Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
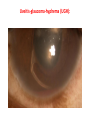
Postoperative uveitis Ahmad Jahanbakhshi, MD TASS Chronic Endophthalm itis Preexisiting Uveitis Diabetic patients UGH • TASS: acute inflammatory reaction ,noninfectious substance enters AC ,toxic damage to intraocular tissues, within 12-48 h after uncomplicated surgery,mimics infectious endophthalmitis. 1.Minimal or no pain 2- pronounced cellular and fibrinous AC reaction 3.diffuse limbus-to-limbus corneal edema without posterior segment involvement. Clinical feature It usually improves with local steroid but may result in chronic elevation of IOP or irreversible corneal edema (J Fr Ophtalmol. 2015 ) AC inflammation is severe with hypopyon, No bacterium in ocular samples. Initialy infectious and noninfectious inflammation indistinguishable ,TASS is usually diagnosed and treated as acute endophthalmitis. Etiology:For a few of these outbreaks, the inciting factors were identified, but for the majority, the precipitating factors were often postulated but not confirmed. anesthetics and antibiotics i Incorrectly BSS, pH,or osmolarity • Bacterial endotoxin preservatives, • hand gloves, • IOL,medicati ons/solutions, • Denatured OVD Viscoelastic substance( Ivisc®1.4% sodium hyaluronate(Cutan Ocul Toxicol. 2015 Outbreak of Late-Onset Toxic Anterior Segment Syndrome After Implantation of One-Piece IOL. (Am J Ophthalmol. 2015 Jul) Two cases of toxic anterior segment syndrome from generic trypan blue(J Cataract Refract Surg. 2015 ) Some cases of TASS associated with spillover of subconj gentamicin at the end of routine cataract surgery have been reported It is important to recognize that contamination of OVDs with endotoxins can occur at the time of manufacturing. Therefore, i.e. <0.5 endotoxin units/ml must be considered during OVD manufacture. • 6 case,fulminant onset,first 24 h of surgery,high IOP, corneal edema similar to TASS,corneal infiltrates, scleral and uveal necrosis ,hyphema, brownish exudates in AC,necrotizing retinitis in despite immediate intravitreal AB and vitrectomy.gram-positive bacilli in aqueous.2 eyes required therapeutic keratoplasty,with a scleral patch graft in 1 eye, 1 eye was eviscerated after 48, and 2 eyes had phthisical changes within 10 days . One must closely observe every case of TASS that presents with intense pain and extremely high IOP and rule out APE owing to B cereus with microbiologic testing.(Ophthalmology. 2015 ) final coarse of TASS: resolution of severe iridocyclitis was 4 to 8 days 24% atrophic iris changes, 4% CME, 12.5% anterior capsule phimosis 16% PCO. >> There was no significant difference between the mean BCVA at 1 month and 6 months. TASS responded to intensive topical anti inflammatory medication, and was usually associated with a good visual outcome. (J Cataract Refract Surg. 2016) Uveitis Mean relapse-free time was similar (131150 days group A (topical steroid) group B (topical + oral steroid) Perioperative prophylaxis to prevent recurrence following cataract surgery in uveitic patients (Acta Ophthalmol. 2016 Feb ) Uveitis and IVTA BCVA improvement >2 lines in 86.7%. BCVA >1/10 in 73% (4 mg) 17% BCVA= 5/10 Intraoperative intravitreal triamcinolone acetonide for cataract extraction in patients with uveitis controlled postoperative inflammation in all eyes at least 3 months following surgery. (Ocul Immunol Inflamm. 2015) significant reduction in inflammation recurrences 6 m before and 6 m after surgery with Ozurdex Uveitis and Ozurdex (Dexamethasone Intravitreal Implant) IOP remained stable Ozurdex safely and effectively controlled postoperative inflammation in eyes with chronic recurrent uveitis during anterior segment surgery . Caution :Ozurdex use is now contraindicated in posterior capsule rupture and ACIOLs. (J Ocul Pharmacol 2015) Diabetic patients The ratio of fibrinous uveitis, PS, and PCO was found higher in the diabetic group • Diabetic patients should be monitored more carefully for fibrinous uveitis and PS in the early postoperative period and for PCO in late postoperative period Anterior segment complications after phacovitrectomy in diabetic and nondiabetic patients. (Eur J Ophthalmol. 2013 ) Low grade chronic endophthalmitis caused by P.acnes Ophthalmologe. 2015 -Chronic indolent inflammation, misdiagnosed as noninfectious uveitis. This form of endophthalmitis is often unsuccessfully treated with corticosteroids. -It caused by Propionibacterium acnes . -It is difficulties in establishing diagnosis of this form of endophthalmitis as well as the benefits of pars plana vitrectomy, intravitreal antibiotics and posterior capsulectomy for successful treatment in such cases. Massilia timonae as cause of chronic endophthalmitis following cataract surgery. J Cataract Refract Surg.2015 Uveitis-glaucoma-hyphema (UGH): UGH: 1.ACIOL 2.Malpositioned PCIOL 3.In-the-bag placement of intraocular lens. BMJ Case Rep. 2016 -A 48-year-old man with blurred vision after an uneventful cataract surgery treated for anterior uveitis. -The AC inflammation persisted despite topical steroids for 2 months, and IOP was high. -PCIOL was in the bag and well covered by capsulorrhexis margin. -Dilated gonioscopy revealed superior haptic displacement due to a tear in equatorial bag. -This case highlights the importance of dilated gonioscopy and a rare possibility of UGH in an eye with a well-placed IOL. THANKS FOR YOUR ATTENTION