Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
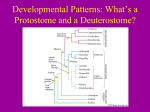
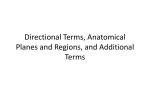
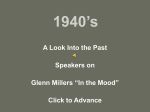
Statistical Analysis of Transmural Laminar Microarchitecture of the Human Left Ventricle Iulia Mirea1, Lihui Wang2, François Varray1, Yue-Min Zhu1, E. E. Dávila Serrano1, Isabelle E. Magnin1 1 Lyon University, CREATIS, CNRS, Inserm, Lyon, France 2 Guizhou University, Guiyang, China. Abstract- A good knowledge of the cardiac microarchitecture is essential for better understanding the function of the human heart. This paper investigates the transmural 3D microstructure of the left ventricle of the human heart. An ex-vivo sample (7 x 7 x 15 mm3) extracted from the anterior wall of the myocardium is imaged using X-rays phase contrast micro-tomography. Sampling the volume at high isotropic resolution of 3.5 x 3.5 x 3.5 μm3 allows a clear reveal of the laminar structure of collagen wrapping the myocytes groups. An image processing protocol is developed to automatically extract cleavage planes and compute statistics of their thickness and distance separating them. The results show the clear presence of cleavage planes in the myocardium and their variation in terms of thickness, interplanes distances and local orientation, which contribute to a better understanding of the human heart function. Keywords— cardiac tissue; 3D; high-resolution; phase contrast imaging; myocytes sheets; cleavage planes; I. INTRODUCTION A good knowledge of the cardiac microarchitecture is essential for understanding the mechanics of the myocardium and of the human heart electrical activity, and the relations between mechanical function, hemodynamics and the adaptive structural changes in cardiac diseases [1, 2]. For this reason, detailed information about the organization and the spatial relationships between the cardiac tissue components is required. However, our understanding of the cardiac architecture is limited by the lack of 3D descriptions of the tissue organization at a small or microscopic scale. One of the main components that define the 3D myocardial tissue organization and function is the cardiac extracellular matrix. The cardiac extracellular matrix includes: endomysium that surrounds and separates individual myocytes and capillaries, perimysium that surrounds and separates groups of myocytes and epimysium that surrounds the entire heart muscle. Previous studies demonstrate that the ventricular myocardium has a laminar organization, where the myocytes are organized in groups separated by cleavage planes “shear layers” [3]. The perimysium, a connective tissue matrix made of collagen, contains the cleavage planes and various components as blood vessels, capillaries, lymphatic vessels. The 3D arrangement of myocardial lamellae accommodates the changing myocytes orientations across the ventricular wall and plays an important role in the mechanical activity of the heart [4, 5, 6, 7]. The description of the transmural architecture has been achieved using 2D techniques such as optical images of histological sections. Such techniques provide high 2D spatial resolutions but suffer from distortions due to cutting thin samples [5]. Although these techniques yield important 2D morphological information, they are not fully adapted to reconstruct complex 3D microstructures that can be resliced and reoriented with much more details. 3D techniques such as polarized light microscopy, transmission or scanning electron microscopy (TEM, SEM) [1, 8, 9] have been used to study the cleavage planes arrangement and their bifurcations. However, those studies were limited to small tissue samples ~ 60 µm. Confocal microscopy can offer a very high 3D resolution, but cannot acquire large image volumes [10, 11]. DT-MRI is also used to image the myocardial architecture non-destructively; however, DT-MRI is limited by a low spatial resolution, comparatively to the myocytes size, to investigate the microstructure [12]. II. HUMAN HEART SAMPLES The human heart sample was supplied by the MedicoLegal Institute of Lyon IML HCL (n◦ DC − 2012 − 1588) and collected during a medical-legal autopsy of a subject who suffered a violent death. A sample (7 x 7 x 15 mm3) located in the anterior wall of the left ventricle was extracted from this heart. The sample preparation procedure and the X-rays phase contrast imaging (PCI) acquisition technique performed at the ESRF are described in [13]. A set of 2500 X-rays projections is acquired and the tissue sample is reconstructed in 3D with an isotropic spatial resolution of 3.5 × 3.5 × 3.5 μm3. The sample has a length of 15 mm corresponding to the thickness of the left ventricle anterior wall from endocardium to epicardium. The width and thickness of the sample are about 5-6 mm. A sub-volume of this sample is shown in Figure 1. The cleavage planes are clearly visible (Figure 1) as planar sections of dark gray color (1). The components of the circulatory system going through the cleavage planes, such as blood vessels are also visible (2). Myocytes lying in the longitudinal section, appear as thin white filaments (3) and in the transversal section (4) as white quasi circular regions. The intercellular space corresponds to thin black filaments (5) in the longitudinal section. cleavage planes because they are the most important structures contained in the binary sub-volume. We threshold the FFT to keep only 4% of the lowest frequency components in order to select the major orientation. We then perform a Principal Component Analysis (PCA) on the coordinates of these pixels as proposed in [14]. This determines the main direction (angles in 3D) of variation that is orthogonal to the cleavage planes. Figure 1. 3D reconstructed sub-volume of the left ventricle anterior sample acquired at the ESRF. In this subsample of size 3 x 1.8 x 0.3 mm3, we can observe that the cardiac tissue components are locally aligned in a principal direction. The cleavage planes appear to be parallel and the myocytes are packaged between the cleavage planes and aligned. The myocytes orientation is restricted by the cleavage planes. The following statistical analysis method is based on the fact that the cleavage planes are locally parallel and have a privileged direction. III. MULTISCALE PROCESSING We analyze the orientation and spatial organization of the cleavage planes for three subsamples of the anterior left ventricle sample: respectively located close to the endocardium, in the mid-wall and close to the epicardium. In order to measure the distances between the cleavage planes, we create a large number of parallel lines crossing the cleavages planes through the 3D sub-volume (Figure 3). Then we analyze the binary profiles along these lines (white = 255 for myocyte sheets and black = 0 for cleavage planes). The sequence length of consecutive 255 values reflects the distance between the cleavage planes and the sequence length of consecutive 0 values gives the thickness of the cleavage planes. The distribution of the length of the two types of sequences, 255 and 0, is obtained, respectively, by computing the two histograms for the entire set of lines. The statistics about cleavages plane distances and size are then extracted from these 2 histograms (Figure 4). The lines are spaced by 3 pixels (10.5 µm). The total number of lines in each subsample is about 110 000. Each 3D reconstructed sub-volume is 7 x 7 x 0.9 mm3 in size corresponding to 2048 voxels x 2048 voxels x 256 voxels. Each sub-volume contains 109 voxels representing 4.3 Gb. Our aim is to extract the cleavage planes structure automatically. To do so, we develop a multiscale approach. First, we build a Gaussian pyramid of each sub-volume. Then, we compute the difference between two levels of the Gaussian pyramid corresponding to σ = 3 and σ = 44 respectively. This allows both to suppress highfrequencies corresponding to noise and slowly varying background while preserving the large structures. We select the size of the Gaussian filter in accordance with the size of myocytes we want to eliminate. The next step is a binarization operation. We apply a 3D Otsu thresholding [15] globally on the preprocessed sub-volume to obtain the cleavage planes. The entire process is illustrated in Figure 2. To investigate the impact of the threshold value on the cleavage planes detection and their quantification properties, we vary the threshold on either side of the obtained threshold. We demonstrate that the evolution of the histogram corresponding to the distance between the cleavage planes remains rather low and that the histogram corresponding to the thickness of the detected cleavage planes remains very similar when the threshold varies around the “Otsu” Value. IV. STATISTICAL ANALYSIS OF THE CLEAVAGE PLANES Once each sub-volume has been binarized, we automatically detect the preferential average direction of the cleavage planes using the following strategy: we take the 3D Fast Fourier Transform (FFT) of a cubic region of interest of each subsample. The Fourier coefficients of highest amplitude correspond to the preponderant spatial orientation contained in the sub-volume. Such an orientation is orthogonal to the Figure 2. Multiscale processing steps used for extracting the cleavage planes The entire process of determining the average orientation, constructing the series of lines and extracting dimensional statistics is illustrated in Figure 2 and Figure 3. corresponding to 185.5 µm. The average distance in the epicardium is about 39 pixels (136.5 µm). Those results are presented in terms of histograms in Figure 5. On the other hand, visually, the orientation of the cleavage planes changes from endocardium to epicardium. Qualitatively, when passing from endocardium to mid-wall, the orientation of the cleavage planes changes by about 90°. Likewise, when passing from mid-wall to epicardium, the cleavage planes orientation also changes by approximately 90°. So, the orientations of the cleavage planes show a range of about 180°. VI. CONCLUSIONS In this paper we have presented a multiscale strategy to automatically extract and analyze some features of the cleavage planes in a fresh human heart sample. The tissue sample was imaged in 3D at a very high isotropic resolution (3.5 µm) using X-rays phase contrast micro CT. We processed three distinct reconstructed sub-volumes of the sample, respectively located close to the endocardium, mid-wall and epicardium. We demonstrate that the proposed method allows to clearly reveal the cleavage planes in the myocardium and quantify some statistical properties such as their thickness, the distances separating them and the evolution of their orientation through the wall. Those are our first results on the left ventricle. New cardiac tissue samples are currently being processed and analyzed. Figure 3. The. red lines are perpendicular to the main orientation of the cleavage planes derived from the PCA of the FFT. V. RESULTS The above-described method is applied on three sub-regions of the sample with equal size of 6 x 6 x 0.9 mm3: a region located at 1.6 mm from the endocardium, a region located at mid-wall (at a distance of 7.5 mm from the endocardium in the middle of the sample) and a region located at 2 mm from the epicardium (i.e. at 13 mm from the endocardium). The cleavage planes are binarized using the method presented above. They correspond to the linear black objects in Figure 2 and Figure 3 also including some blood vessels. At the endocardium, the sample contains trabeculae and papillary muscles. Figure 4 shows three representative sections of the myocardial volume, which correspond to the endocardium, mid-wall and epicardium, respectively. We clearly observe the presence of cleavage planes represented by blue linear objects. They are parallel to each other. In the sub-volume close to the endocardium, the average thickness of the cleavage planes is 10 voxels (35 µm) and the average distance between the planes is 57 voxels (200 µm). They are longer and less fragmented in the mid-wall than at the epicardium. The thicknesses of the cleavage planes in the epicardium and midwall are similar, with an average of about 8 pixels (i.e. 28 µm). In contrast, the distances between consecutive cleavage planes in the mid-wall and the epicardium are slightly different; the distances in the sub-volume close to the epicardium are smaller than in the mid-wall. The average distance in the mid-wall is approximately 53 voxels Figure 5. Statistical study of thicknesses (left column) of cleavage planes and distances (right column) between cleavage planes. The top, middle and bottom rows correspond to the endocardium, midwall and epicardium sub-regions, respectively. ACKNOWLEDGMENTS The authors thank L. Fanton, F. Peyrin, M. Langer, C. Olivier for their help in obtaining the data. This work was done in the scope of the LIA Metislab. REFERENCES [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] Figure 4. Example of three sections of the myocardium X-Rays reconstructed volume corresponding respectively to endocardium, mid-wall and epicardium. The blue regions correspond to the cleavage planes superimposed to the original X-rays reconstructed volume in grey levels. [14] [15] I. J. LeGrice, B. H. Smaill, L. Z. Chai, S. G. Edgar, J. B. Gavin, P. J. Hunter, “Laminar structure of the heart: ventricular myocyte arrangement and connective tissue architecture in the dog”, American Journal of Physiology - Heart and Circulatory Physiology Published 1 August 1995 Vol. 269 no. 2, H571-H582 DOI K. T. Weber, “Cardiac interstitium in health and disease: The fibrillar collagen network”, Journal of the American College of Cardiology June 1989; Vol. 13, Issue 7. pages: 1637-1652. P. F. Ferreira, P. J. Kilner, L.A. McGill, S. Nielles-Vallespin, A. D. Scott, S.Y. Ho, K. P. McCarthy, M. M. Haba, T. F. Isamail, P. D. Gatehouse, R. De Silva, A. R. Lyon, S. K. Prasad, D. N. Firmin, D. J. Pennell, “In vivo cardiovascular magnetic resonance diffusion tensor imaging shows evidence of abnormal myocardial laminar orientations and mobility in hypertrophic cardiomyopathy”, Journal of Cardiovascular Magnetic Resonance 2014, 16:87 H. Ashikaga, J.C. Criscione, J.H. Omens, J.W. Covell, NB Ingels Jr. “Transmural left ventricular mechanics underlying torsional recoil during relaxation.” Am J Physiol Heart Circ Physiol 286: H640 –H647, 2004. K. B. Harrington, F. Rodriguez, A. Cheng, F. Langer, H. Ashikaga, G. T. Daughters, J. C. Criscione, N. B. Ingels, D. C. Miller, “Direct measurement of transmural laminar architecture in the anterolateral wall of the ovine left ventricle: new implications for wall thickening mechanics”, Am J Physiol Heart Circ Physiol 288: H1324 –H1330, 2005. Costa KD, Takayama Y, McCulloch AD, and Covell JW.” Laminar fiber architecture and three-dimensional systolic mechanics in canine ventric- ular myocardium.” Am J Physiol Heart Circ Physiol 276: H595–H607, 1999. T.F. Robinson, L. Cohen-Gould, S.M. Factor “The skeletal framework of mammalian heart muscle. Arrangement of inter- and pericellular connective tissue structures”, Lab Invest 49: 482– 498, 1983 Y. Kanzaki, Y. Yamauchi, M. Okabe, F. Terasaki, N. Ishizaka, “ThreeDimensional architecture of cardiomyocytes and connective tissues in hypertrophic cardiomyopathy.” Images in Cardiovascular Medicine, 2012; 125:738-739. G. Kung, T. C. Nguyen, A. Itoh, S. Skare, N. B. Ingels Jr., D. Craig Miller, D. B. Ennis, “The presence of two local myocardial sheet populations confirmed by diffusion tensor MRI and histological validation”, Journal Magnetic Resonance Imaging, 2011; 34(5):10801091 A. J. Pope, G. B. Sands, B. H. Smail, I. J. LeGrice, “Three-dimensional trasmural organization of the perimysial collagen in the heart,” Am. J. Physiol Heart Circ. Physiol 295, H1243-H1252 (2008) A. A. Young, I.J. LeGrice, M.A. Young, B.H.Smail, “Extended confocal microscopy of myocardiar laminae and collagen network ”, Journal of Microscopy, Vol. 192 , Pt 2, Nivember 1998, pp 139-150 D. Rohmer, A. Sitek, G.T. Gullberg, “Reconstruction and visualization of fiber and laminar structure in the normal human heart from ex vivo diffusion tensor magnetic resonance imaging (DTMRI) data”, Investigative radiology Volume: 42 Issue 11 (2007). I. Mirea, F. Varray, Y.M. Zhu, L. Fanton, M.Langer, P.S. Jouk, G. Michalowicz, Y. Usson, I.E. Magnin, “Very high-resolution imaging of post-mortem human cardiac tissue using x-ray phase contrast tomography ”, In: H. van Assen, P. Bovendeerd, T. Delhaas (EDS), FIMH 2015. LNCS, vol. 9126, pp. 172-179, Springer. F. Varray, L. Wang, L. Fanton, Y-M Zhu, I.E. Magnin, “High resolution extraction of local human cardiac fibre orientation’. In: Ourselin, S. Rueckert, D. Smith, N. (eds.) FIMH 2013,LNCS, vol. 7945, pages. 150157. (2013). N. Otsu, “A threshold selection method from gray-levels histograms”. IEEE Trans. Syst. Man Cybern. 9(1), pages 62-66 (1979)