Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
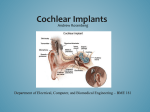
Cochlear Implants A guide for families Our vision is of a world without barriers for every deaf child. Contents Introduction p4 What is a cochlear implant? What does a cochlear implant consist of? How does a cochlear implant work? Deciding to have cochlear implants Who is suitable for a cochlear implant? What age can my child have a cochlear implant? The assessment process During the assessment process At the end of the assessment process Which cochlear implant for my child? One ear or two? Funding Surgery Risks of surgery Switch on After the operation and tuning Growing up with an implant Assistive Listening Devices Lost or damaged processors p5 p5 p6 p8 p10 p11 p12 p13 p14 p15 p16 p17 p18 p19 p20 p21 p24 p28 p29 Where to go for more information p31 Thank you to the following companies for their permission to print photographs and images in this booklet: Cochlear UK (www.cochlear.com), Advanced Bionics (www.advancedbionics.com), MED-EL (www.medel.com/uk). 3 Introduction If your child has a severe to profound permanent deafness and cannot hear speech sounds with hearing aids, you may be thinking about them having a cochlear implant. To make a decision on what’s best for your child it’s important that you have as much information about the process as possible. The aim of this book is to give you clear, balanced and accurate information about cochlear implants. This booklet is divided into three parts: about cochlear implants, the assessment process, using a cochlear implant. On the NDCS website you will find links to further information about cochlear implants, written stories from families and young deaf people who have been through the process of considering cochlear implants, and videos of families who share their experiences at www.ndcs.org.uk/family_support/audiology/cochlear_implants/index.rma. At the end of the booklet you will find the contact details of other groups and organisations who work with children and adults who use cochlear implants and can share their personal experiences and provide further information. 4 What is a cochlear implant? A cochlear implant is a type of hearing aid that converts sound into electrical signals. Cochlear implants are for children and adults who gain limited or no benefit from hearing aids. Instead of simply making sounds louder as with a conventional hearing aid, the cochlear implant provides a sensation of hearing by bypassing the damaged hair cells in the cochlea and directly stimulating the auditory nerves using electrical signals. To date, there are around 12,000 people in the UK who use cochlear implants. Cochlear implants are unable to restore normal levels of hearing and the degree of hearing provided can vary from child to child. However, the majority of children who have permanent severe to profound deafness and who were unable to hear the full range of speech sounds with their hearing aids, are now able to access these and understand speech and language using only their cochlear implants. Other children are unable to follow conversation without additional visual information but the cochlear implants enable them to recognise voices and enhance their lipreading skills. A smaller number of children gain less benefit from their cochlear implants but have improved awareness of environmental sounds. Examples of cochlear implant systems External (behind-the-ear) External (behind-the-ear) External (behind-the-ear) Internal Internal Internal What does a cochlear implant consist of? There are several makes and models of cochlear implant available but they share similar design and features. Cochlear implants have two parts – an internal receiver which is implanted surgically and an external part which is worn like a hearing aid. The internal part is surgically implanted under the skin behind the ear and the electrodes are inserted inside the cochlea. The external part is known as a speech processor and includes the microphone. The speech processor is usually worn like a hearing aid behind the ear. For very young children and those with very small ears a separate battery pack may be worn clipped onto clothing and connected to the speech processor with a lead. 5 How does a cochlear implant work? To understand how a cochlear implant works, it is useful to know about how the ear works. The ear is made up of the outer, middle and inner ear. Working in synergy they enable us to hear and process sound. The ear has two main functions: it receives sound and converts it into signals the brain can understand, It helps us to balance. The two functions are closely connected. The ear is the first part of the hearing system. The pinna is the outer part of the ear that we can see. It collects sound waves and directs them down the ear canal towards the eardrum. The eardrum separates the outer ear from the middle ear. The middle ear is air-filled and contains three tiny bones (ossicles). These are called the malleus (also known as the hammer), the incus (also known as the anvil), the stapes (also known as the stirrup). Sound waves cause the eardrum to vibrate and these vibrations are passed across the middle ear by the three tiny bones. The bones increase the strength of the vibrations before they pass through the oval window into the cochlea. 6 The cochlea looks like a snail’s shell. It is filled with fluid and contains thousands of tiny sound-sensitive cells. These cells are known as cilia or “hair cells”. The vibration of the bones in the middle ear enters the cochlea and causes the fluid to move which in turn causes the hair cells to bend. The movement of the hair cells is similar to the movement of seaweed on the seabed when waves pass over it. As the hair cells move, they create a small electrical charge. This charge moves along the auditory nerve to the brain where it is converted into signals that can be understood. To be able to hear the full range of sounds, all of the hearing system must work well. Deafness occurs when at least one part of the hearing system is not working effectively. Implant in place Cochlear implants work as follows: The microphone of the cochlear implant picks up the sound and the speech processor converts the sound waves into a digital code which is then sent to the transmitter coil. The transmitter coil sends the coded signal through the skin to the implanted receiver which is located just under the skin. The receiver converts the digital code to an electrical signal. This signal is then sent from the implanted receiver via a wire to the electrodes in the cochlea. The electrodes stimulate the cochlear nerve fibres and they send the signal to the brain. The brain interprets these signals so the wearer can understand what was ‘heard’. The sound perceived through a cochlear implant is not the same as the sound heard with normal hearing. Cochlear implant wearers who have previously heard naturally often describe the sound as being robotic or tinny. However, with time the brain adjusts to the new signals and what is heard becomes more natural. 7 Deciding to have cochlear implants Before deciding to go ahead with a cochlear implant for your child, you will need time to think about the long-term commitment you are making. It is important to get balanced information during the assessment and about the surgery and followup care. If English is not your first language, ask for an interpreter to be present at meetings or for information to be translated. You can also phone our NDCS Freephone Helpline and arrange for our audiology adviser to phone you back with an interpreter. Having a cochlear implant means making a lifetime commitment to looking after it. This will involve regular visits to the cochlear implant centre, both before and after the surgery. You, your family and professionals will also need to provide a lot of long-term support for your child. It is also important to remember that when the speech processor is removed e.g. at bedtime, your child is still deaf. Families who go through the assessment process will make the decision on whether a cochlear implant is the right option for their child in partnership with the professionals from the cochlear implant team. For some families this can be a difficult decision as there are so many things to consider. Having lots of balanced information and speaking to families with experience of the process may help you make your decision. It is important that if your child is old enough, you and the professional involved listen to their feelings about cochlear implants and involve them as much as possible in making the decision. When you start thinking about cochlear implants and finding out more information about them you will come across different views regarding implanting children of a young age. Some people in the Deaf community do not feel that deafness needs to be cured and that a deaf child should be old enough to make their own decision before being implanted, whereas others see deafness as a condition which can be helped by technological intervention and that a cochlear implant can give a profoundly deaf child their best and only chance of gaining access to spoken language. If you are interested in finding out more about this debate, it is a good idea to talk to deaf people with and without cochlear implants and to families and deaf children themselves about their experiences and feelings. The useful contacts below may be helpful. Most parents find that the decision to proceed with the implant is an ongoing process throughout the assessment (see p12 for further information on the assessment process). If at any time, you or your child feels that having an implant is not the right choice, always feel free to say so. If you have any questions about the tests, the operation and what it is like to live with an implant, talk to the professionals working with you and your child. 8 it is important for your child’s self-esteem and confidence that they grow up knowing that they are deaf and feeling positive about their deafness. It is important that as children grow up they are given information about their cochlear implant and the opportunity to become independent in looking after it. That way they are more likely to become confident and be able to advocate more effectively for their needs as a teenager and young adult. If your child is older when you are first thinking about a cochlear implant it is important that they are fully involved in the assessment process, discussions and decision to have one. Whilst you are going through this process, it is advisable for both you and your child to talk with other families about their experiences of what it is like to have and also to live with an implant. You may also feel you would like to speak to deaf adults about their experiences. Useful contacts: CICS (Cochlear Implanted Children’s Support) Group is a voluntary group which is run by parents offering support to parents of deaf children about cochlear implants and those who are in the decision making process regarding cochlear implantation for their child (see the contact details on page 31). Children may like to talk to a trusted friend, family members or a trusted professional such as their Teacher of the Deaf or communication support worker. NDCS can put you in touch with a deaf role model: a deaf adult who will help promote a positive view of deafness and also be a positive role model for your child. Some deaf role models use implants, some hearing aids and some neither. Communication methods also vary amongst the role models and you can ask for a role model who closely matches your child’s experiences. The Buzz is a website run by NDCS for deaf children and young people to make friends, get support and share experiences. There are two separate sites: one for children aged 8-12, and one for young people aged 13-18: www.buzz.org.uk. Older children and teenagers can access information via www.ci-4teenz.com. The site gives a general overview of a cochlear implant, personal views from other teenagers on what it is like to wear a cochlear implant, including their experiences and journey from surgery to wearing an implant. There are fact files that target the different problems that implant users experience with solutions to try. The Ear Foundation is an organisation which supports deaf children, young people and adults. Their Family Programme is aimed at providing activities and opportunities for families to get together, share experiences and learn about the latest hearing technologies (see contact details on page 31). 9 Who is suitable for a cochlear implant? Guidelines were written by the National Institute for Health and Clinical Excellence (NICE) in 2009 with recommendations that: Cochlear implants should be considered for children with severe to profound deafness where they only hear sounds louder than 90 dB HL at 2000 and 4000 Hz in both ears without hearing aids, and when their speech, language and listening skills are behind that expected for their age, developmental stage and cognitive ability. NICE also recommend that: Cochlear implantation should be considered for children only after an assessment by a multidisciplinary team (see p12 for more information on the assessment process). As part of the assessment children should usually have a trial of appropriate hearing aids for at least 3 months. If appropriate, children should be offered bilateral cochlear implants (an implant in each ear), to be fitted during the same surgery. There are currently no guidelines for children who do not meet the above criteria but they may also be assessed at a cochlear implant centre and be considered on a case-by-case basis. These include children with Auditory Neuropathy Spectrum Disorder (ANSD), or children with unilateral (one-sided) deafness. An alternative auditory implant may be found to be more suitable for some children. Cochlear implant technology has developed rapidly in the last few years making more options and features available than ever before. Some children may be suitable for new electro-acoustic (hybrid) implants. This type of implant is for those with aidable low and mid frequency hearing but with a severe to profound loss in the high frequencies. The implant combines amplification of sound acoustically via the hearing aid part of the implant with electrical stimulation via the cochlear implant in the same ear. Overall this may give the individual greater speech recognition than with hearing aids or cochlear implants alone. For more information on ANSD, unilateral deafness or other auditory implants contact the NDCS Freephone Helpline. For more information on the assessment process and individual considerations see pages 12-17. 10 What age can my child have a cochlear implant? Babies who are born deaf or become deaf very early in childhood: Most newborn babies now have a hearing screen performed shortly after birth. This means that children who are born deaf are being identified and fitted with hearing aids at a very young age. In general, the evidence suggests that the younger a child is when they receive their cochlear implant, the more likely they are to get the most benefit from the device. It is important to remember that it takes some time to find out the exact level of a child’s hearing loss and the benefit received from their hearing aids. The cochlear implant team and surgeon will discuss with you the potential risks and benefits when deciding when to perform the surgery. It is now common for children to be implanted before 12 months of age. Early implantation and support is most likely to achieve the development of speech and language skills in a similar way to hearing children of the same age. The most intensive period for speech and language development is during the first three years of life when the brain develops and builds the neural pathways essential for processing auditory information. Older children and teenagers: Older children and teenagers may also be candidates for cochlear implants. This includes those who have become deaf after learning to speak (for example following meningitis), as well as those who have a progressive or acquired hearing loss and who now receive less benefit from their hearing aids. Some older children and teenagers may have been assessed for a cochlear implant when they were younger but were found not to fit the criteria to be implanted at that time. As the guidelines have evolved over time, those children who use hearing aids consistently and mainly use spoken language to communicate may now be considered suitable candidates for reassessment. 11 The assessment process The assessment is carried out at a specialist cochlear implant or auditory implant centre. There are a number of specialist centres around the UK and you will usually be referred to your nearest one. A list of centres is available at www.bcig.org.uk. If you haven’t been offered a referral, think your child may benefit from a cochlear implant, and would like to find out more, ask your ENT consultant, paediatrician, or audiovestibular physician for a referral. You may have to travel some distance to get to your nearest cochlear implant centre. You may be entitled to help with your travel costs through the Healthcare Travel Cost Scheme (HTCS) if you receive either Income Support, Income-based Jobseeker’s Allowance, Pension Credit Guarantee Credit, are named on an NHS tax exemption certificate or qualify under the NHS low-income scheme. The implant team will send you an appointment for an initial assessment to determine your child’s suitability for a cochlear implant. There will usually be a number of further appointments for detailed assessment involving a number of hearing tests and other assessments. This will help the implant team to build up a picture of your child’s deafness, how much benefit is obtained using their hearing aids, whether a cochlear implant is likely to provide additional benefit over their hearing aids, and their ability to make the most of a cochlear implant. The NHS in England has an expected maximum waiting time of 6 weeks for the first assessment and 18 weeks for treatment from the time of referral. The assessment period and surgery can usually be completed within this time. Occasionally the assessment period may take longer, for example if your child has additional needs or you want more time to think about the options available. Throughout the cochlear implant assessment process you will meet a multidisciplinary team including: audiologists, audiovestibular physicians, ENT consultants, speech and language therapists, Teachers of the Deaf, nursing staff, educational or clinical psychologists, radiologists. 12 During the assessment process: You will be given information about your child’s deafness, cochlear implants, the procedure and the habilitation programme after surgery. The implant team will work alongside the professionals that support your child locally. Appointments may be at the cochlear implant centre or at home and may include nursery or school visits. A full examination of your child’s ears will be carried out. If not already done, you will be offered further testing to try to find out the cause of their deafness (known as aetiological testing). Your child will receive a radiological assessment using MRI (Magnetic Resonance Imaging) and CT (Computerised Tomography) scanning. These tests look at the anatomy of the cochlea, the balance organs, auditory nerve (hearing nerve) and the brain. They also help to provide information as to whether it is possible to insert the electrodes. Your child will have detailed behavioural testing, with and without their hearing aids, to give a functional assessment of their level of hearing. Your child may have a further trial of hearing aids for at least 3 months. Your child will have objective hearing tests including auditory brainstem response (ABR) to confirm the function of the auditory nerve pathways. Evaluation of your child’s communication, language and speech skills will be undertaken. The tests may be carried out at the implant centre, at home, or at school by the implant centre’s Teacher of the Deaf and speech and language therapist. For further information on hearing tests and the medical tests used to try and determine the cause of deafness see the NDCS booklets Understanding your Child’s Hearing Tests and Genetic Counselling; Information for families. In addition to the various tests and assessments, the cochlear implant team will discuss the ongoing care and support that is necessary to help your child get the most benefit from the implant. They will look at the long-term support that will be provided by parents, family, the local authority and local audiology services. The cochlear implant team will recommend implantation only if your child has been through the assessment process, that you understand the commitment that is required to start this journey and you and the cochlear implant team agree that your child will consistently, continuously and effectively use a cochlear implant. The assessment process sometimes highlights issues or conditions that may affect the outcome of the assessment, or the expected outcomes with cochlear implants for the child. These rarely prevent proceeding with an implant but need to be understood and addressed during the assessment process: Glue ear is a very common condition during childhood caused by a build up of fluid in the middle ear. Glue ear is often temporary and may resolve without the need for any treatment. However, it may cause a child who has a moderate to severe deafness to 13 appear to have a much more significant hearing loss. This could mean that without glue ear, your child has enough hearing not to need a cochlear implant. It is therefore very important that glue ear is treated and your child has a hearing test once it has resolved to measure the true level of sensori-neural deafness. Children with additional needs can and do benefit from implants. Nowadays many deaf children with additional needs are implanted early in life before their other needs are identified or known about. Sometimes the assessment process helps identify other needs. Each child needs to be assessed as an individual. Very occasionally, it may be felt that a child’s additional needs could make it difficult or impossible to learn to use the new signal. The implant team will discuss this with you and make alternative recommendations for supporting your child if needed. Problems such as ossification following meningitis - new bone growth within the cochlea - can occur making it difficult for the surgeon to insert the electrodes. If there is partial ossification of the cochlear, then implantation is still possible and the results are usually still good. If there is complete ossification, surgery to implant may still be possible but is more difficult and the results can be variable. Very occasionally, children may be born without a cochlea or auditory nerve (hearing nerve). If the scan shows that either is absent, then it will not be possible to have a cochlear implant in that ear. The implant team may then discuss an Auditory Brainstem Implant (ABI). For further information on glue ear and its treatments, deaf children with additional needs, meningitis and childhood deafness, and Auditory Brainstem Implants contact the NDCS Freephone Helpline. At the end of the assessment process Most parents find that the decision whether or not to proceed with cochlear implants is an ongoing process throughout the assessment. If at any time, you or your child feels that having an implant is not the right choice, always feel free to say so. Where applicable, your child should also be involved in the decision making 14 process. If you have any questions about the tests, the operation and what it is like to live with an implant, talk to the professionals working with you and your child. Once all the assessments are complete the implant team will arrange to meet with you to share the results and advise on whether they feel cochlear implants will be suitable for your child. There will be times when the implant team feel that a child is not suitable for a cochlear implant. This could include the following: The results of the scan show that there is no cochlea or auditory nerve or there is a problem with the cochlea making an implant surgically impossible. Your child may have enough residual hearing to benefit from conventional hearing aids. The implant team will make recommendations on hearing aids and your local audiology department will continue to care for and support your child and monitor any changes in their hearing. If your child’s hearing changes in the future a referral back to the implant centre can be made for re-assessment. Once you and the implant team have made the decision to go ahead with the surgery they will arrange a pre-operative appointment with the ENT consultant. The ENT consultant will discuss the surgery and surgical risks with you. See p’s 18-19 for more information on the surgery. The implant team will also check that your child’s immunisations included the meningitis vaccination and recommend this is done before the surgery if it hasn’t been already. You may be offered a choice of implant system for your child, and whether your child is fitted with one or two cochlear implants. See the next section for further guidance on these choices. Which cochlear implant for my child? There are several different makes and models of cochlear implants but they all work in a similar way. Most UK implant centres will offer a choice of two or more devices. In the UK most children use cochlear implants manufactured by Cochlear, Advanced Bionics and Medel. There is currently no evidence that children perform better with one manufacturer’s device over another. Before you make a decision, you may wish to consider the following: Speak with other families about their experiences of and decisions about individual devices. Ask how many cochlear implants the surgeon has implanted of the make and model you are interested in, and the experience of the team, particularly in providing these implants to children. Cosmetic features of the cochlear implant, such as the size of the speech processor, how it fits on the ear and how it looks. Older children should be given as much choice as possible in how their implant looks. Reliability and robustness of the external parts of the cochlear implant. 15 Reliability and safety record of the internal implant. How many people are currently implanted with the make and model you are interested in and what is the expected life-span of the implant. This information can be found on the implant manufacturer’s website. Battery life and type of battery the implant uses. Can they be recharged? Will they last a whole day at school? How easy is it to tell if the battery has run down? Is the system easy to use? When fitted to young children, is it easy to tell if the implant is switched on and working well using the visual indicators? Is the device water resistant or waterproof? Compatibility of the implant with FM systems and other audio equipment. A brand comparison of the different cochlear implants can be viewed on www. cochlearimplantonline.com. How will changes in technology affect my child’s cochlear implant? The internal part of a cochlear implant (the part that is surgically implanted) is unlikely to need upgrading, unless there are problems. The external speech processor can be changed as technology develops and improves, but this should not mean further surgery. To keep up with changes in technology, it is recommended that speech processors are upgraded every five years, when these are available and suitable for the child. One ear or two? Hearing with two ears allows us to understand speech in background noise, and localise sounds i.e. work out which direction the sound is coming from. For children who gain little or no benefit from their hearing aids, the cochlear implant team may recommend having two cochlear implants (bilateral implants). It has been shown that children perform better with two implants rather than one alone. There may be occasions where the implant team recommend your child have a cochlear implant in one ear and continue wearing a hearing aid in the other ear, known as bimodal fitting. This will depend on the level of hearing and also the expected benefits of both options. If it is recommended that your child has one implant and continues to wear the hearing aid in the other ear, you will need to discuss which ear is to be implanted with the surgeon and audiologist. It is important to understand why the implant team recommends a particular ear be implanted instead of the other. It may be because of medical reasons (e.g. the scan may indicate why one ear should be implanted when compared to the other), or because of differing levels of hearing in each ear. For children with physical difficulties, the ear may be chosen for practical 16 reasons (e.g. one arm/hand may have better function than the other and be able to put on and adjust the speech processor more easily). “Simultaneous” bilateral cochlear implant means that your child will receive both implants at the same time i.e. one surgical procedure. Most children in the UK will have simultaneous bilateral cochlear implants now. “Sequential” implantation is where your child receives one implant and after a period of time receives the second implant i.e. two separate surgical procedures. Sequential implantation is done less often but may be done for older children who had their first implant several years ago before the current bilateral recommendations, or in children where the hearing in the second ear was originally better but has deteriorated over time. Funding The new Health and Social Care Act 2012 came into effect from April 2013. Cochlear implants are now funded centrally by NHS England. Provided children meet the identified candidature criteria as set out by NHS England, funding will be paid directly to your specialist service and individual families should not have to apply for funding. Candidature is often identified using recommendations made by the National Institute for Heath and Clinical Excellence (NICE). If a child does not exactly meet the criteria but it is still felt that an implantable device is the most appropriate clinical option for them, then an individual funding request may need to be made. Similar central funding and criteria for implantation are used in Wales, Scotland and Northern Ireland. 17 Surgery Many hospitals have information on their website with advice on preparing yourself and your child for a stay in hospital and surgery. Ask your implant team if they have a liaison nurse who can provide guidance about the ward you will be staying on. For general information see the NHS Choices website at www.nhs.uk/video/Pages/Childreninhospital.aspx . You could also ask other parents for their experiences via the Parent Place forum on the NDCS website or the NDCS group on Facebook. Parents who have already been through the process will often have valuable information that they could share on practical issues. The implant manufacturers also produce DVDs, online videos, children’s stories and colouring books with information specific to cochlear implant surgery which can help explain what is happening to young children. Surgery is usually carried out as a day case but occasionally may involve an overnight stay in hospital. Your child will be examined by the medical team and anaesthetist. You will then be required to fill in a consent form for your child. It is important that you read this carefully to make sure you understand the procedure and what the surgery involves. Ask your surgeon and anaesthetist if there is anything you are unsure about. The operation is performed under general anaesthetic and typically lasts between 2 to 3 hours. If your child is having two implants then the surgery will take longer. Sometimes a small amount of hair may need to be shaved behind the ear and then a small cut is made on the side of your child’s head. The internal receiver is inserted and secured beneath the skin and the electrode is inserted into the cochlea. Tests will be carried out to check it is working. The surgical wound is closed with dissolvable stitches underneath the skin so no stitches will need to be removed. 18 After the operation, you will be able to see your child in the theatre recovery area. A dressing may be placed around your child’s head, which will probably be removed the day after surgery. The implant surgeon will usually want to see you soon after the operation to explain how it went. Before leaving the hospital, you will be given a follow-up care plan. If there is anything you are unsure of, ask a member of the team or nursing staff. An X-ray may have already been done to show the position of the cochlear implant, but if not a separate appointment will be made. After leaving hospital although it is not necessary to see your GP, it is wise for your child to be seen by your local ENT consultant one week after the operation to check the wound is healing well. Children are typically up and about 1 to 2 days after surgery and the implant is activated around 3 to 4 weeks post surgery which allows enough time for the incision to have healed properly. Risks of surgery There are risks associated with any surgery that requires a general anaesthetic. With cochlear implant surgery there are some specific risks which your ENT doctor will discuss with you. Meningitis Although the risk of contracting meningitis in those with cochlear implants is very small, it is slightly higher than in the general population. Vaccination for meningitis is recommended before your child is given a cochlear implant and this is usually given by your GP. Facial nerve The facial nerve lies in close proximity to the area where the surgeon is operating. The risk of it being damaged is very small and monitors are used through the surgery to avoid the likelihood of this happening. Infection Although rare, infection around the implant site can occur which may require removal of the implant. If, after your child’s surgery, you are concerned that they might have an infection, contact the implant centre as soon as possible for advice. You can also contact your local ENT department and your GP for advice. Device failure The internal receiver package and electrode are sensitive electronic devices which occasionally stop working as they should. This will require surgery (known as reimplantation) to replace the device. Re-implantation is usually carried out quite successfully in the same ear. Some other side effects of the surgery include a metallic taste in the mouth and balance problems/dizziness. These are usually short-lived and not long-term problems. Should you have any concerns about the surgery, speak to your surgeon or any member of the implant team. 19 Switch on Three to four weeks after surgery an appointment is made to fit and start programming the external part of the cochlear implant, the speech processor. Each speech processor is individually programmed. The electrical signals produced by the speech processor are very complex and their levels need to be set carefully to suit your child. The process of programming the speech processor is known as “tuning” or “mapping”. Each electrode is stimulated one at a time to find the quietest sound threshold and then to find the level that is comfortably loud and tolerable. The measurements made help to develop an individual programme for your child’s speech processor. With bilateral implants, both the implants are gradually activated together. Frequent adjustments will be made in the beginning as your child starts to adapt to the new sounds. You should be warned by the audiologist that your child’s initial response to sound through the implant may not always be a positive one. Many young children smile or look surprised, but some cry and appear frightened. Your child may need lots of positive encouragement and time to adjust to the new signal. Each child is an individual and it is perfectly normal for a child to respond differently to another when the implant is activated. It may depend on your child’s previous experience with sound. 20 After the operation and tuning After the implant is fitted, your child will need long-term support from you, the cochlear implant team and local professionals. This support and care can make the difference between an implant being used effectively or less effectively. As a family, you need to know the vital role you and other carers of your child play in helping your child to use their implant and in supporting them to develop their listening, communication and language skills. Your child will continue to visit the clinic for the process of tuning their implant’s speech processor and making adjustments as they learn to interpret the new signals. It is important that you know the level of commitment that will be needed, particularly in the early years following implantation. Appointments at the implant centre mean you may need to take time off work and be away from the rest of your family. Ask your implant centre for a schedule of expected visits, both before and after the implant operation. The sessions in the clinic will include time for the audiologist to tune the processor. There may also be a medical check and sessions with the Teacher of the Deaf and a speech and language therapist. It is important that you, your child’s school and the cochlear implant centre keep in touch with each other so that there is good communication between all those caring for and working with your child. It also means that any problems with the equipment can be reported and sorted out quickly and that everyone will have access to the right spares and accessories. 21 The Teacher of the Deaf and speech and language therapist from the implant team may visit your child at home and school to observe and record your child’s progress. It can be advisable to keep notes of your own observations so you can discuss them with them. They will also be able to answer your questions, talk to you about how you can help your child and explain what you can realistically expect of your child’s progress. As your child becomes older, they need to learn about their implant so that they can become responsible for looking after it. They will learn when to contact the implant centre for changes to the tuning and for repairs, spares, testing and advice. All implant systems have handbooks and apps for users and it will be helpful for your child to become familiar with these. It is important that the implant team provides information that is easy to read and that your child will be able to understand. If your child develops glue ear or an infection in the implanted ear, it is important to contact your GP and get it treated quickly. You should also inform your cochlear implant team. 22 Communication and language It is important to remember that it may take a long time for your child to learn to interpret new sounds through the implant and it will require a lot of patience as well as practice. Every child is different and the time it takes will vary with each child. Your child will need to use these new sounds to develop their communication skills and spoken language. For a hearing child this process starts at birth and takes place over years whereas for a child fitted with an implant, the process might take even longer. Ask your speech and language therapist and Teacher of the Deaf for recommendations of games and activities that will help your child learn about new sounds and develop their listening skills. Additionally, the cochlear implant manufacturers have online resources aimed at children of all ages to help them learn to listen and to help with their language skills. It is important that your child wears their cochlear implants as much as possible so they can learn to recognise sounds and make sense of the sounds around them. Playing games, singing songs and reading stories will help to develop these skills. Always be aware of the listening conditions so that background noise is kept at a reasonable level. Ensure that the processors fit comfortably and securely so that children are able to wear them for all waking hours. Prior to implantation, sign language may have been your child’s main communication method as they did not have enough hearing to understand spoken language. There is still some conflict of opinions between professionals as to whether sign language should be used with children who have been implanted. Some professionals feel it hinders the development of spoken language while others feel it supports their communication. Most parents have found that once their child has adapted to the implant, the reliance on signing starts to diminish. The process of changing from sign-based communication to spoken communication occurs naturally, but for some children, sign language will remain an important part of their communication and identity. Regardless of which method is used, the most important factor is that your child can develop fluent language skills to communicate by whichever method is appropriate and most effective for them. The Ear Foundation carried out a three part study looking at parental perspectives on changing communication skills following implantation. Questionnaires and face to face interviews with the parents were carried out and the results and comments published in a joint booklet with NDCS, Children with Cochlear Implants: Parental perspectives on changing communication skills. Having an alternative method of communication, such as British Sign Language, is often beneficial if a situation arises that makes it impractical for your child to wear their implant such as when undertaking water-based activities, or when the speech processor is faulty. 23 Growing up with an implant Most young people who were given cochlear implants as young children, rely on and continue to use them into adulthood. It is important that teenagers are given up-to-date information about their cochlear implant system so that they can become independent in their understanding and care of the system and make informed choices about their own care. Researchers from the Ear Foundation interviewed young people on issues including the advantages and disadvantages of wearing an implant, understanding how the implant works, deciding to have an implant and advice to others. The findings are available in the NDCS resource Cochlear Implants: Young people’s views and can be ordered from NDCS. 24 Safety information Children with cochlear implants are able to take part in most activities, although sometimes it is advisable to remove the speech processor during the activity to prevent it being damaged for example, when taking part in football, netball and swimming. In order to avoid damaging the internal part of the implant, children with cochlear implants are advised to wear head protection for some activities and to avoid contact sports where a knock to the head is likely such as judo, kickboxing and rugby. The British Cochlear Implant Group (BCIG) issue guidelines which your implant centre should give you during the assessment. The BCIG is a professional body which represents all the people working in the cochlear implant centres in the UK. Their recommended guidelines include: sport, leisure and play, medical matters, security systems, flying and travel, employment issues e.g. safety at work, static electricity, interference from electrical equipment, use of personal stereos, audio equipment and TVs. It is important that you read these guidelines and talk to your cochlear implant team during the assessment process about any concerns you may have. You can also phone our Freephone Helpline to speak to our audiology adviser. You can obtain the most recent copy of the safety guidelines from your cochlear implant team or by visiting the BCIG website (www.bcig.org.uk). 25 Waterproof cochlear implants At the time of writing the only waterproof speech processor is the Neptune made by Advanced Bionics. Children who have compatible internal parts may be able to upgrade to the Neptune when their next routine upgrade is due. The Neptune can be submerged in water up to depths of 3 metres and used safely in the pool and bath. Although it is designed for use while children play in the sand and splashing in the sea, the manufacturers do not recommend it be immersed in salt water due to the corrosive effects of the salt. Cochlear’s Freedom & Nucleus 5, and Advanced Bionic’s Harmony speech processors are all described as water resistant but are not suitable for swimming or bathing in. Cochlear have designed the Cochlear Nucleus Aqua accessory, a sealed plastic bag that completely protects the speech processor, cable and transmitter coil for existing wearers of their implants. Children with cochlear implants or hearing aids usually have great difficulty hearing in their swimming classes due to the poor acoustics in swimming pools. The NDCS Me2 deaf-friendly project is working across the UK to help swimming clubs become more deaf friendly. For further information please visit www.ndcs.org.uk/me2. Daily checks of your child’s cochlear implants The following checks should be carried out every day on the external parts of the implant - the speech processor and the transmitter coil. Your child’s implant team will show you how to do these checks on the make and model of cochlear implant your child wears. Your implant team will provide you with a set of replacement leads and coils that you can change at home yourself. When you use your replacement parts don’t forget to let your implant team know so that they can provide you with a new spare. They will probably request you send them the faulty part in return so don’t throw it away unless advised to do so. Switches and controls: Make sure the settings are the same as those given by your cochlear implant centre – if not, reset them if you know how to or take the system back to the centre. Batteries and battery contacts: Make sure you are using the type of battery suggested by your child’s cochlear implant centre. Ensure the batteries are fitted correctly and check the power levels if you have a battery tester. 26 Check that the battery contacts are clean and do not show any signs of rust or rust staining, if so, contact the cochlear implant centre. Leads: Check that there are no obvious signs of wear and tear or damage. Replace the leads if in any doubt. Check the connections between the speech processor and the transmitter coil. If loose contact the cochlear implant centre. Listening check: Your child’s implant team will show you how to do a listening check on the speech processor. If listening earphones are available, make sure you can pick up a signal from the microphone. Some types of listening earphones can also let you judge the quality of the sound. Make sure that you listen at a sound level that is comfortable for you. If you can, make sure that the sound quality is clear and without any crackles. If not, contact your child’s implant centre. The speech processor may have its own self-check function. Make sure that you know about this and what to do if it finds a fault. Checking the telecoil: Ask your child’s implant team to show you how to do this. You may need an extra test device such as a signal check. If you find a problem when doing your daily checks, contact the cochlear implant centre for advice. 27 Assistive Listening Devices Cochlear implants allow most wearers to hear speech well in ideal listening situations. However, most speech is heard in less than ideal listening situations and there are times when your child may find it difficult to hear and listen. Situations when it is difficult to listen are when: there is unwanted background noise, sounds are echoing around the room (reverberation), there is a distance between the person who is speaking and the deaf child. Assistive listening devices (ALDs) can help overcome these problems enabling the wearer to hear people speaking, or sound from other equipment more clearly. Situations where ALDs can be useful for deaf children include when listening to the TV, or using computers, games consuls, MP3 players and smart phones. It is not always possible for children with implants to be able to hear all of these devices with their cochlear implants but for many using an ALD may make it possible for them. Assistive listening devices can connect to cochlear implants in three ways: Telecoil (loop systems), Bluetooth streaming, FM technology. Loop Systems and bluetooth streamers with neck loops Many deaf children use a loop system at home to help them hear the television, music or on the telephone. Advances in technology have enabled deaf children to access a range of products for example, inductive earhooks, neckloops and Bluetooth streamers with neckloops which allow them to share the same experiences as their friends and enable them to listen to mobile phones and use devices such as an iPod, MP3 player, laptop and portable games console. For a more detailed description of available products see the NDCS booklet How Technology can Help. To try out different products to see if they might be helpful contact the NDCS Technology Test Drive by calling the Freephone Helpline on 0808 800 8880 or go to www.ndcs.org.uk/technology. Personal FM Systems (radio aids) An FM system consists of two parts, a transmitter worn by the person talking e.g. a teacher, and a receiver, worn by the child. A microphone picks up the speaker’s 28 voice and the sounds are then transmitted by radio waves to the receiver. The receiver then picks up the radio signal directly from the transmitter. The FM receiver can be connected directly to the cochlear implant by a lead or by direct input with an FM receiver. Deaf children are particularly affected in situations where there is competing noise or where there is an increase in distance between the child and the person speaking. FM systems are widely used by deaf children of all ages and are highly beneficial in a variety of situations, particularly in educational settings where there can be a lot of background noise and reverberation caused by sound bouncing off hard surfaces. FM systems also help in a variety of other situations such as: group activities, in the car – FM systems reduce the problems that exist due to the engine noise and lack of visual clues particularly for children/babies strapped in their car seats, in playgrounds and outdoors, when shopping or on outings. For further information on FM systems read the NDCS booklet How Radio Aids Can Help; or contact the NDCS Freephone Helpline on 0808 800 8880. Customising speech processors Speech processors come in a range of different colours and designs, enabling your child to choose an alternative to the standard beige, brown and grey shades. Ask your child’s audiologist about the range that is available. There are also other options available including decorating and custom covers for your child’s processors. For more information go to www.ndcs.org.uk/family_support/audiology/decorating_and.html. Charges for lost or damaged speech processors The NHS provides speech processors on a permanent loan basis and they always remain the property of the NHS rather than the wearer. NHS equipment should always be returned when it is no longer needed. The current range of speech processors cost between £6,000 and £8,000 each. It is expected that parents and carers will take every reasonable care of their child’s speech processors, and that implant teams will provide retention accessories and advice on their use to ensure that speech processors can be worn securely and without fear of them falling off and being lost. Your implant team will provide guidance on action to be taken should loss or damage occur to one of your child’s speech processors. Insuring speech processors 29 NHS speech processors cannot be insured as they remain the property of the NHS. However, it may be possible to insure against the risk of being charged for their loss or damage. If you do decide to take out insurance, you should shop around for the cheapest all risks policy. The easiest way to insure speech processors is to add them to the all risks section of your household insurance policy, if you have one. You will need to check whether the cost of replacing one processor is more than the maximum allowed for one item. You will also need to check if the equipment is covered by your insurance policy while you are on holiday. If your insurance company will not cover your child’s speech processors, either free of charge or for a small extra fee, you may want to consider changing your household policy to one that meets your needs. When travelling abroad, you may wish to purchase travel insurance to cover the speech processor and external parts of the implant. Most travel insurance does not cover you for pre-existing conditions (including deafness) so it is important to check with your insurer before travel. It might be that you need to use a specialist company that will cover pre-existing conditions. Holiday Loan Holiday loans are provided by each manufacturer in case your own speech processor should develop a fault whilst away. This service has a small cost involved. Should you wish to borrow a speech processor for a holiday contact the company for more information and they will issue you with a form. Once completed, return it to the company and they will get in touch with your implant centre to obtain the mapping information. You will need to ensure that adequate notice is given when applying for a loan. 30 Where to go for more information You can phone the NDCS Freephone Helpline for more information or to speak to our audiology advisor. The National Deaf Children’s Society Castle House, 37 – 45 Paul Street, London EC2A 4LS Freephone Helpline: 0808 800 8880 (voice and text), open between 9.30am and 9.30pm, Monday to Thursday and 9.30 to 5pm on Friday. Fax: 020 7251 5020 Email: [email protected] www.ndcs.org.uk On the NDCS website, you can find Parent Place (www.ndcs.org.uk/applications/ discussion), a message board for parents. Here you can share your own experience to help other families, or search for discussions on any aspect of childhood deafness and view other parents’ questions and answers to each other. British Cochlear Implant Group (BCIG) The BCIG is a professional body that represents all the cochlear implant centres and other specialist medical professionals in the UK. www.bcig.org.uk Cochlear Implanted Children’s Support Group (CICS) This is a support group for parents. It is run by parents whose children have cochlear implants. CICS, PO Box 28843, London SW13 OWY Phone: South: Tricia Kemp: 020 8876 8605 (voice) North: Deborah Faithfull: 01904 744 639 (voice) Midlands: Carmen Burton: 01332 365 528 (voice) Dominic Byrne Tel: 01623 8825 (voice) Email: [email protected] www.cicsgroup.org.uk Cochlear Implants for Teenz website This website has information for teenagers about cochlear implants. It has interviews and comments from teenagers who wear implants, and information about other organisations that might be useful. www.ci-4teenz.com The Ear Foundation This is a charity that bridges the gap between hospital specialists, families, and children and young people who have a cochlear implant. There is a full programme of parent, family and professionals courses, which take place throughout the year. The Ear Foundation, Marjorie Sherman House, 83 Sherwin Road, Lenton, Nottingham NG7 2FB, Phone: 0115 942 1985, www.earfoundation.org.uk 31 Meningitis Research Foundation A charity that supports families whose children have had meningitis or septicaemia. Meningitis Research Foundation, Midland Way, Thornbury, Bristol BS35 2BS 24-hour helpline phone: 080 8800 3344 (voice) www.meningitis.org National Cochlear Implant Users Association (NCIUA) This is a group run by and for cochlear implant users in the United Kingdom www.nciua.org.uk You can also ask your cochlear implant team to put you in touch with families who are going through the assessment process, or whose child has already had an implant fitted. 32 Notes 33 NDCS is the national charity dedicated to creating a world without barriers for deaf children and young people. NDCS Freephone Helpline: 0808 800 8880 (voice and text) Email: [email protected] www.ndcs.org.uk Cochlear Implants – A guide for families was commended in the 2010 British Medical Association Patient Information Awards. Published by the National Deaf Children’s Society Castle House, 37 – 45 Paul Street, London EC2A 4LS © NDCS February 2015 Review due : February 2017 NDCS is a registered charity in England and Wales no. 1016532 and in Scotland no. SC040779 • ISBN 978-1-907814-03-7 Tel: 020 7490 8656 (voice and text) Fax: 020 7251 5020 This publication can be requested in large print, Braille or on audio CD.