Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
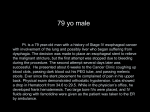
Gullet and Chest Fall/Winter 2014 A Message from the Director Blair A. Jobe, MD, FACS, Director, Esophageal & Thoracic Institute Rodney J. Landreneau, MD, Co-Director of the Esophageal and Lung Institute, Chief of the Division of Thoracic Surgery, and System Director of Thoracic Oncology Welcome to the fall edition of Gullet and Chest. We have had an extremely active summer within the Esophageal and Lung Institute (ELI), and we have several exciting pieces of news to share with you in this edition. However, first and foremost, it is with utmost pleasure that we announce that Rodney J. Landreneau, MD, has been recruited to the Allegheny Health Network family and will serve as the Co-Director of the Esophageal and Lung Institute, Chief of the Division of Thoracic Surgery, and System Director of Thoracic Oncology within the Cancer Institute. Dr. Landreneau comes to us from the Ochsner Health System in New Orleans, where he served as the Medical Director of the Cancer Institute and Vice Chair of the Department of Surgery. He brings to ELI a long and distinguished career of pioneering leadership, excellence and innovation in thoracic surgery. In addition to his unsurpassed clinical talents, Dr. Landreneau is a highly skilled clinical researcher and has led or participated in national clinical trials throughout his career within the American College of Surgeons Oncology Group and the “Alliance” (CAL-GB, NCCTG, ACOSOG) Cancer Cooperative Group. Prior to going to New Orleans, Dr. Landreneau was a tenured professor in the Department of Cardiothoracic Surgery at the University of Pittsburgh, where he worked for more than 20 years. He has been prolific throughout his career and published over 400 peer-reviewed manuscripts in the field of thoracic oncology and esophageal diseases. Dr. Landreneau brings passion, creativity and enthusiasm to everything he does. Within the very near future, we will be opening and enrolling into several additional clinical trials in the field of esophageal and lung cancer, leveraging the AHN’s newborn affiliation with the Johns Hopkins Sidney Kimmel Comprehensive Cancer Center. Dr. Landreneau is highly committed to the people of Pennsylvania and tri-state area, and, although he hails from Baton Rouge, Louisiana, he is a Pittsburgher at heart. The leadership of the Esophageal and Lung Institute believes that it is our absolute obligation to bring every possible advantage to our patients afflicted with esophageal and/or lung cancer. The arrival of Dr. Landreneau bespeaks the commitment and support of AHN to execute this vision. In this issue of G&C, we cover the important issue of Barrett’s esophageal adenocarcinoma. The incidence of this form of esophageal cancer has increased at epidemic proportions over the last three decades and the overall survival — even after aggressive therapy — remains unacceptably low. To put it simply, we must do better. We believe that the answer lies in prevention, early detection and a personalized approach for each patient. The majority of those afflicted are diagnosed at a late stage and this requires a coordinated and multidisciplinary team of experts, which we have assembled within ELI. Our experts are driven toward solutions through research and innovation. This drive is bolstered on a daily basis by the courage and indomitable spirit of our patients. We sincerely appreciate the outpouring of confidence you have shown in our program by entrusting us with your patients. We will continue to deliver humanistic care one patient (family) at a time. In the words of American writer Ursula K. Le Guin, “It is above all by the imagination that we achieve perception and compassion and hope.” ition d E l a i c e p cer S n a C l a e g Esopha Patient Perspective: My Journey with Esophageal Cancer In February 2014, Pittsburgh resident Sara Duffett was told she had esophageal cancer. For the past seven months, Sara has received care at the Esophageal & Lung Institute. Here is her story. Hospital. My ICU nurse was at my bed side whenever she saw that I was in pain. She could see from the window when I was in distress and was at my side before I could press the buzzer for help. Two months ago I danced with my eldest son at his wedding. That doesn’t seem that unusual, except for the fact that I was diagnosed with esophageal cancer in February 2014. It has been quite a journey since February, but it hasn’t been as awful of an experience as one would imagine. I have met the most empathetic and caring people during my surgery, stay in the hospital and throughout my chemo and radiation therapy. Without them, I would have given up hope, but instead I am very optimistic and enjoying my life. Dr. Hiro visited me on the general floors three to four times a day. He made sure everything was going well post-surgery and removed all of my tubes and dressings. While I was taking a walk one day, he joined me and we went to the window to see the sunset. Being treated as a person and not a cancer patient helped immensely in my recovery. I also had a problem at home one day with my feeding tube. I accidently cut the tube off late on a Friday evening. When I called my doctors, they said they were going home for the day. I knew Dr. Hoppo lived in my neighborhood, so I asked if he could meet me somewhere. Instead he said he would come to my house. Yes, my doctor made a house call! I am forever grateful for these compassionate doctors. I will never forget the care that I received while at West Penn Hospital and the doctors that helped me through this process. In November my father passed away and I began experiencing problems with swallowing. I have never been a smoker or drinker and had no acid reflux. The symptom of just having trouble swallowing seemed insignificant to the G.I. doctor that I visited, so I didn’t get an endoscopy until I couldn’t keep food down. The doctor had planned to just stretch my esophagus to allow me to swallow better. Instead, when I awoke from the endoscopy, my doctor told me that I had a cancerous tumor in the wall of my esophagus and needed a surgeon. The third part of my journey was the chemotherapy and radiation treatments. I received five weeks of daily radiation while wearing the chemo pack every day. I did not experience the severe side effects that they expected, but I did lose my appetite and my hair. Losing my hair was not that traumatic, but it did remind me daily that I have cancer. My radiation oncologist, Dr. Russell Fuhrer, gave me some wonderful advice. He said, “Don’t let cancer define you. It is just a bump in the road but it isn’t who you are.” I loved that sentiment and it reminds me to live each day to the fullest. Dr. Casey Moffa and her nurse, Barbara, provided me with superior care as well. They have accommodated me when scheduling appointments and have adjusted my prescriptions to handle the nausea during chemo. They have helped me and made me feel comfortable every step of the way during chemotherapy. Wow, what a blow to my husband and me! I immediately called a doctor friend of mine at the Allegheny Health Network. She referred me to Dr. Blair Jobe at the Esophageal & Lung Institute and said to call him tomorrow. I called him on a Wednesday and he gave me his cell phone number and said that he would see me the following morning. When you hear a diagnosis of cancer, there is nothing more comforting than getting a quick response from your doctors. Dr. Jobe and his practice, including Dr. Yoshihiro Komatsu (Hiro) and Dr. Toshitaka Hoppo, have carried me through this process with compassion and understanding. After another endoscopy with Dr. Jobe, he set my individual plan in motion. He told me we would take this in three steps and not get into all of the problems until we needed to. The first step of my individual plan was to prepare for surgery. I had to see various doctors to evaluate my competency for surgery. I saw a cardiologist (a pulmonary specialist) and was told that I had to recover from the pneumonia I contracted from the preliminary endoscopy. Eventually, all my tests came out great and I was cleared for surgery. I have finally finished all of my chemo treatments and radiation therapy. It has been a hard fought journey. I will receive my PET scan in October and we will find out if all of these treatments have worked. As I stated at the beginning of this article, it has not all been a terrible journey. I am so appreciative of the caring people that I have met along the way. My team of doctors and nurses has been so friendly and competent during these last seven months. I also have a wonderful family, group of neighbors, and the school staff where I work that have been so supportive with meals, cards, rides and their time. I am a very fortunate person and plan to keep fighting. I was always a person that loved life and took time each day to smell the roses and view the sunset. I am remaining positive and enjoying this new life that has taught me to appreciate every moment. The second step of my plan was the surgery to remove my esophagus and, hopefully, the cancerous tumor. The day of my surgery, I asked Dr. Jobe how he was feeling. Ever the jokester, he said he felt great except for the shaking in his hands. I loved his response and felt comfort in his confidence. Everything went very well and I received excellent care in the Intensive Care Unit and on the general floors at West Penn 2 Esophageal Cancer: Disease Burden and Challenges Faced Esophageal cancer is a lethal disease and is the sixth leading cause of cancer deaths in the world. The majority of esophageal cancer patients present with squamous cell carcinoma or esophageal adenocarcinoma (EAC). Since 1970, there has been a 350 percent increase in the incidence of EAC (www.nci.gov), with the preponderance (almost 500 percent increase) in white males over the age of 50. There are approximately 15,000 new esophageal cancer diagnoses per year in the United States, half of which are EAC. In particular, EAC, has risen at an epidemic proportion in the western hemisphere. Chronic gastroesophageal reflux disease (GERD) initiates the development of precancerous cellular changes in the esophageal lining known as Barrett’s esophagus (BE). Approximately, 20 million people suffer from chronic GERD in the United States, of which an estimated 15 percent of cases progress to BE. EAC has known risk factors that include, but are not limited to, being Caucasian, male, over age 50, having reflux disease, obesity, length of BE, hiatal hernia and cigarette smoking. Those diagnosed with BE then undergo lifetime endoscopic surveillance to look for the development of malignancy. Those with dysplasia undergo outpatient endoscopic therapy to reduce the risk of cancer progression. Endoscopic Image of Barrett’s esophagus However, it is important to note that 95 percent of patients who develop EAC have never undergone BE screening prior to their cancer diagnosis. This makes the effectiveness of the current endoscopic screening and surveillance programs very challenging and almost akin to looking for a needle in a haystack. Continued on Page 4. 3 Continued from Page 3. to mask GERD symptoms while the underlying injury mechanism continues unabated. Overall, this results in more than 50 percent of EAC patients presenting initially with difficulty swallowing secondary to obstruction from the tumor representing more advanced disease. Unfortunately, because the esophagus is a distensible organ, the majority of patients who develop EAC do not experience difficulty swallowing until the tumor is advanced and the chances for long-term survival are less likely. Thus, EAC is associated with a poor prognosis, with less than 15 patients out of 100 living more than five years from diagnoses. This underscores the importance of spending research dollars to improve screening and surveillance methods, identifying patients at risk of disease progression and enhancing therapeutic and minimally invasive surgical options for treatment. The Esophageal and Lung Institute offers approaches to diagnosis and therapy not available at other institutions in the region. Compounding the ineffectiveness of the current screening and surveillance paradigm is the fact that up to 57 percent of patients who develop EAC do not even report GERD symptoms and have what is known as “silent reflux.” This “silence” may be compounded by the liberal use of over-the-counter acid suppressant medications that tend You should consider endoscopic screening for BE and EAC if you have: • Commitment to anti-acid medication for more than four years • Difficulty swallowing • Obesity (Body Mass Index >40) with symptoms of reflux • Chronic cough unexplained by any other disease process • A large hiatal hernia • Regurgitation of fluid with changes in body position • Blood in sputum • Heartburn that resolves over time in the absence of treatment with anti-acid medication Endoscopic Image of esophageal cancer 4 Active Clinical Trials Tech Talk n 12-036 Esophageal Tissue Bank n 12-025 POEM Procedure for Achalasia n 13-005 NIH-funded Pathways of Barrett’s n 13-007 Barrett’s Esophagus Risk Consortium n 13-018 Chronic Cough and GERD n 13-035 Lung Tissue Bank n 14-036 B-AMP Panel Serum Study for Esophageal Adenocarcinoma n 3545 Torax Medical Post Approval Study LINX Device n 2271 NinePoint Medical NVLE registry n 2272 Caris Tumor Profiling Registry n Comparative Small Cell Lung Cancer Study n CALGB Lung Cancer Tissue Bank n CALGB 140503 Lobectomy v. Sublobar Resection Unsedated Screening Endoscopy Sedated endoscopy is the primary screening and surveillance method for esophageal disease. It can be quite costly, averaging about $3,000 per exam. Unsedated screening endoscopy, otherwise known as unsedated transnasal or small caliber endoscopy, does not require sedation and can be performed in an in-office setting with a topical anesthetic. This technology has been shown to provide equivalent accuracy in detecting Barrett’s esophagus with excellent patient tolerability. Unsedated transnasal endoscopy is a feasible, safe and well-tolerated method to screen for esophageal disease in a primary care population. Additionally, unsedated endoscopy costs approximately $400 per exam, eliminates anesthesia risks and saves time for patients and their families. Overall, this procedure can enable more people to undergo potentially lifesaving screening at a reduced cost. n Ultrasonography Eval. of Esophageal Cancer n CALGB 80803 PET Scan of Esophageal Cancer n Early Diagnoses of Pulmonary Nodules New Team Members The Esophageal & Lung Institute happily welcomes: n Megan Heit: Clinical Research Coordinator. Megan joins the team with a background in biology and program management as a previous employee of UPMC. n Steve Choe, MD: Minimally Invasive Surgical Fellow. Steve completed his general surgical residency at Drexel University and will be working alongside the institute surgical team during the next year training in minimally invasive esophageal surgery. A Californian, Dr. Choe received degrees from UCLA, Fullerton, and Drexel universities. Our Mission n Amit Shetty BS, MS: Research Fellow. Amit joins the team after completing a master’s degree in physiology from Georgetown University. A Pittsburgh native, Amit received his bachelor’s degree from the University of Notre Dame and previously worked at the University of Pittsburgh Cancer Institute. To provide patient-centered and cutting-edge clinical care for diseases of the esophagus and chest in a compassionate, effective, and user-friendly fashion, employing a coordinated network of clinics which serve the patients of western Pennsylvania, surrounding states and the nation. Gullet and Chest is published by the Esophageal and Lung Institute. Please send all questions and comments to Emily Lloyd, Editor, [email protected] or call 412.578.1343. 5 Expert Care for Esophageal Cancer Clinical scenario: A man in his late fifties with a 15-year history of GERD and a hiatal hernia visits his primary care physician’s office. The patient says he is having problems swallowing and has lost 10 pounds. Furthermore, the patient states that he has been having episodes of regurgitation of foamy saliva and thought that it represented worsening symptoms of GERD. The construct of the Esophageal & Lung Institute is unique in that providers deliver long-term and seamless care throughout the entire course of the treatment and recovery while maintaining detailed communication with the patient’s referring and primary care physicians. Surgeons work closely with medical and radiation oncologists to plan the most effective treatment strategies. Multiple specialists, at one hospital, can see patients on the same day. Molecular profiling is routinely performed on esophageal tumors to best select chemotherapeutic treatment options to target vulnerabilities of a given individual’s cancer. The doctor reviews his medical history and performs a physical examination. The man is referred to an endoscopist where he is scheduled for an upper endoscopy. During the procedure, the physician notices long-segment Barrett’s esophagus with nodularity and a mass in the end of the man’s esophagus. The mass is biopsied and after confirmatory tests, the diagnosis is esophageal adenocarcinoma in a field of Barrett’s esophagus with multifocal high-grade dysplasia. Now what? For those with Barrett’s esophagus or early stage cancer, physicians within the institute are the region’s leaders in endoscopic esophageal preserving techniques, using radiofrequency ablation, cryoablation, endoscopic mucosal resection and endoscopic submucosal dissection (pictured above) to remove cancerous areas from the inside of the esophagus and stomach. These procedures are performed on an outpatient basis and do not require surgical incisions on the skin. The Esophageal & Lung Institute offers the highest quality and most specialized care for individuals diagnosed with esophageal cancer in the region. Individuals receive an initial consultation with one of the institute’s disease-based specialists to outline the best possible treatment plan. Patients are guided through the variety of options currently available to overcome the disease. Patients first undergo clinical staging, which dictates the treatment strategy. Most often, clinical staging can be performed on the same day or within days of the initial consultation. This involves imaging and endoscopic ultrasound of the diseased esophagus and surrounding lymph nodes. For more advanced cases, individuals may need to have the affected area of the esophagus removed entirely. The institute’s surgeons are national leaders in the field of minimally invasive esophagectomy — a combined laparoscopic (abdomen) and thoracoscopic (chest) procedure for removal of the esophagus. This procedure only requires 5 and 10mm incisions that lead to less pain, faster healing times and likely less morbidity than the same procedure performed through large incisions. Continued on Page 7. 6 Continued from Page 6. surgical approach used at the Esophageal & Lung Institute (versus the comparison group), which is theoretically more aggressive in removing all lymph nodes in the region of the cancer. The outcomes of esophagectomy within the Esophageal and Lung Institute are outstanding and compare favorably to that of national and regional numbers. The most recent series of 100 consecutive esophagectomy cases has yielded outcomes consistent or superior to national standards in most postoperative complication categories (see graph below). Of these 100 patients who underwent esophagectomy, 70 underwent the procedure for EAC and had short hospital stays and excellent survival on short term follow-up. The higher pneumonia rates in this series likely reflect the Throughout their treatment and recovery, patients have access to real-time counseling from institute-dedicated dieticians, speech pathologists and palliative care experts who improve an overall sense of well-being. The team works alongside the patient and family throughout the course of their cancer treatment in order to coordinate efforts and provide the best possible outcomes. 7 Case Study: Use of NVLE to target biopsies, increase diagnostic yield and decrease sampling error Upper Endoscopy with Narrow Band Imaging The traditional approach for evaluating a patient with Barrett’s esophagus (BE) is to obtain random biopsies from the field of endoscopically apparent BE. Unfortunately, this approach sets the stage for missing dysplasia and early cancer as only a very small proportion of the field is sampled with very small biopsy forceps. The Esophageal and Lung Institute is the only program in the region that offers optical coherence tomography (volumetric laser endomicroscopy or NVLE) for its patients with BE. This technology enables directed biopsies by using real-time microscopic imaging to pinpoint the location of diseased tissue. Long segment Barrett’s esophagus with the longest lesion measuring 5 cm in length was identified. The surface of the esophageal lining appeared flat and no significant nodularity was identified using the standard white light endoscope and narrow band imaging. NVLE Circumferential images of the esophagus were taken using the volumetric laser endomicroscopy (NVLE). Multiple Barrett’s glands were identified using NVLE at 38.5cm from incisors that were not initially apparent using white light endoscopy. A second area of Barrett’s esophagus was scanned using NVLE but did not show suspicious glands. The Patient The patient is a 51-year-old male with a long history of GERD. He has been on proton pump inhibitors (medication) for over five years which helps his heartburn. He has undergone upper endoscopy by a different physician several times before. His last upper endoscopy was in 2011 which reported long segment Barrett’s esophagus with lesions measuring 8cm in length. Serial biopsies had revealed abnormal tissue (intestinal metaplasia) without dysplasia. We performed upper endoscopy with NVLE to evaluate the current status of his long segment Barrett’s esophagus. EMR and Serial Biopsy Based off of NVLE imaging, endoscopic mucosal resection (EMR) was performed on the suspicious region of Barrett’s esophagus. This EMR sample removed a larger amount of tissue compared to biopsies. Random biopsies were obtained from other areas and all tissue was sent to pathology for analysis. Pathology Outcomes The EMR specimen showed intestinal metaplasia with focal low-grade dysplasia. Random biopsy specimens showed intestinal metaplasia without dysplasia. Future Treatment Plan The NVLE-guided tissue acquisition and the lesions of dysplasia were successfully removed during endoscopy through EMR. Radio frequency ablation (RFA) is planned to remove and treat the remaining Barrett’s tissue. Anti-reflux surgery may also be scheduled in order to eliminate the patient’s GERD and prevent further damage caused by recurrent acid reflux. 8 Genetic profiling in a model of metastatic esophageal cancer: Using research models to gain insight into the mechanisms of metastasis MicroRNAs constitute a recently discovered class of genetic fragments that play a key role in gene regulation. In cancer models they control the “mutated” genes central to tumor development, invasion and spread. By using a molecular profiling technology on rat esophageal cancer specimens, the Esophageal & Lung Institute research team further identified a unique set of microRNAs that predict advanced esophageal adenocarcinoma that will likely spread to other organs within the animal. This unique microRNA signature could eventually be used in clinical care to predict survival, identify patients at risk of developing metastatic disease, and, most importantly, guide selection of molecular targets for new therapies for each individual patient. As an example, this predictive microRNA signature can potentially dictate selection of a more aggressive chemotherapy regimen for patients likely to develop metastasis and save metastasis-unlikely patients from the unnecessary cytotoxic effects where surgery alone will be effective. This work was presented at the Annual Meeting of American College of Surgeons, San Francisco in October, 2014. Over the last decade, advances in molecular profiling technology have resulted in a survival benefit and improved patient quality of life for several well-studied cancer types such as breast, colon and lung. Unfortunately, with EAC, which is an understudied and underfunded cancer, this goal has not yet been realized and is reflected by very low patient survival rates. Therefore, in order to bring benefit to EAC patients there is a profound need to develop representative esophageal cancer animal models to study cancer behavior, cellular changes central to disease progression and to test new drug therapies. Helpful Links for Patients with Esophageal Cancer The animal model employed by researchers at the Esophageal & Lung Institute results in the free flow of stomach acid and bile juices into the esophagus leading to the development of EAC within seven months. This mimics the human esophageal cancer molecular progression. To date, the major criticism of this model has been that, unlike human EAC, no metastatic disease has been shown in these rodents. However, in a recent study, the institute research team was able to confirm distant metastasis in the model using fluorescent labeled metastatic and epithelial markers, hence establishing their esophageal origin. This research finding opens the door to the utilization of this model for the study of mechanisms of EAC metastasis. Esophageal Cancer Action Network - http://www.ecan.org NCCN Guidelines for EAC - http://www.nccn.org/patients/ guidelines/esophageal/index.html#20 Esophageal Cancer Education Foundation - http://www. fightec.org Association of Online Cancer Resources - http://www.acor. org National Cancer Institute - http://www.cancer.gov Esophageal Cancer Awareness Association - http://www. ecaware.org Barrett’s Esophagus - http://digestive.niddk.nih.gov/ ddiseases/pubs/barretts/index.aspx 9 Support for those with Cancer Contact Us To schedule an appointment: Call 724.260.7300 or visit www.ahn.org. The Esophageal & Lung Institute strives to provide the most convenient and reliable cancer support for those immediately affected by the disease. Immediate clinic visits are offered to all patients with a new diagnosis of esophageal cancer where patients and families are supported through the process by trained nurse navigators. To make a donation: Call 412.578.4427 or visit www.wphfoundation.org. For overnight lodging: Family House: for out-of-town patients and their families traveling to any AHN location who require overnight lodging, visit www.familyhouse.org/. For individuals who travel long distances to seek treatment, the Family House offers affordable accommodations and is located in close proximity to West Penn Hospital in Pittsburgh, Pa. Patients and families are provided with housing and shuttle transportation to and from the hospital, as well as many activities. For more information on pricing or to book a room, please call 412.647.7777. For clinical trial enrollment: Call 412.578.1343 Locations Served The Allegheny Health Network offers emotional support and has a variety of resources to help those with cancer and their loved ones through their cancer journey. Support group meetings occur the second Tuesday of every month, from 7:00 to 8:30 p.m. at Jefferson Hospital in Jefferson Hills, Pa. Other meetings will soon be available at West Penn Hospital and the Wexford Health + Wellness Pavillion, located in Wexford, Pa. Registration is easily accessible by calling 412.622.1212. For more information and a comprehensive schedule of other general support groups, please visit https://www.ahn.org/events/. Whether it is finding an affordable and convenient place to stay or learning more about the disease and treatment options, the Esophageal & Lung Institute, as part of the Allegheny Health Network, pledges to provide a supportive environment for those affected by cancer. Allegheny General Hospital 320 East North Avenue Pittsburgh, PA 15212 Peters Township Health + Wellness Pavilion 160 Gallery Drive McMurray, PA 15317 Bethel Park Health + Wellness Pavilion 1000 Higbee Road Bethel Park, PA 15102 Uniontown 97 Delaware Avenue Suite 103 Uniontown, PA 15401 Canonsburg Hospital 100 Medical Boulevard, Canonsburg, PA 15317 West Penn Hospital 4800 Friendship Avenue Pittsburgh, PA 15224 Forbes Hospital 2570 Haymaker Road, Monroeville, PA 15146 Wexford Health + Wellness Pavilion 12311 Perry Highway Wexford, PA 15090 New Castle 3124 Wilmington Road Suite 203 New Castle, PA 16105 10 Meet Your Care Team Lana Y. Schumacher, MD, MS, FACS, is an accomplished thoracic surgeon specializing in thoracic surgical oncology and minimally invasive/robotic thoracic surgery. She is an Assistant Professor of Cardiothoracic Surgery at Temple University and is boardcertified with both the American Board of Thoracic Surgery and the American Board of Surgery. She has a special interest in thoracic oncology and focuses on innovative minimally invasive and robotic approaches to lung and esophageal surgery. Her research interests include specialized treatments for lung and esophageal cancers, lung cancer screening, and participation in national clinical trials. in 1975 and worked there for years. She later became a Senior Professional Nurse and a Certified Gastroenterology Registered Nurse (CGRN). As a nurse educator and preceptor for professional development, Joan has helped to improve knowledge, skills and critical thinking to ensure best practices and positive patient outcomes in the specialty. Ms. Schrenker served as a unit representative to the hospital Professional Practice Council. She participated in the development of a comprehensive orientation and preceptor program for other nursing units regarding the care of patients undergoing GI specialty procedures. Joan also coordinated the development of a nursing staff competency assessment programs that included peer review and self-evaluation processes as well as ongoing continuing education programs and opportunities for nursing career development. Dr. Schumacher received her medical degree at the University of California of Los Angeles (UCLA) School of Medicine and both her Bachelor of Science and Master of Science degrees from the University of Southern California. She completed her surgical internship and residency at Stanford University Hospital and subsequently completed her Cardiothoracic Fellowship at the University of Pittsburgh Medical Center (UPMC). During her surgical training, she also carried out a research fellowship supported by the National Institute of Health in Immunotherapy for Cancer. She further spent fellowship training at the Memorial Sloan Kettering Cancer Center (New York, NY). As the years progressed, Joan found a special niche in diseases of the esophagus. In 2012, Joan joined the Esophageal and Lung Institute under the direction of Dr. Blair Jobe. Currently, Joan coordinates and performs many diagnostic testing such as high resolution esophageal manometry and pH reflux testing as well as related patient/ family education. Results of these procedures assist in the treatment of patients using state-of-the-art critical therapies. With her wealth of knowledge and experience, Joan serves as a resource for staff education for the multidisciplinary team members of the Esophageal and Lung Institute at Allegheny Health Network. Dr. Schumacher is an active member in the Society of Thoracic Surgeons, Women in Thoracic Surgery, General Thoracic Surgery Club and a Fellow of the American College of Surgery. She was awarded the Outstanding Researcher Award at Stanford University in 2008. She has also received numerous teaching awards, the most prestigious being the Arnold P. Gold Foundation Award for Humanism and Excellence in Teaching Award in 2008. Donna Snyder has been employed at the Esophageal and Lung Institute since March of 2013, after having worked for over 20 years in primary care for West Penn Allegheny Health System (now Allegheny Health Network). Donna acts as the institute’s scheduler where she often is tasked with juggling operating room schedules, clinic visits and esophageal testing appointments for the institute’s various sites. In addition to scheduling, Donna seeks out authorizations from insurance providers for surgeries and procedures and is frequently the voice patients hear when calling the institute at 724.260.7300. Donna particularly enjoys the face-to-face interactions with patients and being able to help them receive the care they need. She strives to do her best every day and has learned a great deal while working with the talented surgeons and staff at the Esophageal & Lung Institute. Within Allegheny Health Network, Dr. Schumacher sees patients and performs thoracic surgery at Allegheny General Hospital, West Penn Hospital, Forbes Regional Hospital and Allegheny Valley Hospital. Joan Schrenker RN, CGRN, has practiced nursing for many years in a variety of roles. After graduating from Shadyside Hospital School of Nursing in 1971, Joan worked in the Intensive Care Unit and began learning the specialty of gastroenterology. She was the nurse member of the team that developed the inaugural GI Lab at Shadyside Hospital 11 4800 Friendship Avenue, Suite 242 Pittsburgh, PA 15224 Non-Profit Organization U.S. Postage PAID Pittsburgh, PA Permit No. 2039