and Blood Pressure
In studying the residuals of the basic model (Table 6,
all subjects), a statistically significant interaction
(P<.001) was found between sodium intake and systolic
blood pressure. Table 7 shows the results of adding the
term "sodium intake systolic brachial artery pressure"
into the equation. It should be noted that the individual
TABLE 5. Correlation of Left Ventricular Mass With Hemodynamic and Laboratory Measurements
Partial Correlation Coefficient After Adjustment for
Bivariate Correlation
Characteristic
Coefficient
Sex
Systolic brachial artery blood pressure
.33t
.40t
Diastolic brachial artery blood pressure
.33t
.33t
Finger arterial systolic blood pressure
5-Min average
.26*
.22*
Total power§
-.12
-.01
Peak value at the Valsalva test
.29*
.28t
Stroke volume
.60t
.42t
- .1
Peripheral arterial resistance
- .28t
Hematocrit
.56t
.30t
Serum insulinil
.24*
.28t
Results are based on measurements in 89 subjects. Bivariate correlation
*P<.05, tP<.01, *P<.001.
§Square-root transformed data.
!1Log-transformed data.
Height
.44t
.39t
.30t
-.15
.40t
.44*
Weight
.26*
.19
.24*
-.12
.31 t
Sex and Height
.38t
.37t
.24*
-.06
Sex and Height
and Weight
.25*
.23*
.21
-.04
.29*
.34t
.39*
.38t
.31t
- .09
- .01
- .02
- .07
.22*
.36t
.29t
.42t
.26*
.01
.24*
.04
coefficients are Pearson's product-moment coefficients.
1046
Circulation Vol 89, No 3 March 1994
TABLE 6. Independent Correlates of Left Ventricular Mass Based on Multiple Linear Regression Analyses in All
Subjects and Separately in Men and Women
All Subjects (n=83)
Women (n=43)
Men (n=40)
Variable
b
P
SE
P
b
SE
b
SE
P
Body weight, kg
1.03
0.33
.002
t
t
t
1.42
0.31
<.001
Systolic blood pressure, mm Hg*
0.87
0.26
.001
0.41
1.31
.003
t
t
t
Stroke volume, mL
1.23
0.36
.001
1.37
0.50
.010
1.34
0.60
.033
Sodium intake, mEq/d
0.17
0.07
.033
0.24
0.12
0.17
.045
0.09
.052
Physical activity index, VMET- h/d
12.4
5.6
.029
t
t
16.0
5.3
t
.005
Hematocrit, %
2.1
1.0
.051
t
t
t
t
t
t
-214
Constant, g
-99
-63
R2
0.693
0.451
0.618
*Brachial artery cuff blood pressure.
tRegression was not statistically significant.
b indicates multiple linear regression coefficient; MET, metabolic equivalent (z1 kcal kg` * h-1); P, statistical significance of the
coefficient; R2, squared multiple correlation coefficient; and SE, standard error of the coefficient.
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
coefficients of sodium intake and systolic blood pressure, which now have a negative sign, cannot be used in
isolation from their product term to predict LV mass.
The explanatory power of the model increased from
69% to 75%.
For further analyses, the subjects were divided into
groups of "low" and "high" systolic blood pressure at
the population median of 121 mm Hg. Table 8 summarizes the regressions of LV mass on weight, systolic
blood pressure, stroke volume, sodium intake, physical
activity, and hematocrit in these groups, and Fig 1
highlights the group difference in the association of LV
mass with sodium intake. Although there appeared to
be differences in the regressions of LV mass on other
factors, too-weight and physical activity in particular
(see Table 8) -the standard errors of the coefficients
were large, and these differences were not statistically
significant. The subgroups by blood pressure were divided further into groups of low and high sodium intake
at the population median of 148 mEq/d. Fig 2 compares
TABLE 7. Prediction of Left Ventricular Mass With a
Regression Equation Including Interaction of Systolic
Blood Pressure and Sodium Intake
Variable
b
SE
P
Body weight, kg
1.00 0.30
.001
-1.50 0.67
Systolic blood pressure, mm Hg
.029
Stroke volume, mL
1.11 0.33
.001
Sodium intake, mEq/d
-1.56 0.47
.001
Physical activity index, A/MET- h/d
14.51 5.16
.006
Hematocrit, %
2.69 1.00
.009
Systolic blood pressure sodium intake,
mm Hg mEq
0.014 0.004 <.001
74
Constant, g
R2
0.751
b indicates multiple linear regression coefficient; MET, metabolic equivalent ('1 kcal * kg 1 h- 1); P, statistical significance of
the coefficient; R2, squared multiple correlation coefficient; and
SE, standard error of the coefficient.
Model was constructed in the total study population (n=83) by
adding the interaction term to the basic model shown in Table 6.
the mean values of LV mass (adjusted for weight, stroke
volume, physical activity, and hematocrit) across the
four subgroups. Persons with both systolic blood pressure and sodium intake below the median had an LV
mass of 161±20 g compared with 153±18 g in subjects
with high blood pressure alone (P=.425), 165±29 g in
persons with high sodium intake alone (P=.685), and
186±42 g in subjects with both high systolic blood
pressure and high sodium intake (P=.004).
Discussion
Our study showed that as much as 75% of the
cross-sectional variation in LV mass can be attributed to
weight, blood pressure, stroke volume, leisure-time
physical activity, sodium intake, and hematocrit in unselected persons aged 36 to 37 years. The contributions
of stroke volume, sodium intake, and hematocrit were
demonstrated for the first time in a population-based
study. However, the most outstanding finding was the
synergistic interaction of blood pressure and salt intake;
LV mass was particularly high in persons whose blood
pressure and salt intake were both in the upper half for
the study population.
Methodological Considerations
Our study group was a fully random sample of people
living in our area and borne in 1954. The sample can be
considered representative of the target population because the participation rate was close to 80% .25 The age
criterion was used to recruit an age-homogeneous cohort with a low prevalence of heart diseases; we wanted
to reduce the number of confounding factors in the
statistical analyses.
The quantification of the lifestyle variables was made
with 2-month prospective daily recording instead of
retrospective questioning, which has been relied on in
earlier studies.4-6,10,26 We aimed at obtaining as accurate
lifestyle information as possible for the last 6 to 8 weeks
preceding the ultrasound study because the LV mass
can change within days to a few weeks of changes in
physical activity or salt intake.27.28 The physical activity
index that we used is similar in principle to previously
described instruments,15 except the activity data were
collected prospectively in the present study.
Kupari et al Correlates of Left Ventricular Mass
1047
TABLE 8. Regression of Left Ventricular Mass on Body Weight, Systolic Blood Pressure, Stroke Volume, Sodium
Intake, Physical Activity, and Hematocrit in Subjects With Systolic Brachial Artery Blood Pressure Below or Above
Population Median (121 mm Hg)
Variable
Body weight, kg
Systolic blood pressure, mm Hg
Sodium intake, mEq/d
Stroke volume, mL
Physical activity index, VMET* h/d
Hematocrit, %
Constant, g
Systolic Blood Pressure <121
Systolic Blood Pressure .121
mm Hg (n=42)
mm Hg (n=41)
R2
P
.006
SE
0.49
0.72
0.10
0.51
5.8
1.21
b
1.41
1.17
-0.15
1.07
20.8
2.55
-243
0.724
.111
.141
.049
.001
.043
b
0.62
1.38
SE
0.42
0.53
0.41
1.17
7.3
3.43
-340
0.11
0.44
8.2
1.63
P
.149
.015
.001
.012
.433
.052
0.772
b indicates multiple linear regression coefficient; MET, metabolic equivalent (---1 kcal * kg` h-1); P, statistical significance of the
coefficient; R2, squared multiple correlation coefficient; and SE, standard error of the coefficient.
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
The assessment of salt intake was based on diet
records designed, accepted, and analyzed by an expert
nutritionist. The calculated sodium intake included not
only the sodium in the natural and commercial processed foods but also the average sodium added during
cooking with standard Finnish recipes.16 In the previous
studies on salt and LV mass, sodium intake was estimated by 8-1o to 24-hour89 urine collections. We did not
measure urinary sodium, but earlier research has shown
that sodium intake by food records correlates well with
24-hour urinary sodium and can be used to estimate salt
intake.29
The key echocardiographic measurements of this study
have been validated previously by other researchers.2223
We showed, however, that the reproducibility of these
methods in our hands was sufficient and comparable with
the experience of other echocardiographers.30 Regarding
the statistical methods, all main results and conclusions
derived from multivariate analyses combining men
and women. Although the sex-specific regression equations were not identical (Table 6), the lack of sex interactions in the model for both sexes suggests that the regression slopes were not statistically significantly different in
men and women. Admittedly, the relatively small total
sample size may have limited the power of our statistical
analyses (particularly in the subgroups) to identify true
associations or interactions.
were
Correlates of LV Mass
Body Size and Obesity
Of the variables characterizing body habitus, weight
predicted the LV mass better than height or body mass
index. Regarding the quantitative association of LV
mass with weight, the data in Tables 6 and 7 suggest that
300
300
a
Systolic blood pressure <121 mmHg
to
y=0.03x+1 59
r=0.06
p=0.7 1
250
a
5
5
Systolic blood pressure >121 mmHg
y=0.45x+1 03
" 250
r=0.61
p<0.00l
a
. 0
0
200
200
0
j
a* --,
*0
150
150
*
.
0
.
100
0
100
40
92
144
196
248
300
40
92
144
196
248
300
Sodium intake (meq/day)
Sodium intake (meq/day)
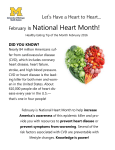
FIG 1. Plots of relation of left ventricular mass to sodium intake in people with systolic blood pressure below (left) or above (right) the
population median of 121 mm Hg. Left ventricular mass data are adjusted for the effects of weight, stroke volume, physical activity, and
hematocrit using the regression coefficients in Table 6 (all subjects). Note that left ventricular mass is unrelated to sodium intake in
subjects with "low" blood pressure, but a strong positive association is found in those with "high" systolic blood pressure.
1048
Circulation Vol 89, No 3 March 1994
200
190
oo 190
-,-
1
9
F=4.63
p=0.005
0 170
.~160
,~150
140
130
Na-intake <148
<121
SBP
25
n
<148
>121
>148
<1 21
18
>148 (meq/day)
>121 (mmHg)
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
1S
25
FIG 2. Bar graph of left ventricular mass in the subgroups of the
study formed by classifying the participants according to sodium
(Na) intake and systolic blood pressure (SBP). Group means
are, from left to right, 161 g, 153 g, 165 g, and 186 g. Bars
indicate standard errors. Overall statistical difference across the
groups is shown. In separate comparisons, people with both Na
intake and SBP above the population median (right) differed
from each of the other groups (P<.004), but differences across
the three groups with Na intake, SBP, or both below the median
were not statistically significant. Left ventricular mass data are
adjusted for the effects of weight, stroke volume, physical
activity, and hematocrit using the regression coefficients in Table
6 (all subjects).
each 1-kg difference in weight could explain an average
increment of 1 g in LV mass. To distinguish between the
effects of body stature and obesity (weight reflects them
both), we constructed an alternative model for LV mass
by substituting height and body mass index category for
weight. The data suggest that marked obesity (body
mass index, >30 kg/m2) could explain an increment of
27 g in LV mass compared with nonobesity (body mass
index, 20 to 25 kg/m2). In previous studies of hypertensive10 or mixed normotensive and hypertensive persons,31 a difference of 10 kg/mi2 in body mass index
explained 34-g10 to 45_g31 increments in the LV mass by
echocardiography. In the Framingham population free
of cardiopulmonary disease, the difference in age-adjusted LV mass/height between obese (body mass index,
>28 kg/M2) and lean people (body mass index, <24
kg/M2) was 18 g/m for men and 20 g/m for women.32
Other reports also support the key role of obesity as a
predictor of high LV mass.33,34
Physical Activity
The LV mass was associated with leisure-time physical activity more strongly in this study than has been
reported previously.4.26 According to the regression
coefficients (Tables 6 and 7), an energy expenditure of
2 kcal . kg- 1 . d-1 (1000 kcal/wk in a 70-kg person) could
explain a 17- to 20-g increment in LV mass. The
association tended to be more clear in women, although
no statistically significant sex interaction was observed.
In the Framingham population, a similar activity level
explained only a 2.5- to 4.6-g change in LV mass in
young men; no association was found in women or in
older men.4 Washburn et a126 reported that expenditure
of 1000 kcal/wk in leisure-time physical activity explained a 3 -g/m2 difference in ratio of LV mass to body
area, but only men were studied. These varying results
may reflect differences in the study groups and in the
assessment of physical activity. Contrary to our prospective method, the other works estimated leisure-time
activity for a 1-year period with retrospective recalls.4,26
Furthermore, the temporal relation of the ultrasound
study to the period covered by the recall was not
specified in either study.
Stroke Volume
Previous work by Ganau et al12 has suggested that
stroke volume is an essential determinant of LV mass
along with systolic blood pressure and contractility.
Other studies, by contrast, have found no independent
relation of LV mass to stroke volume in hypertensives8
or in selected hypertensive and normotensive persons.11
In our study, stroke volume predicted LV mass even
after adjustment for blood pressure and several other
variables, including weight as a measure of body size
(see Tables 6 through 8).
Blood Pressure and Sodium Intake
Our data are consistent with the well-known association of LV mass with blood pressure.3-12,31 Ambulatory
or exercise blood pressure may35,36 predict the LV mass
better than casual readings, but such measurements
could not be not evaluated in this study. Instead, we
used continuous finger arterial pressure monitoring to
quantify the beat-to-beat variation of systolic blood
pressure and its behavior in the Valsalva test. The
overshoot of blood pressure after the release of strain in
the Valsalva maneuver results from a sudden increase of
cardiac output at a time of peripheral vasoconstriction.37 We reasoned that the resulting peak of systolic
blood pressure could reflect the reactivity of blood
pressure and serve as a useful predictor of the LV mass.
However, the peak blood pressure at the Valsalva test
was no better predictor of LV mass than the average of
three casual brachial cuff measurements. The LV mass
was fully unrelated to the beat-to-beat variation of the
resting systolic blood pressure.
The relation of LV mass to sodium intake has been
shown previously in experimental animals38 and in selected people with8-10,28 or without9 hypertension. The
mechanism of this association is unknown, but direct
effects of sodium on the myocyte, modulation of neurohormonal systems, and effects on the intravascular
volume state have been proposed. As a novel finding,
our study uncovered a synergistic interaction of sodium
intake with blood pressure regarding association with
LV mass. Importantly, neither blood pressure nor salt
intake alone above the population median predicted an
increased LV mass (Fig 2), but when both were high,
the LV mass was clearly elevated. Experiments in
animals have shown that a sodium-deficient diet reduces
heart weight in hypertension but has no effect in normotension,38 which supports the possibility of a saltblood pressure interaction. On the other hand, Du
Cailar et a19 reported that LV mass was positively
related to sodium excretion both in normotensive subjects and in hypertension. Their work was not a population-based study, however.
The mechanisms underlying the sodium-blood pressure interaction cannot be deduced from our data.
However, because dietary sodium can modulate the
signals for synthesis of myocardial proteins,38 we spec-
Kupari et al Correlates of Left Ventricular Mass
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
ulate that higher sodium intake might sensitize the
heart to the hypertrophic stimulus of pressure load.
Ferrara et a128 have reported that the percent reduction
of LV mass induced by salt depletion in hypertension
increases proportionately with initial LV mass. They
believed that reduction of dietary sodium might interfere with the mechanisms modifying LV mass in
hypertension.
Hematocrit
Whole-blood viscosity has also been raised as a factor
possibly influencing the LV mass.'439 In normal adults,
hematocrit is the main determinant of whole blood
viscosity and explains about four fifths of its variation.40
We used hematocrit as a surrogate of blood viscosity
and found that it was an independent although relatively weak predictor of LV mass. Each 1% difference in
hematocrit could on average explain a 2.1- to 2.7-g
difference in the LV mass. One earlier report on
hypertensive subjects8 found an association of hematocrit with LV wall thickness, but not with LV mass, and
another study in children41 showed a univariate but no
multivariate association of LV mass with hemoglobin.
Other Factors
Many3"10 although not all8 earlier reports have shown
that men have higher LV mass than women even after
adjustment for body size. We found a similar difference
(see Tables 2 and 4), which, however, disappeared when
the hemodynamic, lifestyle, and laboratory characteristics were included in the analysis. This suggests that the
sex difference in the body size-adjusted LV mass was
attributable to differences between men and women in
the other independent factors of the multivariate
model. It is noteworthy in this respect that systolic blood
pressure, hematocrit, and physical activity were higher
in men and that the sex difference in stroke volume
persisted after adjustment for height and weight.
Trophic neurohormonal influences on the myocardium have also been implicated as determinants of LV
mass, particularly in hypertension.42-44 Evidence for
their significance is weak, however. In the study of
Schmieder et al,8 LV mass was unrelated to plasma
catecholamines, renin, angiotensin, or aldosterone. Two
other studies43,44 have found a relation of LV mass to
plasma renin in hypertension, but, confusingly, the
relation was negative in one43 and positive in the
other.44 We did not assess these factors, but we showed
that serum insulin does not predict LV mass independently of body weight. Finally, LV mass has been
associated with smokings"1043 and alcohol intake.5 Our
data did not confirm these findings, but we did not
estimate the lifetime ethanol consumption, which has
been claimed to be superior to current drinking as a
predictor of LV mass.45 We have shown that LV mass
increases with chronic alcohol abuse.46
Conclusions and Implications
Our study shows that up to three fourths of the
variation of LV mass in a population sample aged 36 to
37 years can be attributed to body weight, systolic blood
pressure, stroke volume, sodium intake, leisure-time
physical activity, and hematocrit. Increases of LV mass
with higher values of these factors are consistent for
each variable apart from sodium intake and blood
1049
The interaction of these two factors makes the
relation of LV mass to salt intake critically dependent
on the level of blood pressure (and vice versa). The data
in Table 8 suggest that a 100-mEq/d difference upward
in sodium intake could explain an increment between 19
g and 63 g (95% confidence interval) in the LV mass if
the systolic blood pressure is in the upper half for the
population, but a change between a 5-g increase and a
35 -g decrease (ie, no systematic change) in persons with
lower blood pressure. These findings are of potential
epidemiological and clinical importance but suffer from
the limitations of the cross-sectional design and the
relatively small sample size of our study. More firm
conclusions must await clinical experiments on how
manipulation of dietary sodium influences LV mass in
pressure.
relation to blood
pressure
and habitual salt intake.
Acknowledgments
This work was supported by a grant from the Foundation for
Alcohol Studies, Helsinki, Finland. We are grateful to Markku
Ventila, MSc, Marjaana Lahti-Koski, MSc, Tuovi Pekuri, RN,
and Soili Sirenius, RN, for help and skillful assistance during
the study. The technical support of Christian Nissen, Inc,
Helsinki, Finland, is also acknowledged.
References
1. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med.
1990;322:1561-1566.
2. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Left
ventricular mass and incidence of coronary heart disease in an
elderly cohort: the Framingham Heart Study. Ann Intern Med.
1989;110:101-107.
3. Levy D, Anderson KM, Savage DD, Kannel WB, Christiansen JC,
Castelli WP. Echocardiographically detected left ventricular
hypertrophy: prevalence and risk factors. Ann Intern Med. 1988;
108:7-13.
4. Savage DD, Levy D, Dannenberg AL, Garrison RJ, Castelli WP.
Association of echocardiographic left ventricular mass with body
size, blood pressure and physical activity (the Framingham Heart
Study). Am J Cardiol. 1990;65:371-376.
5. Manolio TA, Levy D, Garrison RJ, Castelli WP, Kannel WB.
Relation of alcohol intake to left ventricular mass: the Framingham Heart Study. JAm Coll Cardiol. 1991;17:717-721.
6. Galderisi M, Anderson KM, Wilson PWF, Levy D. Echocardiographic evidence for the existence of a distinct diabetic cardiomyopathy (the Framingham Heart Study). Am J Cardiol. 1991;68:
85-89.
7. Lauer MS, Levy D, Anderson KM, Plehn JF. Is there a relationship between exercise systolic blood pressure response and left
ventricular mass? The Framingham Heart Study. Ann Intern Med.
1992;116:203-210.
8. Schmieder RE, Messerli FH, Garavaglia GE, Nunez BD. Dietary
salt intake: a determinant of cardiac involvement in essential
hypertension. Circulation. 1988;78:951-956.
9. Du Cailar G, Ribstein J, Daures J-P, Mimran A. Sodium and left
ventricular mass in untreated hypertensive and normotensive
subjects. Am J Physiol. 1992;263:H177-H181.
10. Liebson PR, Grandits G, Prineas R, Dianzymba S, Flack JM,
Cutler JA, Grimm R, Stamler J. Echocardiographic correlates of
left ventricular structure among mildly hypertensive men and
women in the Treatment of Mild Hypertension Study (TOMHS).
Circulation. 1993;87:476-486.
11. Messerli H, Sundgaard-Riise K, Ventura HO, Dunn FG, Oigman
W, Frolich ED. Clinical and hemodynamic determinants of left
ventricular dimensions. Arch Intern Med. 1984;144:477-481.
12. Ganau A, Devereux RB, Pickering TG, Roman MJ, Schnall PL,
Santucci S, Spitzer MC, Laragh JH. Relation of left ventricular
hemodynamic load and contractile performance to left ventricular
mass in hypertension. Circulation. 1990;81:25-36.
13. Uusitupa M, Siitonen 0, Pyorala K, Mustonen J, Voutilainen E,
Hersio K, Penttild I. Relationship of blood pressure and left ventricular mass to serum insulin levels in newly diagnosed non-
1050
Circulation Vol 89, No 3 March 1994
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
insulin-dependent (type 2) diabetic patients and in non-diabetic
subjects. Diabetes Res. 1987;4:19-25.
14. Devereux RB, Drayer JIM, Chien S, Pickering TG, Letcher RL,
DeYoung JL, Sealey JE, Laragh JH. Whole blood viscosity as a
determinant of cardiac hypertrophy in hypertension. Am J Cardiol.
1984;54:592-595.
15. Wilson PWF, Paffenbarger RS, Morris JN, Havlik RJ. Assessment
methods for physical activity and physical fitness in population
studies: report of a NHLBI workshop. Am Heart J. 1986;111:
1177-1192.
16. Rastas M, Seppanen R, Knuts L-R, Karvetti R-L, Varo P, eds.
Nutrient Composition of Foods. 2nd ed. Hameenlinna: Karisto;
1989:1-457.
17. Boehmer RD. Continuous, real-time, noninvasive monitor of blood
pressure: Penaz methodology applied to the finger. J Clin Monit.
1987;3:282-287.
18. Virolainen J. Use of non-invasive finger blood pressure monitoring
in the estimation of aortic pressure at rest and during the Mueller
manoeuvre. Clin Physiol. 1992;12:619-628.
19. Kupari M, Virolainen J, Ventila M. Respiratory variation of heart
rate and systolic arterial pressure in adults with atrial septal defect.
Am J Cardiol. 1992;70:1615-1617.
20. Kupari M. Reproducibility of M-mode echocardiographic assessment
of left ventricular function: significance of the temporal range of
measurements. Eur Heart J. 1984;5:412-418.
21. Troy BL, Pombo J, Rackley CE. Measurement of left ventricular
wall thickness and mass by echocardiography. Circulation. 1972;45:
602-611.
22. Devereux RB, Alonso DL, Lutas EM, Gottlieb GJ, Campo E,
Sachs I, Reichek N. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J
Cardiol. 1986;57:450-458.
23. Lewis JF, Kuo LK, Nelson JG, Limacher MC, Quinones MA.
Pulsed Doppler echocardiographic determination of stroke volume
and cardiac output: clinical validation of two new methods using
the apical window. Circulation. 1984;70:425-431.
24. Kupari M, Koskinen P. Systolic flow velocity profile in left ventricular outflow tract in persons free of heart disease. Am J Cardiol.
1993;72:1172-1178.
25. Evans SJW. Good surveys guide. Br Med J. 1991;302:302-303.
26. Washburn RA, Savage DD, Dearwater SR, LaPorte RE,
Anderson SJ, Brenes G, Adams LL, Lee HKM, Holland J, Cowan
M, Parks E. Echocardiographic left ventricular mass and physical
activity: quantification of the relation in spinal cord injured and
apparently healthy active men. Am J Cardiol. 1986;58:1248-1253.
27. Ehsani AA, Hagberg M, Hickson RC. Rapid changes in left ventricular dimensions and mass in response to physical conditioning
and deconditioning. Am J Cardiol. 1978;42:52-56.
28. Ferrara LA, de Simone G, Pasanisi F, Mancini M, Mancini M. Left
ventricular mass reduction during salt depletion in arterial hypertension. Hypertension. 1984;6:755-759.
29. Pietinen P. Estimating sodium intake from food consumption data.
Ann Nutr Metab. 1982;26:90-99.
30. Wallerson DC, Devereux RB. Reproducibility of echocardiographic left ventricular measurements. Hypertension. 1987;9(suppl
ll):11- 6-11-18.
31. Hammond IW, Devereux RB, Alderman MH, Laragh JL. Relation
of blood pressure and body build to left ventricular mass in nor-
motensive and hypertensive employed adults. J Am Coll Cardiol.
1988;12:996-1004.
32. Lauer MS, Anderson KM, Levy D. Separate and joint influences of
obesity and mild hypertension on left ventricular mass and
geometry: the Framingham Heart Study. JAm Coll Cardiol. 1992;
19:130-134.
33. Messerli FH, Sundgaard-Riise K, Reisin ED, Dreslinski GR,
Ventura HO, Oigman W, Frolich ED, Dunn FG. Dimorphic adaptation to obesity and arterial hypertension. Ann Intern Med. 1983;
99:757-761.
34. MacMahon SW, Wilcken DEL, Macdonald GJ. The effect of
weight reduction of left ventricular mass: a randomized controlled
trial in young, overweight hypertensive patients. N Engl J Med.
1986;314:334-339.
35. Devereux RB, Pickering TG, Harshfield GA, Kleinert HD, Denby L,
Clark L, Pregibon D, Jason M, Kleiner B, Borer JS, Laragh JH. Left
ventricular hypertrophy in patients with hypertension: importance of
blood pressure response to regularly recurring stress. Circulation.
1983;68:470-476.
36. Ren JF, Hakki AH, Kotler MN, Iskandrian AS. Exercise systolic
blood pressure: a powerful determinant of increased left ventricular mass in patients with hypertension. J Am Coll Cardiol.
1985;5:1224-1231.
37. Gorlin R, Knowles JH, Storey CF. The Valsalva maneuver as a test
of cardiac function: pathologic physiology and clinical significance.
Am J Med. 1957;22:197-203.
38. Sen S, Young DR. Role of sodium in modulation of myocardial
hypertrophy in renal hypertensive rats. Hypertension. 1986;8:
918-924.
39. de Simone G, Devereux RB, Roman MJ, Ganau A, Chien S,
Alderman MH, Atlas S, Laragh JH. Gender differences in left
ventricular anatomy, blood viscosity and volume regulatory
hormones in normal adults. Am J Cardiol. 1991;68:1704-1708.
40. de Simone G, Devereux RB, Chien S, Alderman MH, Atlas SA,
Laragh JH. Relation of blood viscosity to demographic and physiologic variables and to cardiovascular risk factors in apparently
healthy adults. Circulation. 1990;81:107-117.
41. Daniels SD, Meyer RA, Loggie JMH. Determinants of cardiac
involvement in children and adolescents with essential hypertension. Circulation. 1990;82:1243-1248.
42. Frohlich ED, Apstein C, Chobanian AV, Devereux RB, Dustan
HB, Dzau V, Fauad-Tarazi F, Horan MJ, Marcus M, Massie B,
Pfeffer MA, Re RN, Roccella EJ, Savage D, Shub C. The heart in
hypertension. N Engl J Med. 1992;327:998-1008.
43. Hammond IW, Devereux RB, Alderman MH, Lutas EM, Spitzer
MC, Crowley JS, Laragh JH. The prevalence and correlates of
echocardiographic left ventricular hypertrophy among employed
patients with uncomplicated hypertension. JAm Coll Cardiol. 1986;
7:639-650.
44. Bauwens FR, Duprez DA, De Buyzere ML, De Backer TL,
Kaufman JM, Hoecke JW, Vermeulen A, Clement DL. Influence
of the arterial blood pressure and nonhemodynamic factors on left
ventricular hypertrophy in moderate essential hypertension. Am J
Cardiol. 1991;68:925-929.
45. Urbano-Marquez A, Estruch R, Navarro-Lopez F, Grau JM, Mont
L, Rubin E. The effects of alcoholism on skeletal and cardiac
muscle. N Engl J Med. 1989;320:409-415.
46. Kupari M, Koskinen P, Suokas A. Left ventricular size, mass and
function in relation to the duration and quantity of heavy drinking
in chronic alcoholics. Am J Cardiol. 1991;67:274-279.
Correlates of left ventricular mass in a population sample aged 36 to 37 years. Focus on
lifestyle and salt intake.
M Kupari, P Koskinen and J Virolainen
Downloaded from http://circ.ahajournals.org/ by guest on June 15, 2017
Circulation. 1994;89:1041-1050
doi: 10.1161/01.CIR.89.3.1041
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1994 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circ.ahajournals.org/content/89/3/1041
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial
Office. Once the online version of the published article for which permission is being requested is located,
click Request Permissions in the middle column of the Web page under Services. Further information about
this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/