Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
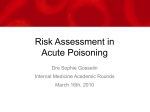
JO_CE_AcutePain_0906_E 8/15/06 3:20 PM Page 1 A FREE CONTINUING EDUCATION LESSON OBJECTIVES Upon successful completion of this lesson, the pharmacist will be able to: 1. assess whether patients require referral to another health-care professional for acute pain management. 2. compare and contrast medications currently indicated for acute pain management. 3. recommend appropriate acute pain management strategies. 4. discuss the role of the newly approved combination tramadol/acetaminophen in the treatment of acute pain. 5. counsel patients about benefits/risks associated with analgesics for the relief of acute pain. INSTRUCTIONS 1. After carefully reading this lesson, study each question and select the one answer you believe to be correct. Circle the appropriate letter on the attached reply card. 2. To pass this lesson, a grade of 70% (14 out of 20) is required. If you pass, your CEU(s) will be recorded with the relevant provincial authority(ies). (Note: some provinces require individual pharmacists to notify them.) ANSWERING OPTIONS A. For immediate results, answer online at www.pharmacygateway.ca. B. Mail or fax the printed answer card to (416) 764-3937. Your reply card will be marked and you will be advised of your results within six to eight weeks in a letter from Rogers Publishing. THIS FREE LESSON IS APPROVED FOR Acute Pain Management — A Practical Update for Community Pharmacists By Tom Smiley, BSc Phm, Pharm D Tom Smiley is a pharmacist consultant and a community pharmacist in Brantford, ON. In addition to his clinical experience with patients and pain management over the last 25 years, Tom has developed and presented many CE lessons and workshops for pharmacists on the topic. He has also written many patient brochures and web postings about acute and chronic pain management principles and integration into practice. Tom currently sits on the executive committee of the Ontario Pharmacists Association board of directors and serves on the Family Health Team Action Group and Chronic Disease Management subcommittee of the Ontario Ministry of Health. The author, expert reviewers and Pharmacy Practice magazine have each declared that there is no real or potential conflict of interest with the sponsor of this lesson. INTRODUCTION It is often difficult to distinguish acute from chronic pain because these phenomena likely represent a continuum rather than distinct entities.1 Acute pain has been defined as “pain of recent onset and probable limited duration.”1 Cause of acute pain is usually associated with an isolated injury or disease process. Pain is an individual experience that is influenced by culture, previous pain events, beliefs, mood and ability to cope. Therefore, pain management strategies must be individualized to the circumstances and personal experiences of the specific patient, and selfreporting of pain should be employed as a monitoring parameter whenever possible.1 It is extremely important that acute pain be treated appropriately and in a timely fashion. In addition to the obvious associated quality-of-life implications, untreated or inadequately treated pain may cause physiologic hormonal responses that alter circulation and tissue metabolism and can produce significant psychological stress responses. 1.25 CE UNITS The body’s immune system may be compromised by release of endogenous corticosteroids provoked by pain.2 Certain acute pain states, including postoperative and post-traumatic pain, acute back pain and acute zoster, may progress to chronic pain if not managed appropriately.1 Pharmacists are frequently the first health professional a patient turns to when seeking relief from acute pain. For this reason, it is extremely important for pharmacists to clearly understand the principles of individualized acute pain management with respect to options available and associated benefits and risks of treatment. This lesson has been designed to refresh and update the community pharmacist’s knowledge in the area of acute pain management. ORIGINS AND TYPES OF PAIN Pain may be nociceptive or neuropathic in nature. Nociceptive pain can be further subdivided into somatic and visceral pain. • Somatic pain is often described as sharp, hot or stinging, and is generally SUPPORTED BY AN EDUCATIONAL GRANT FROM Approved for 1.25 CE units by the Canadian Council on Continuing Education in Pharmacy. File #432-0606. Not valid for CE credits after June 26, 2009. September 2006 | Answer online at www.pharmacygateway.ca Acute Pain Management — A Practical Update for Community Pharmacists | 1 JO_CE_AcutePain_0906_E 8/15/06 3:20 PM localized with surrounding tenderness. • Visceral pain is often described as dull, cramping, or colicky, and is often poorly localized. Visceral pain may be associated with tenderness locally or distally in the form of referred pain, and may illicit symptoms such as nausea, sweating and cardiovascular changes. Neuropathic pain is more common in chronic pain syndromes but may also be a component of acute pain.1 Patients suffering from this type of pain often describe it as burning, shooting or stabbing. The pain may be paroxysmal or spontaneous in nature. Additional experiences associated with neuropathic pain may include:3 • dysaesthesias (spontaneous unpleasant abnormal sensations) • hyperalgesia (increased response to normally painful stimulus) • allodynia (pain due to a stimulus that does not normally evoke pain) • regional autonomic features (changes in colour, temperature and perspiration) • phantom pain. PAIN ASSESSMENT In order to appropriately assess pain, a structured approach should be applied, including identification of the components that contribute to the patient’s perception of pain. A useful tool that may be adapted for such an approach is illustrated in Appendix A. Evidence suggests that regular assessment of pain leads to improved acute pain management.1 The pain assessment tool chosen should be appropriate to the individual patient. Numerical Rating Scales (NRS) or Verbal Rating Scale (VRS) and Visual Analogue Scales (VAS) are the two most common and simple pain assessment tools available (see Appendix B). The NRS has patients assess their pain on a scale of 0 to 10, where 0 represents no pain and 10 represents the worst pain imaginable. The scale can also be used to determine the effectiveness of pain medications where 0 would represent no relief and 10 would represent complete relief.4 The VAS consists of a 100 millimeter (mm) horizontal line with the left side marked no pain and the right side marked the worst pain possible. Various authors have suggested the following interpretation of Numerical Rating Scales (NRS) and VAS ratings:2,5,6 • 7-10 (NRS) or >70 mm (VAS) = severe pain • 4-6 (NRS) or 45-74 mm (VAS) = moderate pain • 1-3 (NRS) or 4-44 mm (VAS) = mild pain 2 Page 2 FIGURE 1: Soft Tissue Injury Acute Pain Assessment Algorithm Soft tissue injury Are any of the following present? • Severe pain • Obvious fracture (bone sticks out or makes grating sound) • Joint deformity • Inability to weight-bear on an injured limb Refer to physician at once How long since injury occurred? <2 days RICE regimen ± oral analgesic 2-14 days NO Has initial swelling subsided? YES When swelling subsides and 48 hours have passed since acute injury, begin therapy listed for 2-14 days Heat therapy. Consider oral or external analgesics >14 days Refer to physician. Consider heat therapy ± analgesics while waiting for appointment. NO Are symptoms resolved in 14 days? Adapted from Reference 9 • 0 (NRS) or 0-3 mm (VAS) = no pain The VAS is unsuitable for children under five years because of the need for concentration and coordination to use effectively.1 Tools such as the Wong-Baker Faces Pain Rating Scale, where children choose faces ranging from happy to sad based on how they are feeling, have been validated for use in children aged 3-8 years (see Appendix B).7 The McGill Pain Questionnaire assesses sensory, affective and evaluative dimensions of pain (see Appendix C).8 This type of tool is more appropriate for pain that is neuropathic in nature and allows the patient to be more descriptive with regard to other factors affecting their quality of life which may also influence their response to pain.1 The tools discussed above and presented in the appendices are easily administered and may be utilized by pharmacists to help assess their patient’s pain and effectiveness of their therapies. GENERAL APPROACH TO ACUTE PAIN CAUSED BY SOFT TISSUE INJURY Pharmacists are often the first point of care for patients who have sustained a soft tissue injury either at home or through sports. A regimen referred to by the acronym RICE is often recommended for initial management | Acute Pain Management — A Practical Update for Community Pharmacists of these types of injuries:9 • Rest – immobilize the affected area for at least the first 24 hours to avoid aggravation of the injury. Continue to exercise unaffected joints where possible to prevent tissue atrophy and loss of coordination. • Ice – Apply cold to injury for reduction of local blood flow. Apply cold therapy every few hours until swelling subsides. Apply for 10-30 minutes at a time depending on body area. Areas with little body fat (e.g., bony areas such as knees, elbows) should be kept to the lower end of time. • Compression – Use an elasticized bandage for at least the first 24 hours to reduce swelling and support a weak joint. • Elevation – Raise the injured area above the level of the heart to help drain fluid and reduce swelling. Figure 1 offers an algorithm for helping patients with acute soft tissue injuries associated with acute pain.9 CONSIDERATIONS IN PHARMACOLOGICAL MANAGEMENT OF ACUTE PAIN Pain is a very individual experience and the selection of pharmacological agents must also be individualized. Factors influencing the choice of medication(s) include: patient’s age, concomitant medical conditions, allergies and sensitivities, patient’s preference for dosage form and dosing Answer online at www.pharmacygateway.ca | September 2006 JO_CE_AcutePain_0906_E FIGURE 2: 8/15/06 3:20 PM Page 3 Pharmacological Choices According to Severity of Acute Pain11 Assess and determine source of pain. Refer to physician for diagnosis where appropriate (e.g., chest pain, migraine, dyspepsia) Minor Pain 1. Acetaminophen 2. If ineffective or not effective for at least 4 hrs, consider NSAID (unless contraindicated) Moderate Pain 1. Codeine ± Acetaminophen* 2. If ineffective or not effective for at least 4 hrs, consider NSAID (unless contraindicated) Severe Pain+ 1. Morphine (unless contraindicated) 2. If ineffective or not effective for at least 2 hours, titrate and consider infusion (or more frequent dosing interval)1 *Tramadol/acetaminophen was not available when this algorithm was originally created and may be considered an alternative to codeine ± acetaminophen (see “Tramadol/Acetaminophen — a new option…”). + It is assumed that most patients with severe acute pain will be treated in hospital. Algorithm refers to patients with somatic pain (most common). Visceral pain and neuropathic pain may require alternative strategies specific to cause of pain and patient symptoms. interval, history of pain management and details of pain. The pharmacist should obtain the following specifics regarding the patient’s pain:10 • Type of pain • Onset and frequency of pain • Description of pain • Location of pain, including radiating patterns • Intensity of pain at rest and with activity • Factors that induce and/or exacerbate pain and associated signs and symptoms • Factors that relieve the pain, including non-pharmacological and pharmacological interventions • Side effects of interventions along with side effect management and their effectiveness • Degree of pain relief or intensity of pain after a pain relieving treatment or intervention Figure 2 suggests an approach to pharmacological management of acute pain. ACUTE PAIN MANAGEMENT IN LIGHT OF RECENT NSAID CONCERNS With the recent withdrawals of the COX2 inhibitors rofecoxib and valdecoxib from the Canadian market and warnings related to the balance of available NSAIDs, acute pain management has become somewhat more complicated. More specifically, evidence from the APPROVe trial indicated that patients treated with rofecoxib had a risk of stroke or myocardial infarction of 1.5 per 100 patient years versus 0.78 per 100 patient years in the placebo group17. Valdecoxib was found in manufacturer studies to be associated with increased risk for cardiovascular events versus placebo and increased risk for potentially serious rash.18 The only clinical trial demonstrating a dose-related increase in serious cardiovascular events with celecoxib compared to placebo (mainly myocardial infarction) employed the drug at a dose of 200 mg twice daily or more (highest recommended dose is 200 mg twice daily for rheumatoid arthritis).15 As a result, celecoxib is currently the only COX-2 inhibitor available in Canada. All NSAIDs, COX-2 or otherwise, are now required by Health Canada to indicate the following statement on their monograph: “Caution should be exercised in prescribing (name of NSAID) to patients with risk factors for cardiovascular disease, cerebrovascular disease or renal disease, such as any of the following (not an exhaustive list):”14 • hypertension • dyslipidemia/hyperlipidemia • diabetes mellitus • congestive heart failure (NYHA 1) • coronary artery disease (atherosclerosis) • peripheral arterial disease • smoking • creatinine clearance <50 mL/min The following strategies have been recommended in light of recent warnings associated with the use of NSAIDs:19 • Use NSAIDs preferentially for patients at low risk of thrombotic events (e.g., no history of ischemic heart disease or stroke; low risk-factor profile for vascular disease). • Initially use drugs with lowest risk of thrombotic events (e.g., acetaminophen); if symptoms are not adequately controlled, assess risk-to-benefit ratio before moving to drugs with a higher risk of thrombotic events (relative degree of COX-2 selectivity cannot be used to assess comparative risks of drugs). • Minimize duration of treatment with NSAIDs to decrease period of risk. September 2006 | Answer online at www.pharmacygateway.ca • Use the lowest dose of NSAID to control symptoms. • If clinical circumstances necessitate NSAIDs be prescribed to patients at increased risk of thrombotic events and/or for extended periods, add ASA 81 mg (enteric-coated) in combination. The antithrombotic effects of low-dose ASA may be helpful but do not necessarily completely neutralize the risks of other NSAIDs. When ASA is used in combination with another NSAID, consider a proton pump inhibitor or misoprostol to reduce risk of gastrointestinal bleeding. • During the period of treatment with an NSAID, the patient should be monitored for increases in blood pressure, development of edema, deterioration of renal function, or development of gastrointestinal bleeding. Where NSAIDs are contraindicated, or risks outweigh benefits, recommendations regarding therapy that will relieve pain to acceptable levels are extremely important. Pharmacists have a critical role to play in helping patients make truly informed decisions regarding pain control. MODERATE TO SEVERE ACUTE PAIN – ASSESSING THE OPTIONS Moderate acute pain is most appropriately treated with a combination opioid/acetaminophen analgesic. One of the most commonly prescribed medications in Canada is acetaminophen with codeine. Codeine is defined as a weak opioid.1 The molecule itself does not have any analgesic activity, but is partially metabolized to morphine (approximately 10% of dose given).1 The enzyme responsible for the conversion to morphine is cytochrome P450 2D6 (CYP2D6). Approximately 9% of Caucasians are lacking in this enzyme and therefore may receive minimal pain relief with codeine and 2% of Asian people due to inefficiency of the CYP2D6 enzyme.1 When it is deemed that severe acute pain is best treated parenterally (due to fast onset of action), the most appropriate choice is intravenous morphine due to less painful administration and more predictable onset of action compared with subcutaneous or intramuscular route. (See Figure 2).11 When possible, pharmacists should refer patients with severe pain to a physician capable of administering this type of treatment (i.e., emergency department or urgent care centre). In circumstances where oral opioids are appropriate, those that are immediaterelease dosage form are the agents of choice for acute pain. All full opioid agonists Acute Pain Management — A Practical Update for Community Pharmacists | 3 JO_CE_AcutePain_0906_E TABLE 1: 8/15/06 3:20 PM Page 4 Overview of Analgesics Recommended for Treatment of Acute Pain in Adults Medication Dose Adverse Effects (ADRs), Precautions & Drug Interactions* Role in Acute Pain Management Acetaminophen Adults: 325-650 mg po or pr q4h Max: 4 g daily Pediatric: 10-15 mg/kg/dose po q4h; 15-20 mg/kg/dose pr q4h Max: 5 doses/day ADRs: Hepatotoxicity11 Pregnancy and Nursing: Analgesic of choice in pregnancy (category B).12 May be used in nursing mothers.13 Drug interactions: Warfarin11 Monitor more frequently at doses of acetaminophen 2000 mg (2 g) daily or above. - Used for mild to moderate pain. - Analgesic and antipyretic activity equal to ASA and fewer adverse reactions and drug interactions than NSAIDs but no anti-inflammatory action. - Use with opioid analgesics for additive analgesic effect.11 NSAIDs Adults (unless otherwise stated) ASA 325 mg - 650 mg po q4h Max: 4 g/day Ibuprofen 200-400 mg po q 6-8 h Max: 1.2 g/day Pediatric: Ibuprofen 10 mg/kg/dose po q 6-8 h Max: 40 mg/kg/day, not to exceed adult dose Naproxen 500 mg initially, then 250 mg po q 6-8 h Max: 1,250 mg/day Celecoxib 400 mg as single dose first day followed by 200 mg /day to a max 7 days. Patients may take up to 400 mg/day as instructed by physician.14 Ketorolac 10 mg PO q 4-6 hrs prn (max 40 mg daily) - not to exceed 5 days for post-surgical patients or 7 days for musculoskeletal pain 10-30 mg IM or IV q 4-6 h Max: 120 mg/day Not to exceed 2 days therapy. Total combined IV/IM plus oral therapy not to exceed 5 days. ADRs: Common (>10%) Dyspepsia, nausea/vomiting, diarrhea, dizziness, headache, antiplatelet effect Uncommon (1-10%) Gastric and duodenal ulcers, fluid retention/ edema, tinnitus, loss of hearing, disorientation, confusion (seniors), increased liver enzymes Rare (<1%) Gastric hemorrhage, perforation, small bowel ulceration, renal insufficiency, skin rashes, hypersensitivity reaction, thrombocytopenia, asthma (in patients with ASA hypersensitivity). Pregnancy and Nursing: Contraindicated during 3rd trimester of pregnancy and while nursing.14 Exception: Ibuprofen is considered compatible with nursing by American Academy of Pediatrics. Category: B (D in 3rd trimester) Drug Interactions: warfarin diuretics, betablockers, ACE inhibitors, alpha-blockers, lithium11 - Indicated for short-term (≤7 days) management of moderate to severe acute pain - COX-2 selective inhibitors (e.g., celecoxib) and nonselective NSAIDs have similar efficacy for acute pain.1 - Usual doses of celecoxib do not appear to have antiplatelet effect but monitoring with warfarin therapy still recommended.14 Opioids Adults (unless otherwise stated) Codeine 15-60 mg q 4-6 h (alone or in combination with acetaminophen) Max: 60 mg/dose Pediatric: Codeine 0.5-1 mg/kg/dose po q 4-6 h Max: 60 mg/dose Morphine (immediate-release) 5-20 mg PO q 4-6 h prn Morphine intermittent iv: 2.5 - 10 mg IM or IV q 2-4 h prn (use lower dosing range for narcotic naïve patients) Morphine (continuous infusion) 1-10 mg/h Breakthrough pain during infusion: 2.5-5 mg/dose Oxycodone immediate-release (alone or in combination with acetaminophen) 5-10 mg PO q6h prn Hydromorphone (immediate release) 2-4 mg PO q 4-6 hrs prn. Meperidine 50-150 mg PO q 3-4 hrs prn 50-100 mg IV q 3-4 hrs prn ADRs: Sedation, constipation, respiratory depression (dose related)1 Pregnancy and Nursing: Category: C (D in prolonged doses) Weigh benefits versus risks for pregnancy and nursing.15 Codeine considered compatible with nursing by American Academy of Pediatrics. Drug Interactions: All opioid CNS depressants Codeine: somatostatin, rifampin, celecoxib, cimetidine, desipramine, fluoxetine, paroxetine, quinidine. - For short-term use in the treatment of acute moderate to severe pain associated with medical conditions such as trauma and myocardial infarction.15 - Oral opioids, preferably shortacting agents at regular intervals may be necessary to relieve severe acute musculoskeletal pain; ongoing need for such treatment requires reassessment.1 Opioid/ serotonin, norepinephrine reuptake inhibitor16 Adults (over 18 years) Tramadol (37.5 mg)/acetaminophen (325 mg) per tablet: 1-2 tablets every 4-6 hours to a maximum of 8 tablets per day. Dose adjustment required for patients with impaired renal function: CrCl <30 ml/min: Max 2 tablets q12h. ADRs: sedation, constipation, respiratory depression (higher dose), increased risk for seizures Pregnancy and Nursing: Risk category C Nursing not recommended as safety not known. Drug Interactions: CNS depressants Carbamazepine (should not be used together) MAOIs (great caution) SSRIs (caution) increased risk of serotonin syndrome, seizures Warfarin - rare interaction - monitor regularly - For the short-term management of acute pain (5 days or less)16. - Tramadol may cause less constipation as compared to codeine at equi-analgesic doses.1 - Tramadol may be useful in neuropathic pain.1 *Please refer to product monographs for more detailed description of drug interactions 4 | Acute Pain Management — A Practical Update for Community Pharmacists Answer online at www.pharmacygateway.ca | September 2006 JO_CE_AcutePain_0906_E 8/15/06 3:20 PM given in equianalgesic doses produce the same analgesic effect.1 Choices include codeine, morphine, hydromorphone and oxycodone. The combination of oxycodone/acetaminophen is also commonly prescribed for moderate to severe pain. Ketorolac is an NSAID that can be given IM or IV or orally. When used parenterally, a dose of 30 mg is comparable in pain relief potential to approximately 12 mg of morphine.11 This treatment is appropriate for pain that would otherwise be treated with parenteral opioids but contraindications exist.11 TRAMADOL/ACETAMINOPHEN – A NEW OPTION FOR ACUTE PAIN MANAGEMENT Recently, a combination product containing tramadol/acetaminophen was introduced on the Canadian market. The following section is intended to help pharmacists understand how this product compares to other currently available acute pain analgesics. Tramadol/acetaminophen (37.5 mg/325 mg) was approved for use in Canada in July 2005 for the short-term management (5 days or less) of acute pain and is marketed under the brand name Tramacet®.20 Unlike other products containing an opioid, Health Canada has designated tramadol/acetaminophen as a Schedule F drug.21 This decision was made based on reports from other jurisdictions, notably the United States, that tramadol abuse occurs at a level of 0.5 - 1.0 case per 100,000 patients who are prescribed the analgesic.22 Furthermore, release of a less expensive generic brand in the United States did not result in an increase in the rate of abuse.22 Although similar studies of the rates of abuse of opiates such as morphine and oxycodone were not undertaken, reports based on prescription drug plan use reveal that therapeutic use of pain relievers seldom leads to dependence.22 Suspicion of patients seeking pain relief remains an inappropriate obstacle to the appropriate use of pain relievers.22 The tramadol component of tramadol/acetaminophen is unique from other opioid agents in that it appears to have at least two complementary mechanisms of action; the binding of parent and a metabolite to µ-opioid receptors and weak inhibition of reuptake of norepinephrine and serotonin.16 When the combination of tramadol/acetaminophen is administered with food, the time to peak plasma concentration is delayed. It is not known whether this delay is clinically significant. Excretion of tramadol is reduced Page 5 in patients with renal impairment and dose adjustments are required for patients with creatinine clearance of less than 30 mL/minute. In these patients tramadol/acetaminophen dosing should not exceed 2 tablets every 12 hours.20 Studies suggest that tramadol has low dependence potential for a period of treatment less than 6 months, but the possibility of dependence with long-term use cannot be ruled out.2 To this end, the manufacturer of tramadol/acetaminophen in Canada has initiated a “risk management strategy” to support the safe and effective use of the analgesic combination product. Appendix A: The components of the risk management strategy include:16 • Commitment to not emphasize or highlight the scheduling of tramadol/acetaminophen in advertising or promotional activities. • Inclusion of an approved fair balance statement in all tramadol/acetaminophen advertising and promotional materials. • Provision of progress reports to Therapeutic Products Directorate, Marketed Health Products Directorate and the Health Environments and Consumer Safety Branch of Health Canada from an ongoing drug abuse surveillance program, Recommended Information to be Assessed During Pain History4 Nature of Pain • Onset and duration • Location(s) and radiation • Quality • Intensity • Associated symptoms • Factors that exacerbate or alleviate pain, including medical intervention Attempted • Ask about current and prior attempts to manage the pain. For prior Management attempts, ascertain why intervention was discontinued. Strategies • Medications (prescription, nonprescription, supplements) • Nonpharmacologic treatments (physical therapy, etc.) • Complementary and alternative treatments (chiropractic, acupuncture) • Other coping strategies (distraction, relaxation) Medical • Prior and coexisting illnesses (including mental comorbidities, substanceHistory abuse disorders) • History of accidents and surgeries • Allergies and/or intolerances to medications • Medical conditions affecting choice of medication Family History • Health status of family members • Family history of pain or illness, including depression Psychosocial • Developmental, marital or vocational problems History • Stressors or depressive symptoms • Compensation/litigation issues Functional Impact of pain on the patient’s: Impact of • Work Pain • Other daily activities (e.g., ability to care for house and family members, ability to participate in sports or hobbies) • Personal relationships • Sleep, appetite, emotions Expectations What the patient hopes to achieve with regard to: and Goals • Intensity of pain • Functional abilities • Quality of life Appendix B: Pain Assessment Tools Numerical Rating Scale Rate your pain on a scale of 0 to 10 where 0 is “no pain” and 10 is “the worst pain ever” Visual Analogue Scale Mark the line below to indicate the current level of your pain NO PAIN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . PAIN AS BAD AS IT CAN BE Wong-Baker FACES Pain Rating Scale* 0 No hurt September 2006 | Answer online at www.pharmacygateway.ca 1 Hurts little bit 2 Hurts little more 3 Hurts even more 4 Hurts whole lot 5 Hurts worst *Adapted from Wong D, Daley L. (1986) Clinical Handbook of Pediatric Nursing, 2nd ed. p. 373; St. Louis. C.V. Mosby Company. Available online at: http://painconsortium.nih.gov/pain_scales/Wong -Baker_Faces.pdf. Acute Pain Management — A Practical Update for Community Pharmacists | 5 JO_CE_AcutePain_0906_E Appendix C: 8/15/06 3:20 PM Page 6 The McGill Short-Form Pain Questionnaire24 Patient’s Name ___________________________________ Date: _______________ None Mild Moderate Severe 1.Throbbing 0) ______ 1) _______ 2) ______ 3) ______ 2.Shooting 0) ______ 1) _______ 2) ______ 3) ______ 3. Stabbing 0) ______ 1) _______ 2) ______ 3) ______ 4. Sharp 0) ______ 1) _______ 2) ______ 3) ______ 5. Cramping 0) ______ 1) _______ 2) ______ 3) ______ 6. Gnawing 0) ______ 1) _______ 2) ______ 3) ______ 7. Hot-Burning 0) ______ 1) _______ 2) ______ 3) ______ 8. Aching 0) ______ 1) _______ 2) ______ 3) ______ 9. Heavy 0) ______ 1) _______ 2) ______ 3) ______ 10. Tender 0) ______ 1) _______ 2) ______ 3) ______ 11. Splitting 0) ______ 1) _______ 2) ______ 3) ______ 12. Tiring-Exhausting 0) ______ 1) _______ 2) ______ 3) ______ 13. Sickening 0) ______ 1) _______ 2) ______ 3) ______ 14. Fearful 0) ______ 1) _______ 2) ______ 3) ______ 15. Punishing-Cruel 0) ______ 1) _______ 2) ______ 3) ______ Total Score = Pain Rating Index (PRI) = ___________ Visual Analogue Scale (VAS) No pain |--------------------------------------------------------------------------------| Worst possible pain Present Pain Index (PPI) 0 No pain ______ 1 Mild ______ 2 Discomforting ______ 3 Distressing ______ 4 Horrible ______ 5 Excruciating ______ Descriptors 1-11 represent the sensory dimension of pain experience and 12-15 represent the affective dimension (qualitative descriptors). Each descriptor is ranked on an intensity scale of 0=none, 1=mild, 2=moderate, 3=severe. The PPI and VAS are included to provide overall pain intensity scores. Appendix D: 1. 2. 3. 4. 5. The Screening Instrument for Substance Abuse Potential25 If you drink alcohol, how many drinks do you have on a typical day? How many drinks do you have in a typical week? Have you used marijuana or hashish in the past year? Have you ever smoked cigarettes? What is your age? The SISAP screening tool suggests to doctors that caution should be used when prescribing opioids for: men who exceed four drinks per day or 16 drinks per week, women who exceed three drinks per day or 12 drinks per week, patients who admit recreational marijuana or hashish use in the past year and patients under 40 who smoke. * For additional addiction screening tools see reference 25 Appendix E: Possible Indicators of Drug-Seeking Behaviour26 • Patient is from out of town • Hurried manner • Allergic to weak opioid analgesics or non-opioid drugs such as NSAIDs • Conversant with clinical terms • Knows street nicknames for prescription drugs • Reluctant to present identification • Offers to pay cash instead of presenting identification or prescription drug plan including data from 4 key informant Canadian sites in the program. • Reassessment of the success of the risk management strategy two years post-product launch. 6 This risk program was modelled after a similar very successful program that was launched in the United States in 1995 along with the release of tramadol in that country.22 Substance abuse and drug diver- | Acute Pain Management — A Practical Update for Community Pharmacists sion are important issues for pharmacists. Appendix E overviews patient characteristics that may indicate drug-seeking behaviour, while the Screening Instrument For Substance Abuse Potential (SISAP) is presented in Appendix D. Although these tools can be used in a general approach to assessing the likelihood of someone seeking drugs, they should not be used to stereotype. Prescriptions from doctors who are not known to the pharmacist should always be verified regardless of the circumstances. The risk of respiratory depression with tramadol is significantly lower at equianalgesic doses in comparison with other opioids.1 Tramadol is also associated with less constipation and has less effect on gastric emptying and postoperative bowel recovery than morphine. Nausea and vomiting occur at rates that are similar to other opioids. Tramadol may increase incidence of seizures with increasing risk at higher doses (above recommended range) and when used together with selective serotonin re-uptake inhibitors, tricyclic antidpressants, other opioids, monoamine oxidase inhibitors, neuroleptics or other drugs that reduce the seizure threshold.1,16 Two studies comparing tramadol/acetaminophen to other currently available agents have been conducted. Tramadol/ acetaminophen has been found to work as well as acetaminophen with codeine 30 mg for chronic back pain and osteoarthritis pain.2 Tramadol 37.5 mg/acetaminophen 325 mg was recently compared to codeine 30 mg/acetaminophen 300 mg or placebo (2 tablets initially, then 1 to 2 tablets every 4 to 6 hours as needed) in 305 patients with postsurgical orthopedic or abdominal pain.20 Tramadol/acetaminophen was superior to placebo for average daily pain relief and average daily pain intensity while codeine/acetaminophen was found to be not statistically different in these categories from placebo. Tramadol/acetaminophen was found to be superior to placebo but was not significantly different than acetaminophen/codeine for total pain relief, sum of pain intensity differences, and sum of pain relief and pain intensity differences. Adverse events were similar for both treatment groups except for constipation (4.1% for tramadol/acetaminophen versus 10.1% for codeine/acetaminophen) and vomiting (9.2% for tramadol/acetaminophen and 14.7% for codeine/acetaminophen).20 In a study comparing tramadol 37.5 mg/acetaminophen 325 mg tablets with hydrocodone bitartrate 10 mg/acetaminophen 650 mg tablets for treatment of postoperative dental pain, the tramadol/acetaminophen combination (2 tablets) was Answer online at www.pharmacygateway.ca | September 2006 JO_CE_AcutePain_0906_E 8/15/06 3:20 PM found to provide equivalent analgesia to the comparator (one tablet) with a better tolerability profile.23 Tramadol/acetaminophen offers an alternative to codeine/acetaminophen for treatment of moderate acute pain in those who find codeine ineffective or who cannot tolerate constipation associated with codeine. THE PHARMACIST’S ROLE IN ACUTE PAIN MANAGEMENT Pharmacists are often the first health professional consulted by patients with acute pain. It is extremely important for health professionals to gather appropriate information and make individualized recommendations regarding the best therapeutic approach. Open communication with the patient is a vital component in the approach to effective pain management. Assessment of pain type, level, duration and compounding factors are critical for identifying those patients in need of emergency or physician care. Assessment tools presented in the appendices will help with patient assessment. Rest, application of cold, compression and elevation of injured limb are often appropriate recommendations for self-limiting soft tissue injuries that have occurred within the last 48 hours. Recommendation of appropriate analgesia (based on benefitto-risk considerations), and ongoing care as outlined in Figure 1 are also important roles for the pharmacist. Pain control is a patient’s right, and it is tremendously important for pharmacists Page 7 to help their patients make educated and well-informed decisions. For example, some patients may fear taking opioids due to addiction concerns, or NSAIDs because of the recent reports of cardiovascular events associated with their use. Pharmacists need to take individual patient concerns into account when recommending the most appropriate therapy for managing pain effectively. 11. Bailey B. Acute Pain. In: Gray J, editor. Therapeutic Choices. Ottawa: Canadian Pharmacists Association, 2003: 116-27. 12. Black RA, Hill DA. Over-the-counter medications in pregnancy. Am Fam Physician 2003; 67(12):2517-24. 13. Medline Plus. Acetaminophen (Systemic). Available online at http://www nlm nih gov/medlineplus/druginfo/uspdi/202001 html. Accessed March 23, 2006. 14. Celebrex product monograph. Pfizer Canada 2006. 15. Opioids Product Monograph. Compendium of Pharmaceuticals and Specialties 2006. 16. Tramacet Product Monograph. Janssen-Ortho Inc 2006. 17. Bresalier RS, Sandler RS, Quan H, Bolognese JA, Oxenius B, Horgan K et al. Cardiovascular events associated with rofecoxib in a colorectal ade- REFERENCES noma chemoprevention trial. N Engl J Med 2005; 352(11):1092-102. 1. Australian and New Zealand College of Anaesthetists and 18. Health Canada. Bextra: Important Safety information. Faculty of Pain Medicine. Acute Pain Management: Scientific Evidence. Available online at http://www.pfizer.ca/english/newsroom/press% Available online at http://www anzca edu au/publications/acutepain 20releases/default.asp?s=1&year=2004&releaseID=146.2006. pdf. Accessed March 21, 2006. Accessed March 21, 2006. 2. Reisner LKPJS. Pain and its Management. In: Koda-Kimble M, Young L, Kradjan WA, et al, editors. Applied Therapeutics: The Clinical Use of Drugs. Philadelphia: Lippincott, Williams & Wilkins, 2005: 9.1-9.40. 3. Hobbs GJ, Hodgkinson V. Assessment, measurement, history and examination. In: Rowbotham D, Macintyre PE, editors. Clinical Pain Management; Acute Pain. London: Arnold Publishers, 2003. 4. American Pharmacists Association. A Pharmacist’s Guide to the Clinical Assessment and Management of Pain. Available online at http://www pharmacist com/pdf/pain/pharmacists-guide pdf 2004. 19. Antman EM, DeMets D, Loscalzo J. Cyclooxygenase inhibition and cardiovascular risk. Circulation 2005; 112(5):759-70. 20. PMPRB Canada. Report on New Patented Drugs - Tramacet. Available online at http://www.pmprb-cepmb.gc.ca/English/View asp?x=561&mp=117. Accessed March 23, 2006. 21. Health Canada. Notice of Decision for Tramacet. Available online at http://www.hc-sc.gc.ca/dhp-mps/prodpharma/activit/ proj/sbd-smd/nd_ad_2005_tramacet_095167 _e html. Accessed March 26, 2006. Accessed March 21, 2006:1-39. 5. Aubrun F, Langeron O, Quesnel C, Coriat P, Riou B. Relationships between measurement of pain using visual analog score and morphine requirements during postoperative intravenous morphine titration. Anesthesiology 2003; 98(6):1415-21. 22. Cicero TJ, Inciardi JA, Adams EH, Geller A, Senay EC, Woody GE et al. Rates of abuse of tramadol remain unchanged with the introduction of new branded and generic products: Results of an abuse monitoring system, 1994-2004. Pharmacoepidemiol Drug Saf 2005; 14(12):851-9. 6. Jensen MP, Chen C, Brugger AM. Interpretation of visual analog 23. Fricke JR, Jr., Karim R, Jordan D, Rosenthal N. A double-blind, scale ratings and change scores: A reanalysis of two clinical trials of single-dose comparison of the analgesic efficacy of tramadol/acetamin- postoperative pain. J Pain 2003; 4(7):407-14. ophen combination tablets, hydrocodone/acetaminophen combination 7. Wong DL, Baker CM. Pain in children: Comparison of assessment scales. Pediatr Nurs 1988; 14(1):9-17. 8. Melzack R. The McGill Pain Questionnaire: Major properties and scoring methods. Pain 1975; 1(3):277-99. 9. Lum L. Sports Injuries. In: Repchinsky C, editor. Patient SelfCare. Ottawa: Canadian Pharmacists Association, 2002: 439-46. 10. The Canadian Pain Society. Accreditation Pain Standard: Making it Happen! Available online at http://www.canadianpainsociety.ca/ accreditation_manual.pdf. Accessed March 21, 2006. tablets, and placebo after oral surgery. Clin Ther 2002; 24(6):953-68. 24. Melzack R. The short-form McGill Pain Questionnaire. Pain 1987; 30(2):191-7. 25. The Canadian Pain Society Task Force. Use of opioid analgesics for the treatment of chronic noncancer pain - A consensus statement and guidelines from the Canadian Pain Society. Pain and Research Management 1998;1-19. 26. Goldman B. Drug-Seeking Behaviour. Managing Pain - The Canadian Health Professional’s Reference 2002;77-86. QUESTIONS 1. Which of the following best describes the type of pain that John is experiencing? a) Neuropathic c) Somatic b) Visceral d) Allodynia 3. Which recommendation(s) would be most appropriate for John? a) Immobilize and rest the ankle for at least 24 hours and apply cold therapy every few hours until swelling subsides. b) Try walking on the injured ankle every few hours for the first 24 hours to prevent tissue atrophy and apply ice after each round of exercise. c) Sit with the heel on the floor and keep the ankle joint flexed. d) a and c 2. You ask John what his pain is on a scale of 0 to 10 where 0 is no pain and 10 is the worst pain imaginable. He says it is about a 6. Which of the following would best describe the level of his pain according to the Numerical Rating Scale? a) Mild pain c) Severe pain b) Moderate pain d) Very severe pain 4. Which situation(s) should prompt a referral to a physician as soon as possible? a) Severe pain b) Obvious fracture c) Inability to bear weight on the injured ankle. d) All of the above CASE 1: John H is a 20-year-old male who has just twisted his ankle while playing intramural basketball at university. He has come into the pharmacy and describes his pain as sharp and stinging, with tenderness around the ankle. He is not currently taking any medication and is generally healthy. September 2006 | Answer online at www.pharmacygateway.ca 5. If John’s physician prescribed celecoxib for him, which protocol would be most appropriate for acute pain management? a) 100 mg bid for maximum 14 days b) 200 mg bid for maximum 7 days c) 400 mg first day, followed by 200 mg daily for 7 days maximum d) 400 mg once daily for maximum 7 days CASE 2: Sonya is an otherwise healthy 4year-old who has just had a tonsillectomy. She weighs 22 kg. The physician has recommended ibuprofen for pain. 6. Which dose of ibuprofen would be most appropriate for Sonya? a) 200 mg every 6-8 hours prn b) 100 mg every 4 hours prn c) 50 mg every 4 hours prn d) 100 mg every 6-8 hours prn Acute Pain Management — A Practical Update for Community Pharmacists | 7 JO_CE_AcutePain_0906_E 8/15/06 3:20 PM Page 8 QUESTIONS continued 7. If the doctor had prescribed acetaminophen suppositories, which statement would apply? a) Give double dose as recommended for oral acetaminophen products in the suppository dosage form. b) She should receive 325 mg pr q4h with a maximum of 5 doses per day. c) She should receive 480 mg pr per day divided into 4 doses (i.e., 120 mg qid prn). d) She should receive 650 mg pr q6h with a maximum of 4 doses daily. CASE 3: Joan is a 30-year-old female who has been given a prescription for acetaminophen 300 mg with codeine 15 mg, 1-2 tablets q4h prn pain for one week. Additional medications include docusate sodium 100 mg at bedtime. She is currently nursing her infant baby. 8. Which statement about codeine is TRUE? a) About 9% of the Caucasian population lacks the enzyme to metabolize codeine to morphine. b) Codeine is not compatible with breast feeding according to the American Academy of Pediatrics c) Acetaminophen with codeine is a primary choice for minor pain. d) None of the above. 9. Would celecoxib be considered an appropriate alternative for Joan? a) Yes, if acetaminophen with codeine is ineffective. b) Yes, NSAIDs should actually be used before acetaminophen with codeine for moderate acute pain. c) No, because Joan is nursing. d) No, because Joan is taking docusate sodium. CASE 4: Fred is a 58-year-old man with Type 2 diabetes. Fred currently takes metformin 500 mg bid, ramipril 10 mg once daily, and coated ASA 81 mg daily. He has a prescription from his doctor for diclofenac 25 mg three times daily for acute pain. 10. Which statement(s) about NSAIDs is/are TRUE? a) COX-2 selective inhibitors are considered by Health Canada to be associated with greater cardiovascular risk than traditional NSAIDs. b) Patients who smoke are at increased risk of cardiovascular events while using NSAIDs than the general population. c) Valdecoxib has been associated with increased risk for serious rash. d) b and c 8 11. Which statement(s) about Fred’s circumstances is/are TRUE? a) Fred should stop taking his coated ASA while taking diclofenac. b) Fred does not have any risk factors that increase his risk for cardiovascular adverse effects with NSAIDs. c) Fred should continue to take his coated ASA while taking diclofenac as its antithrombotic effect may be helpful. d) None of the above. CASE 5: Millie is a 48-year-old woman who has just had dental surgery. She rates pain at 6 out of 10 on the numerical rating scale. The doctor calls and says Millie can’t take NSAIDs, and codeine tends to constipate her. You ask if he has considered Tramacet® (tramadol/acetaminophen). 12. Which of the following are included in the indications for use of tramadol/ acetaminophen for acute pain? a) Use for not longer than 5 days. b) Use for not longer than 7 days. c) Use for not longer than 14 days. d) Use for not longer than one month. 13. Which of the following is TRUE of tramadol/acetaminophen compared with acetaminophen/codeine? a) Less constipation at equi-analgesic doses. b) Increased risk for respiratory depression at equi-analgesic doses. c) Increased risk for interaction with CYP2D6 inhibitors. d) a and c 14. Which drugs should not be used with tramadol/acetaminophen but may be used with other opioids? a) Amlodipine b) Verapamil c) Carbamazepine d) Clonazepam 15. If Millie has a creatinine clearance of 25 mL/min, what is the maximum daily dose of tramadol/acetaminophen (37.5/325 mg) tablets allowed? a) 2 c) 6 b) 4 d) 8 16. Which description makes tramadol/acetaminophen unique among opioid analgesics? a) It is associated with a very low abuse potential. b) It is a Schedule F product. c) The manufacturer has implemented a post-marketing “risk management strategy.” d) All of the above | Acute Pain Management — A Practical Update for Community Pharmacists 17. Which result was found in a study comparing 2 tablets tramadol/acetaminophen (37.5/325 mg) with hydrocodone bitrartrate/acetaminophen (10/650 mg) for treatment of postoperative dental pain? a) Tramadol/acetaminophen provided better analgesia with better tolerability. b) Tramadol/acetaminophen provided less analgesia with better tolerability. c) Tramadol/acetaminophen provided equivalent analgesia with better tolerability. d) Tramadol/acetaminophen provided better analgesia with worse tolerability. 18. Which situation would lead you to suspect drug-seeking behaviour or someone at high risk for substance abuse? a) A man hands you the prescription, says immediately that he will pay cash and that he is in a bit of a hurry. b) When asked, a 58-year-old woman tells you she smokes one-half pack of cigarettes a day. c) A 40-year-old man tells you he has a glass of wine with dinner every day. d) All of the above would lead you to suspect drug-seeking behaviour or substance abuse potential. 19. Which patient would be most appropriate to ask to fill out a short-form McGill Pain Questionnaire? a) A patient who complains of pain symptoms that are burning, shooting and stabbing in nature. b) A patient whose pain is generally welllocalized. c) A patient who marks their pain at 10 mm on a standard Visual Analogue Scale. d) None of the above 20. Which statement is TRUE concerning acetaminophen and warfarin use? a) Acetaminophen and warfarin do not interact. b) Acetaminophen may increase the effects of warfarin at a dose of approximately 650 mg daily in most individuals. c) Acetaminophen may increase the effects of warfarin at a dose of approximately 2 g daily in most individuals. d) One should begin monitoring INR more closely when acetaminophen doses reach 4 g daily. Answer online at www.pharmacygateway.ca | September 2006 TO ANSWER THIS CE LESSON ONLINE If currently logged into our ONLINE CE PROGRAM, please return to the "Lessons Available Online" Page and click on "Link to questions" for this CE Lesson. If not logged in but already registered to our ONLINE CE PROGRAM, please click here: http://ce.pharmacygateway.com/Pharmacy/login/index.asp If you have not registered for our ONLINE CE PROGRAM and wish to answer online, please click here: http://ce.pharmacygateway.com/Pharmacy/login/adduser.asp If you have any questions. Please contact: Pharmacy Practice, Pharmacy Post, Novopharm CE Compliance Centre, More CCCEP-approved CE’s, or Tech Talk (English and French CE's) Mayra Ramos Fax: (416) 764-3937 or email: [email protected] Quebec Pharmacie and L'actualite Pharmaceutique Stephane Paradis Fax: (514) 843-2183 email: [email protected]