Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
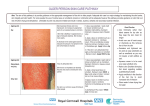
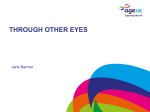
Continuing professional development The use of emollient therapy for ageing skin NOP580 Watkins P (2011) The use of emollient therapy for ageing skin. Nursing Older People. 23, 5, 31-37. Date of acceptance: March 28 2011. Abstract Skin ageing has intrinsic signs and symptoms, often complicated by extrinsic photo-ageing symptoms and concurrent disease processes. It progresses with age but varies between individuals and its symptoms are numerous. Skin ageing has physical and psychosocial repercussions that can influence coping. Emollient therapy can help to reduce two symptoms – dryness and loss of the skin’s barrier function. Better understanding of skin ageing and the usefulness of emollients can be reinforced by education and encouragement from healthcare professionals. Such interventions should encourage self-management and confidence in using emollients. The partnership between healthcare professionals and older people helps to overcome co-existent ageing difficulties, such as cognitive impairment, hearing loss and impairment of manual dexterity and mobility, which enhances self-reliance. Aims and intended learning outcomes The aim of this article is to help develop nurses’ knowledge of the characteristics of skin ageing and their contribution towards deterioration and loss of skin function. It will also help to develop nurses’ knowledge of emollients and emollient therapy, and how this can help to reduce some of the detrimental effects of skin ageing, as well as improve understanding of the role of healthcare professionals in educating older people in emollient therapy and encouraging optimal self-management and self-reliance. After reading this article, you should be able to: ■■ Summarise the characteristics of skin ageing and the associated deterioration and loss of skin function. ■■ Describe the types of emollients and their roles in maintaining the skin barrier. ■■ Discuss the influence of effective emollient therapy in helping to minimise skin ageing and loss of function. ■■ Describe the educational and supportive role of healthcare professionals when helping older patients to cope with the management of ageing skin. Introduction In mid-2008, the most numerous age groups included those born in the post-world war two baby NURSING OLDER PEOPLE boom of 1946/51 and the baby boom of 1966/71. Life expectancy in the UK is expected to rise from 77.8 years to 83.1 years for men and 81.9 years to 86.9 years for women between 2008/09 and 2032/33 (Office for National Statistics 2010). This progressive, dramatic rise in the number of older people helps to frame the importance of skin ageing. More people will live to an older age and many will be concerned with skin function and appearance. The physiological and psychosocial effects of skin ageing on older people have created a demand for better understanding of the process, and particularly for effective interventions (Yaar et al 2002). Patients want to understand how skin ages and how skin appearance and integrity can be preserved for as long as possible. Some skin changes are part of normal ageing, they are intrinsic and genetically related. Others are extrinsic and influenced by the environment. Whatever the source of skin ageing, the concern remains to preserve its integrity by sustaining moisture content and potential as a barrier against infection. Maintaining the suppleness of the skin, reducing cracking and redness also have psychological benefits, making the skin look healthier. Generally, emollient therapy is the primary treatment recommended for skin care (Lawton 2004, Philip Watkins is clinical nurse specialist, dermatology, Epsom and St Helier University Hospitals NHS Trust, Surrey Keywords Emollients, older people, skin ageing These keywords are based on the subject headings from the British Nursing Index. This article has been subject to double-blind review and checked using anti-plagiarism software. For related articles visit our online archive and search using the keywords. June 2011 | Volume 23 | Number 5 31 Continuing professional development National Institute for Health and Clinical Excellence 2007). Emollients are useful to ensure that the skin remains intact and healthy (Aycliffe 2007, Radley and Shaw 2007). However, emollient therapy is poorly acknowledged, leading to under-prescribing (Bridgett et al 1996, Lawton 2004, Clark 2006). With understanding and support, most people can apply emollients simply and regain some independence from healthcare professionals (Cork et al 2003, Cork 2006a, Cork 2006b). Effects of ageing skin 1 Ageing skin Time out Box 1 shows the factors associated with skin ageing. Intrinsic skin ageing is experienced by everyone and primarily affects skin function rather than appearance. However, extrinsic photo-ageing, related to chronic exposure to ultraviolet light, superimposes chronic sun damage on skin affected by intrinsic ageing. Photo-ageing is not universal or inevitable but is likely in people who have been exposed to ultraviolet light through sunbathing or during working hours, for example, roadside workers and farmers. Photo-ageing affects the appearance and structure of the skin. Now do time out 1. Box 1 introduces some of the features associated with ageing that are likely to trigger or exacerbate skin problems. Think about three older people you have nursed. How do they describe their skin now? Are they upset, alarmed or resigned to its appearance and how it has changed? What do they say about how they have looked after their skin? Time-aged skin appears dry, pale, finely wrinkled, lax and marked by a variety of benign lesions. In contrast, the appearance of photo-aged skin depends on skin type and degree of damage. It may look dry, irregularly pigmented and yellow-tinged. It may display deep furrows, severe atrophy, multiple spider-like blood vessels (telangiectasis) on the skin surface and a variety of pre-malignant lesions such as mildly sun-damaged, rough, superficial, pink-red defects (actinic keratoses) (Yaar et al 2002). Ageing progresses cumulatively from unrepaired damage to cells. Deterioration in cell function, with reduced response to lifelong stressors affecting cell growth and multiplication, increases the risk of chronic changes and eventual cell death (Farage et al 2009). In later life, skin cells reproduce at a slower rate to replace surface damage or loss of skin. Sebum 32 June 2011 | Volume 23 | Number 5 production slows, resulting in less natural oil production and drying out of skin surfaces. Elasticity of the skin is compromised by a loosening of the connections between elastin and collagen fibres. Skin becomes flaccid. It thins out and loses fat, leaving it less plump and smooth. Furthermore, gravity pulls at the skin and causes it to sag. Underlying layers of subcutaneous fat cells decrease in thickness, leaving the skin more vulnerable (Finch 2003, Farley et al 2006, American Academy of Dermatology 2011). Epidermal thinning during ageing reduces the effectiveness of the skin as a barrier. The hard keratin-based skin cells (corneocytes) of the outer stratum corneum lose their binding ability. This reduces their capacity for trapping and collecting water, the result of which is further drying of the skin (Lawton 2007). In addition to this, production of Langerhans cells is curtailed, leaving fewer cells to bind with harmful antigens. Older skin then becomes more susceptible to infection, and healing is slower (Ersser et al 2007). During ageing, recovery of the skin’s barrier function after damage is delayed, and the barrier to water loss is more easily disturbed. The time needed to reconstitute competent stratum corneum is more than doubled in older people, partly due to a decreased capacity to synthesise lipids. Age-associated decreases in female hormone levels significantly influence lipid composition in the stratum corneum, suggesting an effect on barrier function in older people (Yaar et al 2002). Additional threats to skin integrity Some older people develop incontinence, exposing their skin to faeces and urine. The skin’s surface becomes softer and waterlogged, and its barrier function is weakened. The groin area is most susceptible to this, and friction from rubbing the damp, warm skin adds to the risk of skin breakdown (Burr 2007). These warm, moist creases or flexures can breed fungal and bacterial communities. Infestations and infections are likely to result if fine cracks appear in the skin. In these situations, the breakdown of the skin barrier is exacerbated (Burr 2007). Itching (pruritus) can have variable origins. Localised itching is usually attributable to skin problems (More 2010). Dry ageing skin can stimulate localised itching, and people naturally respond to this by scratching (Bridgett et al 1996). This can rupture the skin’s surface and disrupt the barrier. Chronic scratching thickens the skin’s surface and further contributes to barrier abnormality, which is seen in conditions such as nodular prurigo and lichen simplex. Emollients can be effective in ameliorating dry skin and associated itching, reducing the risk of scratch damage and ulceration. NURSING OLDER PEOPLE Box 1 Factors associated with skin ageing Lack of fluids ■■ Dehydration. Dryness ■■ Often affects lower legs, elbows and lower arms, rough, scaly skin. Itching ■■ Common in older people because of: – Reduced sebum production (unavoidable). –■Increased central heating in residential homes (avoidable). –■Unnecessarily frequent washing in residential homes (avoidable). –■Pruritus (unavoidable). –■Asteatotic eczema – dry skin (partially avoidable). –■Scratching causing bleeding, ulceration and infection (avoidable). ■■ Increased sensitivity to fabric preservatives, wool, plastics, detergents, bleaches, soaps and other irritants (avoidable). ■■ Prolonged itching may lead to lack of sleep and fatigue (partially avoidable). Bruising (purpura) ■■ Through rubbing and minor trauma (partially avoidable). ■■ Skin thinning and sun damage (partially avoidable). ■■ Loss of fat and connective tissue weakens support around blood vessels, making them more susceptible to injury (unavoidable). Excessive use of soap, antiperspirants, perfumes, hot baths ■■ Increased use of soap increases pH to 7.5, at which point chymotrypsin enzyme activity increases by 50 per cent leading to breakdown of the barrier function of the skin (avoidable). ■■ Can be avoided by reduced use, using warm rather than hot water and frequent use of emollients as an alternative to soap and perfumes. ■■ Increased sensitivity in ageing skin to detergents, bleaches and soaps (unavoidable). Sun exposure, tanning, sun beds, lack of clothing to cover skin and no sun protection ■■ Main cause of skin cancers – actinic keratoses, solar keratoses, basal cell carcinomas, squamous cell carcinomas, malignant melanomas (avoidable). ■■ Sun spots (lentigines) (Figure 1, page 35), skin tags and wrinkles (partially avoidable). ■■ Raised dermal collagen due to scarring from repeated inflammation and sunburn (avoidable). ■■ Elastosis from photo-ageing – thickened yellow bumps and loss of elasticity; thickened dermis loses elasticity and is weaker than normal (avoidable). Smoking ■■ Skin ageing accelerated (avoidable). ■■ Long-term smokers have more facial lines and yellowish sallow complexion (avoidable). ■■ May also increase the chance of skin cancers (avoidable). Stress and frowning ■■ Can lead to wrinkling of skin in the long term (partially avoidable). Skin types and heredity ■■ Fairer skin damages more easily in ultraviolet light (avoidable). ■■ Tendency to wrinkles is inherited (unavoidable). Common skin disorders (actinic keratoses, adult acne, discoid eczema, rosacea, psoriasis, pemphigoid, seborrhoeic dermatitis, seborrhoeic keratoses and varicose/asteatotic eczema) ■■ Become more prevalent with age (unavoidable). ■■ Thickening of dermis (unavoidable). ■■ Loss of elasticity (unavoidable). ■■ General weakening of skin (unavoidable). Outdoor occupation and hobbies – for example, golf, ■■ Exposure to sun and development of skin cancer and photo-ageing. gardening, bowls, sitting in conservatories ■■ May be avoidable or unavoidable depending on opportunities and availability of alternatives. Dry air conditions NURSING OLDER PEOPLE ■■ Dehydration (partially avoidable). ■■ Possibly avoidable indoors but less avoidable outdoors. (Continued over page) June 2011 | Volume 23 | Number 5 33 Continuing professional development Box 1 Factors associated with skin ageing (continued from page 33) Loss of sweat and oil glands ■■ Loss of heat control and natural skin oils. Reduced bone development ■■ Bones shrink away from the skin due to bone loss, which causes sagging skin. Collagen synthesis and degradation ■■ In women, bone mass and skin collagen decline rapidly in the immediate postmenopausal years. Pigmentary changes ■■ Solar lentigo, guttate hypomelanosis and freckles. Blood discrepancies ■■ Telangiectasis, cherry angiomas and senile purpura. However, pruritus can be symptomatic of other problems. If pruritus is universal and not just localised, a blood test may be needed to rule out a systemic or drug-related cause. This should include a full blood count; kidney, thyroid and liver function tests; and in some cases iron concentrations, stool specimens for parasitic origins and chest x-rays for lymphomas (More 2010). Box 2 gives a limited list of alternative causes of pruritus. In my clinical practice I have often been called out to an older patient to review a suspected outbreak of scabies. In many cases, the initial treatment has been prescribed already, but simpler associated problems are likely to prolong the dry reddened skin, such as lack of sufficient fluid intake, being left in clothes contaminated by urine or faeces, being left next to hot radiators or at windows exposed to direct sunlight, and overuse of soap or inappropriate bath products. Cowdell (2009) provides an excellent and detailed account of pruritus and its many causes. Now do time out 2. Box 2 Alternative causes of pruritus Itching with inflammation ■■ Allergic and contact dermatitis. ■■ Drug-induced reaction. ■■ Eczema. ■■ Reaction to insect bite. ■■ Psoriasis. ■■ Seborrhoeic dermatitis. ■■ Infestations – particularly scabies and mites. Itching without inflammation ■■ Brain tumours or abscesses. ■■ Cholestasis or renal failure. ■■ Liver disease, hepatitis C or HIV. ■■ Iron deficiency and polycythaemia. ■■ Thyroid disease. ■■ Phantom itch and post-stroke pruritus. ■■ Drug sensitivity. ■■ Xerosis. (Ward and Bernhard 2005) 34 June 2011 | Volume 23 | Number 5 2 Perceptions of skin care Time out (American Academy of Dermatology 2009, 2011, Cowdell 2009, National Institute on Aging 2010, New Zealand Dermatological Society 2010a) Look through Box 1 again. You have already thought about how older people in your care view their skin and how they have looked after it in Time out 1. Now, what about their perceptions of skin care? Do they believe that exposure to sun is healthy or that soap is good for keeping their skin clean? What do you think about their ideas? Can you think of any alternative ideas you could offer that might tactfully challenge misconceptions? Box 3 offers some suggestions on how to avoid ageing and damage to skin resulting from exposure to ultraviolet light. Emollient therapy Emollients (from the Latin for ‘to smooth and soften’) or moisturisers (adds moisture) are interchangeable terms for topical applications that help to stop hardening and irregularities in the outer horny layer of the skin through the addition of moisture (Ersser et al 2007, New Zealand Dermatological Society 2010b). The essential ingredient of an emollient/moisturiser is lipid, an inclusive term covering fats, waxes and oils. Emollients come in a variety of formulations. Ointments contain a larger percentage of lipid, whereas creams have a mix of lipid and water plus emulsifier to mix the water and lipid. Lotion and gel preparations are also available. Ointment is ideal for dry skin but messy to apply. Creams are less messy and more cosmetically acceptable. Lotions or gels are useful for hairy areas, where entrapment of greasy preparation is unwelcome. The function of emollients can be divided into: ■■ An occlusive covering – they provide a layer of oil on the surface of the skin, trapping water and stopping evaporation, thereby increasing the moisture content of the stratum corneum. NURSING OLDER PEOPLE Box 3 Photo damage and photo-ageing Figure 1 Person with sun spots (lentigines) Wear protective clothing/avoid tanning ■■ A hat with a wide brim can shade the neck, ears, eyes and head. ■■ Wear sunglasses that block 99 to 100 per cent of the sun’s rays. ■■ In the sun, wear loose, lightweight, long-sleeved shirts and long trousers/skirts. (American Academy of Dermatology 2009, 2011, National Institute on Aging 2010, New Zealand Dermatological Society 2010a) ■■ A humectant – they penetrate the stratum corneum, where their low molecular weight and ability to attract water help to draw water from the dermis and retain it in the epidermis; glycerine, urea, lactic acid and glycolic acid are humectants. Some emollients operate as a humectant and occlusive covering (Ersser et al 2007, New Zealand Dermatological Society 2010b). Sometimes, added ingredients can be helpful. Ingredients such as polyvinyl pyrrolidone form a film over the skin’s surface, increasing water retention while blocking access to harmful antigens and irritants (Cork 2006b). Emollients containing agents such as lauromacrogols have anaesthetising properties that help to reduce itchiness (Davies 2007). NURSING OLDER PEOPLE To be effective, emollients should be applied frequently, in suitable quantities (Table 1 and Table 2, on page 36). Formulations should contain the right mix of ingredients to treat the particular area of skin on which they are applied. Emollient formulations include bath additives, soap substitutes, skin cleansers and topical preparations (Watkins 2008). Now do time out 3. 3 Examples of emollients Time out Limit time in the sun ■■ Keep out of the sun between 11.30am and 3.30pm, when the sun’s rays are strongest. ■■ Ultraviolet rays can pass through clouds. ■■ Ultraviolet rays penetrate glass and water in pools, lakes or the sea. ■■ Use sunscreen. ■■ Use a sunscreen with a sun protection factor (SPF) of 15 or higher. ■■ Choose sunscreens with ‘broad spectrum’ on the label. ■■ ‘Water resistant’ sunscreen remains on wet or perspiring skin, but it is not waterproof and it needs replacing at least two hourly. Science Photo Library ■■ Ageing is accelerated in those areas exposed to sunlight (photo-ageing). ■■ Photo-ageing is due to damage caused by ultraviolet radiation, and may cause, for example, lentigines (Figure 1). ■■ Short wavelength ultraviolet radiation (UVB) affects the outside layers of the skin or epidermis. ■■ Longer wavelength ultraviolet radiation (UVA) affects the middle layers or dermis. ■■ Infrared A radiation affects the deeper dermis and subcutaneous tissue. Choose four or five examples of emollients and where you have used them. Are your examples ointments, creams, bath oils, gels or lotions? Read on to see why this matters. The term complete emollient therapy incorporates all of these formulations (Cork 2006a, Waistell 2007). This complete approach relies on combined use of an emollient cream or ointment, emollient bath oil or shower gel, and an emollient soap substitute, and most importantly adequate education on effective application. Complete emollient therapy replaces the need for soap, detergent and bubble baths (Watkins 2008). Ersser et al (2007) argue that emollients are important for promoting skin health in vulnerable June 2011 | Volume 23 | Number 5 35 Continuing professional development Suitable quantities of emollient to be prescribed for specific areas of the body Site Creams and ointments Lotions Face 15–30g 100ml Both hands 25–50g 200ml Scalp 50–100g 200ml Both arms or both legs 100–200g 200ml Trunk 400g 500ml Groin and genitalia 15–25g 100ml Healthcare worker and older patient partnership Healthcare workers who regularly care for older people are most likely to have to introduce emollient therapy and negotiate its use. A discussion between an older patient and the healthcare worker can lead to a decision on which emollient combination will suit that person. Now do time out 5. These amounts are suitable for twice daily application for an adult for one week (British National Formulary 2011) 5 Decisions about care Time out Table 1 In the previous time outs, you considered the beliefs held by older people in your care about their skin’s appearance and management, what makes an emollient, and in which situation each formulation is useful. Now, think about the setting for each of your contacts: is it a hospital or care home with busy schedules? Do you know the patients’ or residents’ work background and what interests they have? Do they have certain limitations to self-directed care, such as partial sight or hearing, restricted mobility and flexibility, compromised thinking and memory retention? 4 Patient choice Time out groups such as older people. Cork (2006a) stresses the importance of patients’ choice of emollients according to cosmetic acceptability. He argues that the best emollient for a person is the one that the user prefers, because the likelihood is that usage will increase. Now do time out 4. Do you work in a hospital or care home setting? Have you seen older patients encouraged to use their own wash and moisturising products? Is a ‘one-product-fits-all’ attitude prevalent? To what extent is the quantity, type and frequency of emollients considered? Table 2 Decisions about care may be viewed as shared contracts between the patient and the healthcare worker. This is known as concordance, and it should have at its core the patient’s informed and educated wishes. The decision is based on a consultation between two people with equally important beliefs about health. However, the most important determinant is the patient’s wishes, not those of the healthcare worker (Marinker 1997, Emollient measures appropriate for an adult for one application Site Light-dose regimen Medium-dose regimen High-dose regimen Arm (x2) 2 pumps, 1 teaspoon 5 pumps, 1 dessert spoon 10 pumps, 1 tablespoon Chest 2 pumps, 1 teaspoon 5 pumps, 1 dessert spoon 10 pumps, 1 tablespoon Abdomen 2 pumps, 1 teaspoon 5 pumps, 1 dessert spoon 10 pumps, 1 tablespoon Upper back 2 pumps, 1 teaspoon 5 pumps, 1 dessert spoon 10 pumps, 1 tablespoon Lower back 2 pumps, 1 teaspoon 5 pumps, 1 dessert spoon 10 pumps, 1 tablespoon Thigh (x2) 2 pumps, 1 teaspoon 5 pumps, 1 dessert spoon 10 pumps, 1 tablespoon Shin (x2) 2 pumps, 1 teaspoon 5 pumps, 1 dessert spoon 10 pumps, 1 tablespoon Total 20 pumps, 20g 50 pumps, 50g 100 pumps, 100g (Adapted from Britton 2003) 36 June 2011 | Volume 23 | Number 5 NURSING OLDER PEOPLE Conclusion Essentially, skin cannot remain as it was during a person’s earlier years. Some of the changes are unavoidable, while others can be reduced by, for example, avoiding drying of the skin and exposure to ultraviolet light. The study of ageing skin is complex and absorbing, but the people occupying ageing skin are even more varied and interesting. Many residents in care homes require considerable help and are dependent on others to perform frequent tasks such as application of emollients. However, many people with ageing skin live full and independent lives, and this group require appropriate management to release their own potential to care for their skin simply and effectively. 6 Practice profile Time out Royal Pharmaceutical Society of Great Britain 1997). Opportunities for healthcare professionals to strengthen concordance arise in simple everyday routines. When assisting patients to bathe, change clothes or shave, the intimacy of tasks can be an opening for talking and sharing ideas and knowledge. Touch during these tasks can improve awareness of dryness of skin or breaks in the skin’s integrity. It can help to expose a need for better skincare practices – for example, by noticing skin odours or inappropriate use of drying products such as soap or powder. Talking to visitors can be a useful way of discovering otherwise forgotten factors such as the home environment – is this damp, cold, unclean or lacking in basic amenities, such as a bath or shower? Now that you have completed the article you might like to write a practice profile. Guidelines to help you are on page 38. References American Academy of Dermatology (2009) Medical Conditions. www.skincarephysicians. com/agingskinnet/skincancer.html (Last accessed: April 21 2011.) American Academy of Dermatology (2011) Mature Skin. www.aad.org/media-resources/ stats-and-facts/prevention-and-care/ mature-skin (Last accessed: April 21 2011.) Aycliffe V (2007) Contact dermatitis and the effect of fragrance allergy. Dermatological Nursing. 6, 3, 10-16. Bridgett C, Norén P, Staughton R (1996) Atopic Skin Disease: A Manual for Practitioners. Wrightson Biomedical Publishing, Petersfield. British National Formulary (2011) British National Formulary No. 61. British Medical Association and the Royal Pharmaceutical Society of Great Britain, London. Britton J (2003) The use of emollients and their correct application. Journal of Community Nursing. 17, 9, 22-25. Burr S (2007) How to assess and manage older people’s skin. Dermatological Nursing. 6, 4, 28-32. Clark C (2006) How drugs work in dermatology. British Journal of Dermatology Nursing. 10, 1, 8-10. Cork M (2006a) The importance of complete emollient therapy. Medicine Matters in Primary Care. 118, July. Lawton S (2004) Effective use of emollients in infants and young people. Nursing Standard. 19, 7, 44-50. Cork M (2006b) Improving the treatment of atopic eczema through an understanding of gene-environment interactions. National Eczema Society Exchange Journal. 121 June, 7-13. Lawton S (2007) Addressing the skin-care needs of the older person. British Journal of Community Nursing. 12, 5, 203-208. Cork M, Carr J, Young S et al (2003) Using emollients for eczema. British Journal of Dermatology Nursing. 7, 2, 6-8. Cowdell F (2009) Care and management of patients with pruritus. Nursing Older People. 21, 7, 35-41. Davies A (2007) Nursing care and management of patients with pruritus. Nursing Standard. 21, 41, 51-57. Ersser S, Maguire S, Nicol N et al (2007) Best Practice in Emollient Therapy: a Statement for Healthcare Professionals. Dermatological Nursing Supplement. Farage M, Miller K, Berardesca E et al (2009) Clinical implications of aging skin: cutaneous disorders in the elderly. American Journal of Clinical Dermatology. 10, 2, 73-86. Farley A, McLafferty E, Hendry C et al (2006) The physiological effects of ageing on the activities of living. Nursing Standard. 20, 45, 46-52. Finch M (2003) Assessment of skin in older people. Nursing Older People. 15, 2, 29-30. NURSING OLDER PEOPLE Marinker M (1997) Personal paper: writing prescriptions is easy. British Medical Journal. 314, 7082, 747-748. More D (2010) Itching: Pruritus. http://allergies. about.com/od/skinallergies/a/pruritus.htm (Last accessed: April 21 2011.) National Institute for Health and Clinical Excellence (2007) Atopic Eczema in Children: Management of Atopic Eczema in Children from Birth up to the Age of 12 Years. Clinical Guideline 57. NICE, London. National Institute on Aging (2010) Skin Care and Aging. www.nia.nih.gov/HealthInformation/ Publications/skin.htm (Last accessed: April 21 2011.) New Zealand Dermatological Society (2010a) Aging Skin. http://dermnetnz.org/ site-age-specific/ageing.html (Last accessed: April 21 2011.) New Zealand Dermatological Society (2010b) Emollients and Moisturisers. www.dermnetnz. org/treatments/emollients.html (Last accessed: April 21 2011.) Office for National Statistics (2010) Population Trends 139. www.statistics. gov.uk/populationtrends/downloads/ Pop-trends-spring10.pdf (Last accessed: April 21 1011.) Radley K, Shaw E (2007) Topical corticosteroids and their use in venous leg ulcers. Dermatological Nursing. 6, 2, 10-15. Royal Pharmaceutical Society of Great Britain (1997) From Compliance to Concordance: Toward Shared Goals in Medicine Taking. RPSGB, London. Waistell C (2007) Applying emollients and topical steroids correctly. Independent Nurse. May, 36-37. Ward J, Bernhard J (2005) Willan’s itch and other causes of pruritus in the elderly. International Journal of Dermatology. 44, 4, 267-273. Watkins P (2008) Using emollients to restore and maintain skin integrity. Nursing Standard. 22, 41, 51-57. Yaar M, Eller M, Gilchrest B (2002) Fifty years of skin aging. Journal of Investigative Dermatology Symposium Proceedings. 7, 1, 51-58. June 2011 | Volume 23 | Number 5 37 Continuing professional development Practice profile What do I do now? ■■ Using the information in section 1 to guide you, write a practice profile of between 750 and 1,000 words – ensuring that you have related it to the article that you have studied. See the examples in section 2. ■■ Write ‘Practice Profile’ at the top of your entry followed by your name, the title of the article, which is: The use of emollient therapy for ageing skin, and the article number, which is NOP580. ■■ Complete all of the requirements of the cut-out form provided and attach it securely to your practice profile. Failure to do so will mean that your practice profile cannot be considered for a certificate. ■■ You are entitled to unlimited free entries. ■■ Using an A4 envelope, send for your free assessment to: Practice Profile, RCN Publishing Company, Freepost PAM 10155, Harrow, Middlesex HA1 3BR by June 2012. Please do not staple your practice profile and cut-out slip – paper-clips are recommended. You can also email practice profiles to practiceprofile@ rcnpublishing.co.uk. You must also provide the same information that is requested on the cut-out form. Type ‘Practice Profile’ in the email subject field to ensure you are sent a response confirming receipt. ■■ You will be informed in writing of your result. A certificate is awarded for successful completion of the practice profile. ■■ Feedback is not provided: a certificate indicates that you have been successful. ■■ Keep a copy of your practice profile and add this to your professional profile – copies are not returned to you. 1. Framework for reflection ■■ Study the checklist (section 3). ■■ What have I learnt from this article? ■■ To what extent were the intended learning outcomes met? ■■ What do I know, or can I do, now, that I did not/could not before reading the article? ■■ What can I apply immediately to my practice or client/patient care? ■■ Is there anything that I did not understand, need to explore or read about further, to clarify my understanding? ■■ What else do I need to do/know to extend my professional development in this area? ■■ What other needs have I identified in relation to my professional development? ■■ How might I achieve the above needs? (It might be helpful to convert these to short/ medium/long-term goals and draw up an action plan.) 2. Examples of practice profile entries ■■ Example 1 After reading a CPD article on ‘Communication skills’, Jenny, a practice nurse, reflects on her own communication skills and re-arranges her clinic room so that she will sit next to her patients when talking to them. She makes a conscious decision to pay attention to her own body language, posture and eye contact, and notices that communication with patients improves. This forms the basis of her practice profile. ■■ Example 2 After reading a CPD article on ‘Wound care’, Amajit, a senior staff nurse on a surgical ward, approached the nurse manager about her concerns about wound infections on the ward. Following an audit which Amajit undertook, a protocol for dressing wounds was established which led to a reduction in wound infections in her ward and across the directorate. Amajit used this experience for her practice profile and is now taking part in a region-wide research project. 3. Portfolio submission Checklist for submitting your practice profile ■■ Have you related your practice profile to the article? ■■ Have you headed your entry with: the title ■■ ‘Practice Profile’; your name; the title of the article; and the article number? ■■ Have you written between 750 and 1,000 words? ■■ Have you kept a copy of the practice profile for your own portfolio? ■■ Have you completed the cut-out form and attached it to your entry? Continuing professional development: practice profile Please complete this form using a ballpoint pen and CAPITAL letters only, then cut out and send it in an envelope no smaller than 23 x 15cm to: Full title and date of article: Job title: Place of work: Address: Practice Profile RCN Publishing Company Freepost PAM 10155 Harrow, Middlesex HA1 3BR 38 June 2011 | Volume 23 | Number 5 Article number: First name: Postcode: Surname: Daytime tel: NURSING OLDER PEOPLE