Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Leptospirosis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Oesophagostomum wikipedia , lookup
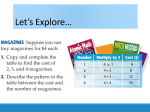
Am. J. Trop. Med. Hyg., 78(6), 2008, pp. 962–967 Copyright © 2008 by The American Society of Tropical Medicine and Hygiene Case-control Study of Armadillo Contact and Hansen’s Disease Brychan M. Clark, Clinton K. Murray,* Lynn L. Horvath, Gregory A. Deye, Mark S. Rasnake, and Robert N. Longfield Department of Infectious Diseases, Wilford Hall Medical Center, Lackland Air Force Base, Texas; Department of Medicine, Brooke Army Medical Center, Fort Sam Houston, Texas; U.S. Air Force Office of the Surgeon General, Medical Modernization Directorate, Pentagon, Falls Church, Virginia; Department of Medicine, University of Tennessee Graduate School of Medicine, Knoxville, Tennessee; Medicine Specialty Service, University of Texas at Tyler and Texas Center for Infectious Diseases, San Antonio, Texas Abstract. Hansen’s disease (HD) continues to have worldwide impact despite efforts to eradicate the disease. Although a definitive transmission mode has not been identified, data supports an association between HD and contact with the nine-banded armadillo. We conducted a case-control study of 28 HD patients to determine if there is an association between armadillo exposure and HD. There was no association between HD and place of birth or having hunted, consumed, or had direct or indirect contact with deer, birds, or squirrels. Univariate analysis showed that residence in Mexico (P ⳱ 0.001), hunting rabbits (P ⳱ 0.04), cleaning rabbits (P < 0.001), and armadillo exposure from hunting (P ⳱ 0.005), cleaning (P ⳱ 0.004), consuming (P ⳱ 0.002) them, or having direct armadillo contact (P ⳱ 0.017) were associated with HD. Multivariate analysis showed that eating armadillos (P ⳱ 0.039, odds ratio [OR] ⳱ 3.65, 95% confidence interval [CI] ⳱ 1.07–12.4), cleaning rabbits (P ⳱ 0.018, OR ⳱ 4.08, 95% CI ⳱ 1.27–13.1), and having lived in Mexico (P ⳱ 0.006, OR ⳱ 24.9, 95% CI ⳱ 2.52–245) were associated with HD. INTRODUCTION fluorescent antibody studies, mycolic acid analysis, and DNA analysis.9,10 Human HD related to armadillos has been described in many patients with close contact with armadillos and no other exposure risks.11–17 Arguing against an association is an age- and sex-matched study of 19 HD patients from Louisiana in 1977 that did not show an association with exposure to armadillos.18 Data regarding an association between contact with the nine-banded armadillo and the development of HD have been conflicting. Case-control studies to delineate an association between the two have not been adequately conducted. We conducted a retrospective case-control study of HD patients to determine if there is an association between armadillo contact or consumption and the subsequent development of HD. Hansen’s disease (HD), or leprosy, is a nationally reportable infectious disease in the United States that continues to have worldwide impact despite the commitment of the World Health Organization to eliminate the disease.1–3 Although most HD occurs in Latin America, Africa, Asia, and various islands in the western Pacific, there were 166 new cases reported in the United States in 2005, mostly in California, Louisiana, Texas, New York, Massachusetts, and Hawaii.3 Most cases that occur in the United States are in immigrants but autochthonous foci for HD transmission have also been recognized.2–4 Numerous modes of transmission have been proposed for HD but no mode is currently based on solid evidence. Traditionally, it was believed that the spread of infection was by respiratory droplets or by skin-to-skin contact. Although insect transmission in the laboratory has been previously described, this is unlikely to be a source of human infection.5 Hansen’s disease may also be zoonotic because it has been described in the armadillo, chimpanzee, and Mangabey monkey.2,6 Discovery of soil glycolipids from Mycobacterium leprae in armadillo habitats, the predominance of M. leprae in rural and not urban areas, transmission of M. leprae through dermal inoculation (tattoos), and the decreasing rate of disease in areas that have become more industrialized all suggest that, like with other non-tuberculous mycobacteria, soil might be a source of transmission.7 However, the inability to readily culture M. leprae from the environment is a significant barrier to investigating environmental reservoirs and related modes of transmission. The armadillo has been a research model for HD because of its cooler body temperature, reproductive rate, and similarity to human HD clinically after inoculation with M. lepraeinfected tissue.8 Nine-banded armadillos (Dasypus novemcinctus) in Louisiana were previously found to have a form of HD identical to human HD on the basis of histologic examination, MATERIALS AND METHODS Patients who were seen at the Texas Center for Infectious Diseases (San Antonio, TX) from January 2001 through June 2005, were eligible to participate in the study. The Texas Center for Infectious Diseases (TCID) is a public health facility of the Texas Department of State Health Services that provides inpatient treatment of patients with tuberculosis (TB) and outpatient treatment of patients with HD. Patients treated at TCID are all referred from the same regional area, which enabled control of geographic bias in the study. Study participants included males and females 18–100 years of age who were undergoing routine care for either HD or TB. These participants, including the control group, were asked to voluntarily participate in the study as they were evaluated in the clinic or inpatient ward for their underlying infection after the protocol was implemented at the site. Subjects were approached in a serial fashion initially; first all inpatients currently in the facility and then new admissions or outpatients as they came to the clinic until the number of participants and corresponding controls were obtained. Consent was obtained at the time of enrollment and a face-to-face interview by the primary or associate investigators using the study questionnaire was then performed. For every HD patient participating in the study, two control patients with M. tuberculosis infec- * Address correspondence to Clinton K. Murray, Department of Medicine, Brooke Army Medical Center, 3851 Roger Brooke Drive, Fort Sam Houston, TX 78216. E-mail: [email protected] 962 963 ARMADILLO CONTACT AND HANSEN’S DISEASE contrasts. Statistical analysis was performed using the software program SPSS version 13.0 (SPSS Inc., Chicago, IL). RESULTS FIGURE 1. Distribution of the nine-banded armadillo (Dasypus novemcinctus) in the United States, 1995. tion were enrolled and entered into the study. Selection of the control group was based on the patient population cared for at TCID and not an attempt to compare the two mycobacterial diseases. Routine clinical care was determined by the treating physician and was not influenced by participation in the study. A comprehensive questionnaire was administered to all study participants in either English or Spanish, depending on the patient’s native language. Demographic details collected included age, sex, race, date of diagnosis, place of birth, type of HD, and state and country of residence in childhood, adulthood, and at the time of diagnosis. Subjects were evaluated for having ever hunted, cleaned, eaten, or direct or indirect contact with armadillos, deer, rabbits, birds or squirrels, and where these activities took place. Exposure to a variety of animals rather than just armadillo exposure was evaluated by the study in an effort to minimize the potential for bias. The other animals were chosen because they are commonly encountered in activities such as hunting, butchering, gardening, frequently kept as pets, and consumed across the country, making regional geographic bias less likely. Subjects were asked if they knew of an association between animal contact and HD or, more specifically, armadillo contact and HD. Subjects were also asked if they had a family member with HD and whether the family member with HD had contact with armadillos. Direct contact was defined as having an armadillo, deer, rabbit, bird or squirrel for a pet, working in the field with direct contact with any of these animals, or preparing them for a meal. Indirect contact was defined as working in fields or gardens with any of these animals present or seen but not actually having direct contact with the animal. Residence in a given state was further classified as an armadilloinhabited area of the United States or a non-inhabited area. This classification was based on the known current and projected range of the nine-banded armadillo within the United States (Figure 1).19 The armadillo expansion map in Figure 1, adapted from Taulman and Robbins, illustrates the known established range of the nine-banded armadillo as of 1995 that included Texas, Oklahoma, Kansas, Missouri, Arkansas, Louisiana, Mississippi, Alabama, Tennessee, Georgia, South Carolina, Florida, and Illinois.19 Categorical variables were then compared with chi-square and Fisher’s exact tests, and multivariate analysis was performed using logistic regression with significance assigned to P values ⱕ 0.05. All categorical variables with P < 0.10 by univariate analysis were included in the multivariate model using backwards conditional logistic regression with simple From January 2001 through June 2005, a total of 28 HD patients and 59 controls were enrolled in the study. Of the study participants, HD patients were generally older than control patients at the time of diagnosis with a mean age of 52 years for HD patients compared with 43 years for control patients, but this difference was not statistically significant by univariate analysis (Table 1). Although Hispanics outnumbered Caucasians by nearly 2:1 and African-Americans by almost 3:1 (Table 1), there was no significant association between race and HD. Among HD patients, men outnumbered women 3:1 and were generally younger with a mean age of 50 years compared with a mean age of 57 years for women (Table 1). There was no statistically significant difference with regard to sex among the two groups. Most HD patients and controls had previously resided in an armadillo-inhabited area of the United States, specifically Texas, Oklahoma, Louisiana, Arkansas, Mississippi, Alabama, Florida, and Georgia. Among study participants, 64% of HD patients and 81% of control subjects reported living in Texas, either in childhood or as an adult, prior to their diagnosis. When study participants with armadillo exposure reported where their exposure to armadillos took place, it was almost always in Texas or Mexico. However, because most study participants with armadillo exposure did not report the location of their exposure, this variable could not be further analyzed. Within the HD study group, seven patients had tuberculoid HD, one had borderline tuberculoid HD, three had borderline HD, four had borderline lepromatous HD, eight had lepromatous HD, and five had either indeterminate HD or were not classified further. Because there were so few patients with a particular type of HD, further statistical analysis of this variable was not performed. Univariate analysis showed that there was no association between having HD and having hunted, consumed, or had direct contact with deer, birds, or squirrels, in fields or gardens, as pets, or in preparation of the animal meat for cooking (Tables 1 and 2). There was a trend toward an association between HD and having either direct contact with rabbits (P ⳱ 0.081, odds ratio [OR] ⳱ 2.24, 95% confidence interval [CI] ⳱ 0.90–5.6) or eating rabbit meat (P ⳱ 0.057, OR ⳱ 2.70, 95% CI ⳱ 0.95–7.63). Hunting rabbits (P ⳱ 0.04, OR ⳱ 2.59, 95% CI ⳱ 1.03–6.55), cleaning rabbits (P < 0.001, OR ⳱ 5.78, 95% CI ⳱ 2.18–15.4), cleaning birds (P ⳱ 0.012, OR ⳱ 3.39, 95% CI ⳱ 1.28–9.01), and armadillo exposure from hunting (P ⳱ 0.005), cleaning (P ⳱ 0.004), eating armadillo meat (P ⳱ 0.002), or having direct armadillo contact (P ⳱ 0.017) were all associated with HD by univariate analysis. All animal exposure occurred prior to diagnosis of either HD or TB. Among patients with HD who hunted armadillos, 67% also frequently ate the armadillos, whereas only 44% of the controls who hunted armadillos reported consuming armadillo meat (P ⳱ 0.002, OR ⳱ 1.74, 95% CI ⳱ 1.22–2.49). Among patients with HD who consumed armadillo meat, 60% also reported cleaning bird and rabbit meat compared with only 22% of controls. Hunting and cleaning of rabbits and arma- 964 CLARK AND OTHERS TABLE 1 Baseline characteristics of study participants* Multivariate analysis Characteristic HD (N ⳱ 28) TB (N ⳱ 59) Univariate analysis P† Mean age at diagnosis, years (range) Sex Male (% of patients) Female (% of patients) Race (%) Hispanic Caucasian African-American Other Place of birth (%) Mexico Armadillo-inhabited area of United States Areas of United States without armadillos Residence in childhood (%) Mexico Armadillo-inhabited area of United States Areas of United States without armadillos Residence as adult (%) Mexico Armadillo-inhabited area of United States Areas of United States without armadillos Type of Hansen’s disease (%) Tuberculoid Borderline tuberculoid Borderline Borderline lepromatous Lepromatous Indeterminate Family contact with Hansen’s disease 52 (21–76) 43 (22–70) 21 (75) 7 (25) 52 (88) 7 (12) NS NS 21 (75) 7 (25) 0 0 23 (39) 17 (31) 16 (25) 3 (5) 8 (29) 18 (64) 2 (7) 5 (8) 51 (86) 3 (5) 10 (36) 16 (57) 2 (7) 5 (8) 51 (86) 3 (5) 8 (29) 19 (64) 1 (4) 1 (2) 56 (95) 2 (3) 7 (25) 1 (4) 3 (11) 4 (14) 8 (29) 5 (18) 3 (11) 2 (3) OR (95% CI) P† 24.9 (2.52–245) 0.006 NS NS 0.01 0.001 NS * HD ⳱ Hansen’s disease; TB ⳱ tuberculosis; OR ⳱ odds ratio; CI ⳱ confidence interval; NS ⳱ not significant. † Significance was assigned to P values ⱕ 0.05. TABLE 2 Correlation of animal exposure and Hansen’s disease (HD)* Characteristic Hunted Armadillo Rabbits Deer Birds Squirrels Cleaned Armadillo Rabbits Deer Birds Squirrels Direct contact Armadillo Rabbits Deer Birds Squirrels Indirect contact Armadillo Rabbits Deer Birds Squirrels Consumption Armadillo Rabbits Deer Birds Squirrels HD Controls N ⳱ 28 (%) N ⳱ 59 (%) OR (95% CI) 12 (43) 17 (61) 13 (46) 12 (43) 8 (29) 9 (15) 22 (37) 19 (32) 18 (31) 17 (61) 4.17 (1.49–11.7) 2.59 (1.03–6.55) 0.005 0.040 NS NS NS 10 (28) 18 (64) 9 (32) 13 (46) 7 (25) 6 (10) 14 (24) 10 (17) 12 (20) 10 (17) 4.91 (1.56–15.4) 5.78 (2.18–15.4) 0.004 < 0.001 NS 0.012 NS 10 (28) 16 (57) 13 (46) 13 (46) 8 (29) 8 (14) 22 (79) 18 (31) 23 (39) 14 (24) 3.54 (1.21–10.4) 2.24 (0.90–5.60) 15 (54) 19 (68) 10 (28) 15 (54) 13 (46) 24 (41) 30 (51) 30 (51) 37 (63) 35 (59) 13 (46) 22 (78) 24 (86) 13 (46) 12 (43) 9 (15) 34 (58) 45 (76) 20 (34) 19 (32) * OR ⳱ odds ratio; CI ⳱ confidence interval; NS ⳱ not significant. † Significance was assigned to P values ⱕ 0.05. Univariate analysis 3.39 (1.28–9.01) Multivariate analysis P† OR (95% CI) P† NS NS 4.08 (1.27–12.4) NS 0.018 NS 0.017 0.081 NS NS NS NS NS NS NS NS NS NS 4.82 (1.72–13.5) 2.70 (0.90–7.65) 0.002 0.057 NS NS NS 3.65 (1.07–12.4) 0.039 NS ARMADILLO CONTACT AND HANSEN’S DISEASE dillos were highly collinear. Therefore, hunting these animals was excluded from the multivariate model because of the stronger association and more plausible intense exposure history between HD, cleaning rabbits (P ⳱ 0.001), and cleaning armadillos (P ⳱ 0.004). After multivariate analysis (Table 2), consumption of armadillos (P ⳱ 0.039, OR ⳱ 3.65, 95% CI ⳱ 1.07–12.4), cleaning rabbits (P ⳱ 0.018, OR ⳱ 4.08, 95% CI ⳱ 1.27–13.1), and having lived in Mexico (P ⳱ 0.006, OR ⳱ 24.9, 95% CI ⳱ 2.52–245) were all independently associated with HD. Logistic regression analysis showed that there was no significant correlation between HD and having hunted, cleaned, or had direct contact with armadillos. Cleaning birds, hunting rabbits and contact with rabbits in fields or gardens, as pets, or in preparation of the animal meat for cooking were also not associated with HD. More patients in the HD group than the control group had heard of an association between animals and HD (P ⳱ 0.001), but there was no difference between the two groups when it came to having heard specifically of an association between armadillos and the development of HD (P ⳱ 0.712). Few patients reported contact with HD cases within the home. For our study participants, there was no association between having HD and having a family member with HD. Only 2% of the controls reported living in Mexico as an adult compared with 29% of HD patients (P ⳱ 0.001). Univariate analysis showed that patients with HD were also more likely to report living as a child (P ⳱ 0.01) in Mexico, where the nine-banded armadillo has been present since the 14th century.16 Because childhood and adult residence in Mexico were highly collinear, only adult residence in Mexico was included in multivariate analysis because of the stronger association (P ⳱ 0.001 versus P ⳱ 0.01) with HD. When compared with the control group, patients with HD were 25 times more likely to have resided in Mexico as an adult (P ⳱ 0.006, OR ⳱ 24.9, 95% CI ⳱ 2.52–245) than in an armadillo-inhabited area of the United States. DISCUSSION As a public health facility, TCID provides treatment primarily for patients with TB and HD. The selection of the control group was based on the population available for study at TCID and was not an attempt to compare the two mycobacterial diseases. There were large numbers of Mexicanborn and Hispanic persons within the general population that served as the referral base for the study center. All study participants were referred from the same general area, which enabled control of geographic bias in the study. Our findings indicate that residing in Mexico, eating armadillos, and cleaning the dead carcass of a rabbit are all associated with human HD. Although there was some association by univariate analysis between HD and armadillo exposure from hunting, cleaning, or directly handling armadillos in fields, as pets, or in the preparation of armadillo meat for a meal, this did not remain significant after analysis by logistic regression. When compared with the control group, most (67%) patients with HD who had hunted armadillos also cleaned the dead carcass and ate the armadillo meat. Because cleaning armadillos had a stronger association with HD (P ⳱ 0.004, OR ⳱ 4.91, 95% CI ⳱ 1.56–15.4) than hunting armadillos did by univariate analysis (P ⳱ 0.005, OR ⳱ 4.17, 95% 965 CI ⳱ 1.49–11.7), hunting armadillos was excluded from the multivariate model because it was most likely a confounding variable. When hunting armadillos was controlled for in logistic regression analysis, patients who frequently ate armadillo meat were almost four times more likely to have HD than those who had never eaten an armadillo. Although cleaning rabbit meat was found to be associated with HD by multivariate analysis (OR ⳱ 4.08), it is unclear if this is a true association because most HD patients who had hunted, eaten, and cleaned armadillo meat also tended to clean bird and rabbit meat. Cleaning rabbit meat might be a confounder or a marker of exposure risk for some unidentified environmental risk factor that has yet to be discovered. Previous studies have reported conflicting data regarding an association between contact with the nine-banded armadillo and development of HD. In 1971, the armadillo was noted to be a research model for HD because of its cooler body temperature, reproductive rate, and similarity to human HD clinically after inoculation with M. leprae-infected tissue.8 In 1975, nine-banded armadillos in Louisiana were noted to have HD that was identical to human HD disease on the basis of histologic examination, fluorescent antibody studies, mycolic acid analysis, and DNA analysis.9,10 Human HD related to armadillos was first described in 1981 when a Texas rancher with HD was noted to have significant armadillo contact but no other exposure risks such as contact with HD patients or travel overseas.11 In 1983 and 1984, 6 cases of HD were described with associated close contact with armadillos but no other exposure risks were noted.12,13 A 1987 study in Los Angeles, California, showed an association among Mexican-born patients with HD and armadillo exposure.14 The relative risk for Mexican-born males was an OR of 6.5 for direct exposure and an OR of 2.7 for indirect exposure, whereas for Mexican-born females, the OR was 4.1 for direct exposure and 3.5 for indirect exposure.14 In 1988, 6 cases of HD were described in residents of a non-endemic area of northern Louisiana with significant armadillo exposure as the only risk factor for HD.15 More recently, a case of HD was reported in a woman from Georgia with no other exposure risks other than frequently working in a garden where armadillos burrowed or were buried.16 A study in 2000 showed that 71% of non-Asian patients with HD in Houston, Texas, reported direct or indirect contact with armadillos compared with none of the Asian patients with HD (P < 0.001).17 Arguing against an association between armadillo contact and HD is a 1977 age- and sex-matched study of 19 HD patients from Louisiana that did not show an association with exposure to armadillos.18 Our study found that consumption of armadillos, and possibly to a lesser extent, cleaning the bloody carcass of a dead armadillo and direct armadillo contact were associated with HD. Unlike the previous study that showed an association among Mexican-born patients and HD, we found no correlation between place of birth and HD. Although there were disproportionately more Hispanic patients in the HD group than the control group, we found no significant association between race and having HD. Because all study participants came from the same general referral area that contained a high percentage of Hispanic and Mexican-born persons among the general population, the possibility of an unintended selection bias is less likely. Previously residing in Mexico, where armadillos have been present for many centuries, seemed to be the most important risk factor 966 CLARK AND OTHERS in our study for acquiring leprosy with an odds ratio of 24.9. Because only 2% of controls reported living in Mexico as an adult compared with 29% of HD patients (P ⳱ 0.001), an environmental bias may have been introduced if the migration from rural to more urban areas coincided with migration from Mexico to the southern part of the United States, specifically Texas. Although our findings support most of the previously published literature regarding an association between armadillo contact and HD, further studies that match for race, age, and residence in Mexico may eliminate any potential bias that might reflect a person’s habits associated with their ethnicity or living in rural areas. Hansen’s disease has affected humans throughout recorded history. Because of an exceptionally stable genome, M. leprae can be a helpful marker for tracking the migration of people over time.20 The M. leprae strain in North America is genetically closest to that found in Europe and west Africa and was likely transported by colonial and migratory voyages.20 Wild armadillos from Louisiana, which have been found to be naturally infected with M. leprae, harbor the European/North African SNP type 3 strain, indicating that they acquired the infection from human sources.20 There is currently little direct evidence of an environmental source or reservoir of M. leprae, other than armadillos.20 Other Mycobacterium, such as M. ulcerans, can be transmitted to humans by insect bites, and various nontuberculous mycobacteria have well-described environmental reservoirs.21 Although transmission of viable M. leprae from HD patients to mice has been shown to occur in the laboratory, it is unlikely to be a source of human infection.5,22 The presence of M. leprae phenolic glycolipids in the soil of armadillo habitats, the predominance of M. leprae in rural areas, transmission of M. leprae through dermal inoculation (tattoos), and the decreasing rate of disease in industrialized areas all suggest that soil might be a potential source of transmission.7 However, the inability to readily culture M. leprae from the environment has proven to be a significant barrier to investigating environmental reservoirs and other related modes of transmission.23,24 Population serosurveys in disease-endemic areas have demonstrated antibodies to M. leprae phenolic glycolipid I among otherwise healthy persons, and it has been postulated that people are exposed to a common source of the bacillus, perhaps in the environment, although no environmental reservoir of M. leprae, other than armadillos, has been demonstrated to date.25,26 Although eating armadillos and cleaning rabbits were associated with human HD in our study, living in Mexico seemed to be the most important risk factor, indicating that contact with an, as yet uncharacterized, environmental reservoir of M. leprae might account for transmission of the disease. Further elucidation of the mode or modes of transmission of M. leprae would be important in prevention and control of HD. Received September 28, 2007. Accepted for publication February 7, 2008. Disclaimer: The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the U.S. Department of the Army, the U.S. Department of the Air Force, the U.S. Department of Defense, or the U.S. government. Disclosure: The authors are employees of the U.S. government and this work was performed as part of their official duties. As such, there is no copyright to be transferred. Authors’ addresses: Brychan M. Clark, Department of Medicine, Mike O’Callaghan Federal Hospital, 4700 Las Vegas Boulevard North, Nellis Air Force Base, NV 89191. Clinton K. Murray and Lynn L. Horvath, Department of Medicine, Brooke Army Medical Center, 3851 Roger Brooke Drive, Fort Sam Houston, TX 78216. Gregory A. Deye, Walter Reed Army Institute of Research, 503 Robert Grant Avenue, Silver Spring, MD 20910. Mark S. Rasnake, Department of Medicine, University of Tennessee Graduate School of Medicine, 1924 Alcoa Highway, Knoxville, TN 37920. Robert N. Longfield, Medicine Specialty Service, University of Texas at Tyler and Texas Center for Infectious Diseases, 2303 SE Military Drive, San Antonio, TX 78223. REFERENCES 1. World Health Organization Expert Committee on Leprosy, 1998. World Health Organ Tech Rep Ser 874: 1–43. 2. Ooi WW, Moschella SL, 2001. Update on leprosy in immigrants in the United States: status in the year 2000. Clin Infect Dis 32: 930–937. 3. Truman R, Kearney MT, Lea JW, 2006. A Summary of Hansen’s Disease in the United States – 2005. Washington, DC: U.S. Department of Health and Human Services, National Hansen’s Disease Program, Health Resources and Services Administration Registry Report, 1–32. 4. Taylor JP, Vitek I, Enriquez V, Smedley JW, 1999. A continuing focus of Hansen’s disease in Texas. Am J Trop Med Hyg 60: 449–452. 5. McDougall AC, Cologlu AS, 1983. Lepromatous leprosy in man; depth of the cellular infiltrate and bacillary mass in relation to the possibility of transmission of leprosy by biting arthropods. Ann Trop Med Parasitol 77: 187–193. 6. Walsh GP, Meyers WM, Binford CH, Gerone PJ, Wolf RH, Leinenger JR, 1981. Leprosy - a zoonosis. Lepr Rev 52: 77–83. 7. Blake LA, West BC, Lary CH, Todd JR, 1987. Environmental nonhuman sources of leprosy. Rev Infect Dis 9: 562–577. 8. Storrs EE, 1971. The nine-banded armadillo: a model for leprosy and other biomedical research. Int J Lepr 39: 703–714. 9. Walsh GP, Storrs EE, Burchfield HP, Cotrell EH, Vidrine MF, Binford CH, 1975. Leprosy-like disease occurring naturally in armadillos. J Reticuloendothelial Soc 18: 347–351. 10. Walsh GP, Meyers WM, Binford CH, 1986. Naturally acquired leprosy in the nine-banded armadillo: a decade of experience 1975–1985. J Leuk Biol 40: 645–656. 11. Freiberger HF, Fudenberg HH, 1981. An appetite for armadillo. Hosp Pract 16: 137–144. 12. Lumpkin LR, Cox GF, Wolf JE, 1983. Leprosy in five armadillo handlers. J Am Acad Dermatol 9: 899–903. 13. Lumpkin LR, Cox GF, Wolf JE, 1984. Leprosy in armadillo handlers. J Am Acad Dermatol 10: 1073. 14. Thomas DA, Mines JS, Thomas DC, Mack TM, Rae TH, 1987. Armadillo exposure among Mexican-born patients with lepromatous leprosy. J Infect Dis 156: 990–992. 15. West C, Todd JR, Lary CH, 1988. Leprosy in six isolated residents northern Louisiana. Ann Intern Med 148: 1987–1992. 16. Lane JE, Walsh DS, Meyers WM, Klassen-Fischer MK, Kent DE, Cohen DJ, 2006. Borderline tuberculoid leprosy in a woman from the state of Georgia with armadillo exposure. J Am Acad Dermatol 55: 714–716. 17. Bruce S, Schroeder TL, Ellner K, Rubin H, Williams T, Wolf JF Jr, 2000. Armadillo exposure and Hansen’s disease: an epidemiologic survey in southern Texas. J Am Acad Dermatol 43: 223–228. 18. Filice GA, Greenberg RN, Fraser DW, 1977. Lack of observed association between armadillo contact and leprosy in humans. Am J Trop Med Hyg 26: 137–139. 19. Taulman JF, Robbins LW, 1996. Recent range expansion and distributional limits of the nine-banded armadillo (Dasypus novemcinctus) in the United States. J Biogeography 23: 635– 648. 20. Monot M, Honore N, Garneir T, Araoz R, Coppee JY, Lacroix C, Sow S, Spencer JS, Truman RW, Williams DL, Gelber R, Virmond M, Flageul B, Cho SN, Ji B, Paniz-Mondolfi A, Con- ARMADILLO CONTACT AND HANSEN’S DISEASE 21. 22. 23. 24. vit J, Young S, Fine PE, Rasolofo V, Brennan PJ, Cole ST, 2005. On the origin of leprosy. Science 308: 1040–1042. Marsollier L, Robert R, Aubry J, Saint Andre JP, Kouakou H, Legras P, Manceau AL, Mahaza C, Carbonnelle B, 2002. Aquatic insects as a vector for Mycobacterium ulcerans. Appl Environ Microbiol 68: 4623–4628. Banerjee R, Banerjee BD, Chaudhury S, Hati AK, 1991. Transmission of viable Mycobacterium leprae by Aedes aegypti from lepromatous leprosy patients to the skin of mice through interrupted feeding. Lepr Rev 62: 21–26. Shepard CC, McRae DH, 1965. Mycobacterium leprae in mice: minimal infectious dose, relationship between staining quality and infectivity, and effect of cortisone. J Bacteriol 89: 365–372. Kirchheimer WK, Storrs EE, 1971. Attempts to establish the ar- 967 madillo (Dasypus novemcinctus Linn.) as a model for the study of leprosy. I. Report of lepromatoid leprosy in an experimentally infected armadillo. Int J Lepr Other Mycobact Dis 39: 693–702. 25. Krishnamurthy P, Rao PS, Reddy BN, Subramanian M, Dhandayudapani S, Bhatia V, Neelan PN, Dutta A, 1991. Seroepidemiological study of leprosy in a highly endemic population of south India based on an ELISA using synthetic PGL-I. Int J Lepr Other Mycobact Dis 59: 426–431. 26. Moet FJ, Pahan D, Schuring RP, Oskam L, Richardus JH, 2006. Physical distance, genetic relationship, age and leprosy classification are independent risk factors for leprosy in contacts of patients with leprosy. J Infect Dis 193: 346–353.