Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
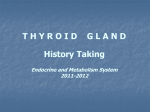
Nuclear Medicine Communications Response rate and factors affecting outcome of fixed dose of RAI131 therapy in Graves` disease: A 10 year Egyptian experience --Manuscript Draft-Manuscript Number: NMC-11-1171R1 Full Title: Response rate and factors affecting outcome of fixed dose of RAI131 therapy in Graves` disease: A 10 year Egyptian experience Article Type: Review Article Keywords: Graves` disease; Radioactive iodine therapy; fixed dose; Tc-99 pertechnetate thyroid uptake. Corresponding Author: Maha Abd Elkareem Husseni, M.D Kasr A l Ainy hospital, cairo university Cairo, EGYPT Corresponding Author Secondary Information: Corresponding Author's Institution: Kasr A l Ainy hospital, cairo university Corresponding Author's Secondary Institution: First Author: Maha Abd Elkareem Husseni, M.D First Author Secondary Information: Order of Authors: Maha Abd Elkareem Husseni, M.D Wajeeh Abdulrazak Derwish, M.sc Hosna Mohammed Moustafa, Professor Order of Authors Secondary Information: Manuscript Region of Origin: EGYPT Abstract: Purpose: Evaluate response and compare success rate of two different doses of I-131 therapy in treatment of Graves` disease and investigate the factors that may affect outcome. Patient and methods: Retrospective analysis was performed on 321 patients treated with I-131 for Graves` disease. Group 1 (155 patients) received 8 mCi and Group 2 (166 patients) received 12 mCi. The therapy was considered successful if euthyroidism or hypothyroidism was achieved within one year of therapy. The outcome was compared with multiple parameters. Results: Significant difference in the outcome between the two groups was found in favor of the second group (P<0.001). Logistic regression analysis revealed that lower dose, Tc-99 pertechnetate thyroid uptake > 20.9 %, moderate and marked goiter were independent variables that significantly associated with less response rate (OR 2.601, 4.023 and 3.309 respectively) and prior surgical treatment with higher response rate (OR 3.071). No correlation between outcome and age, presence of exopthalomos, previous treatment with methimazole and its duration was found. Response rate to the second dose was significantly increased compared to the first one by 27.8 %, there was no correlation among the above mentioned factors and its outcome. The third dose controlled 81.3 % of the remaining patients and the rest were achieved controlled after the fourth dose. Conclusions: I-131 is very effective therapy for Graves` disease with cure rate 100% after 4 doses. Higher first dose activity is recommended in the presence of poor prognostic factors. Second dose is not necessary increased in the non responders. Powered by Editorial Manager® and ProduXion Manager® from Aries Systems Corporation Response to Reviewers 1 Response rate and factors affecting outcome of fixed dose of RAI131 therapy in Graves` disease: A 10 year Egyptian experience Maha Abd El-Kareem M.D, Wajeeh Abdulrazak Derwish M.sc and Hosna Mohamed Moustafa M.D Department of radiotherapy and nuclear medicine (NEMROCK), Nuclear medicine unit, Cairo University. Abstract Purpose: Evaluate response and compare success rate of two different doses of I-131 therapy in treatment of Graves` disease and investigate the factors that may affect outcome. Patient and methods: Retrospective analysis was performed on 321 patients treated with I-131 for Graves` disease. Group 1 (155 patients) received 8 mCi and Group 2 (166 patients) received 12 mCi. The therapy was considered successful if euthyroidism or hypothyroidism was achieved within one year of therapy. The outcome was compared with multiple parameters. Results: Significant difference in the outcome between the two groups was found in favor of the second group (P<0.001). Logistic regression analysis revealed that lower dose, Tc99 pertechnetate thyroid uptake > 20.9 %, moderate and marked goiter were independent variables that significantly associated with less response rate (OR 2.601, 4.023 and 3.309 respectively), while prior surgical treatment with higher response rate (OR 3.071). No correlation between outcome and age, presence of exopthalomos, previous treatment with 1 2 methimazole and its duration was found. Response rate to the second dose was significantly increased compared to the first one by 27.8 %, there was no correlation among the above mentioned factors and its outcome. The third dose controlled 81.3 % of the remaining patients and the rest were achieved controlled after the fourth dose. Conclusions: I-131 is very effective therapy for Graves` disease with cure rate 100% after 4 doses. Higher first dose activity is recommended in the presence of poor prognostic factors. Second dose is not necessary increased in the non responders. Keywords: Graves` disease; radioactive iodine therapy; fixed dose- Tc-99 pertechnetate thyroid uptake. Introduction: Graves` disease (GD) is the most common cause of hyperthyroidism responsible for approximately 50-60% of the cases (1). The most common clinical presentations related to the cardiovascular system. Other disease manifestations include Graves’ ophthalmopathy and myxedema(2). Diagnostic modalities include suppressed serum TSH and an elevated serum FT4, FT3 levels, thyroid scintigraphy either with Tc99m pertechnetate or radioactive iodine-131 (RAI-131) and ultrasonography (U.S) to detect the presence of an associated nodules (3). Three therapeutic modalities are commonly used today; anti-thyroid drugs (ATDs), RAI-131 and surgical treatment (3). The aim of RAI -131 treatment is to cure the hyperthyroidism by rendering the patient either euthyroid or hypothyroid through destruction of the over-functioning thyroid tissues (4). The use of RAI-131 in treatment of GD is increasing, particularly as a first line treatment (5) as it is easy to administer, relatively inexpensive, reliable , safe and highly effective with a cure rate approaching 100% after one or more dose (6) . Different 2 3 methods have been used for determining the administered activity, varied from fixed doses to adjusted calculations based on gland size, iodine uptake and turnover (7). The dose calculation method aims to optimize the therapeutic results through administration of radioactive iodine in proportional to the size of the gland, increasing the probability of cure and providing the lowest possible radiation dose to the rest of the body (8). There is little evidence that using a calculated dose has any advantage over a fixed-dose regimen in preventing hypothyroidism or improvement in cure rate (9), but it increases significantly the cost of the therapy owing to increase the procedure complexity (10). Taking in mind that the radioactive iodine therapy is relatively inexpensive, thus the increase in its cost to determine the administered activity must be clearly justified (10). There are some predictive factors associated with RAI-131 success rate. Previous works have shown lower treatment success rates in young male patients, more severe cases of hyperthyroidism (11)(12) , larger goiters (12) (13) and in cases with low or high pretreatment thyroid uptake (12) (14). The influence of pretreatment with anti-thyroid drugs on the efficacy of radioiodine therapy is controversial. Some authors believe that the thyrostatic drugs methimazole (MMI) and propylthiouracil (PTU) have a radioresistance effect and can lead to half-life reduction and accelerate turnover (15) (16) (17), but others have shown an effect confined to PTU only (18). Patients and Methods: We retrospectively evaluated 321 hyperthyroid patients due to GD referred to the nuclear medicine unit, Kasr Al ainy hospital (NEMROK), Cairo University, during the period of January 2000 till January 2010 for RAI-131 therapy as first or as a second treatment modality (following medical or surgical treatment). Our 3 4 institutional medical ethics committee approved the protocol. The diagnosis of GD was primarily based on clinical (hyperthyroid manifestations and diffusely enlarged thyroid gland) and laboratory data, including high serum free T4 level (FT4; reference Values, RV = 0.9 - 1.8 ng/dL) and low serum thyrotropin levels (TSH; RV = 0.41- 4.5 µ IU/mL). The patients who had thyrotoxicosis due to toxic multi-nodular goiter (Plummer disease), toxic autonomous adenoma, GD associated with (cold) nodule by (scan) or palpation respectively and patients who not completed the follow up were excluded from the study. Data were retrieved from the thyroid clinic database include: age at diagnosis, gender, symptoms, dose and duration of anti-thyroid drugs , previous surgical treatment, clinical data for the presence of palpable nodules & other neck swellings and the presence or absence of eye signs, TSH level and thyroid scan using Tc-99m pertechnetate that was done 20 min after intravenous injection of 5 mCi of the tracer to evaluate the associated nonfunctioning (cold) nodule and quantitation of thyroid uptake using the methodology previously described by Maisey et al(19) and simplified for routine use. The reference values for Tc-99m pertechnetate uptake range from 0.3 to 4 % (20). Gland size were determined by combining clinical examination (palpation) and thyroid scan and was divided in to either normal size (impalpable), mild (palpably enlarged but not visible) and moderate or markedly enlargement (palpable and visible goiter). In view of our socioeconomical circumstances; the simple fixed dose protocol has considerable cost saving advantages, we have adopted this protocol for the treatment of GD in our institution. The patients were divided according to the given RAI-131 dose in to 2 groups: Group 1: 4 5 received 8 mCi (155 patients) (48.3%) and Group 2: received 12 mCi (166 patients) (51.7%), they are the commonly preferred doses in the treatment of GD in our institute. Anti-thyroid drugs, if given before therapy, were withdrawn a week before therapy and for a minimum of 1 week after to avoid any drug influence on the therapeutic effectiveness. Iodine-containing medications were also discontinued several weeks before therapy; in addition, the patients were started on a low-iodine diet for 10 days before therapy, fasted before and for 2 hours after the administration of the dose to achieve higher absorption. Patients were advised to avoid physical contact and transfer of secretions to others for several days after treatment. Regular clinical and laboratory follow up to evaluate therapeutic efficacy was done and the patients were classified according to the outcome in to: Euthyroidism: Absence of signs or symptoms of hyperthyroidism or hypothyroidism with normal serum TSH value without levothyroxin therapy. Resistant to therapy: persistence of thyrotoxic manifestation and suppressed TSH value or by requirement of repeat administration of RAI-131 therapy within 6 months of the therapy and Hypothyroidism: presence of symptoms or signs of hypothyroidism together with elevated TSH value on two occasions four weeks apart, that require permanent treatment with levothyroxine. RAI-131 treatment was considered to be successful if the patient was either euthyroid or hypothyroid. Statistical methods: Data was analyzed using IBM SPSS advanced statistics version 20 (SPSS Inc., Chicago, IL). Numerical data were expressed as mean and standard deviation or median and range as appropriate. Qualitative data were expressed as frequency and percentage. Chi-square test (Fisher’s exact test) was used to examine the relation between 5 6 qualitative variables. For quantitative data, comparison between two groups was done using Mann-Whitney test (non-parametric t-test). The receiver operator characteristic (ROC) curve was used to identify the best threshold for thyroid uptake to discriminate success and failure of RAI-131 therapy. Multivariate analysis was done using forward stepwise logistic regression method for the significant factors affecting response on univariate analysis. Odds ratio (OR) with 95% confidence interval (CI) were used for risk estimation. P-value < 0.05 was considered significant. Results:. Baseline, pre-therapy clinical characteristics and commonly presenting symptoms for the patients are listed in Table 1 and 2. The recorded data documented development of early complications within the 1st 3 months in 31 patients (9.6%), included transient mild increased thyrotoxic manifestations in 21 patients and transient hypothyroidism which occurred for 8 patients, 5 after a high dose and 3 after low dose. Six of the 8 patients developed transient hypothyroidism after 1st dose, while the remaining 2 patients developed it after 2nd dose. Also neck pain developed in 2 patients. There was statistically significant difference in the incidence of early complications between the patients who received 8 mCi and the second group who received 12 mCi, in favor of the latter group (p = 0.024), whereas as there was no statistically significant difference between age, gender, presence of exopthaloms, size of thyroid gland and thyroid uptake and early complications either between the two groups as shown in the table (3) or in each group separately (not included). Exopthalmos was increased in 9 patients (9.6%) after RAI-131 therapy and remained stationary in rest. Three new cases (1.3%) developed exophthalmos from the remaining 6 7 227 patients and they were among the 170 patients who had permanent hypothyroidism (1.7%). No relation was found between the presence of exopthalmos and development of early complications as shown in tables 3. The success rate to the first given dose was 59.8% with development of euthyroidism in 56 patients (17.4%) and hypothyroidism in 136 patients (42.4%). There was statistically significant difference in the successes rate between the patients who received 8 mCi (49%) and 12 mCi (69.9%) P <0.001. Of the 76 patients in whom therapy was successful in group1, 25 (16.1%) developed euthyroidism and 51(32.9 %) developed hypothyroidism and at a median period of 6 months (range: 3 –18 months) and among the 116 responding patients in the second group, euthyroidism was achieved in 37 patients (22.3%) and hypothyroidism in 79 patients (47.6%) with a median cure time 4 months (range: 2 –18 months). There was no statistically significant association between age, presence of ophthalmopathy and previous medical treatment & its duration and outcome, whereas there was statistically significant difference regarding gender, size of thyroid gland, Tc99m pertechnetate thyroid uptake and previous surgical treatment as demonstrated in table 4. We did not find any relationship between the previous use of methimazole & its duration and the outcome of patients either in the whole study population or G1 and G2 separately (tables 4 and 5 A&B). Thyroid uptake was analyzed using ROC curve to discriminate the group of patients who achieved success with treatment from the group that remained hyperthyroid and we found a thyroid uptake threshold of 20.9 % with a sensitivity of 76.1 % and specificity of 65.4 7 8 % for treatment success (Fig. 1). We were unable to find an adequate cutoff value for base line TSH level. Multiple logistic regression analysis demonstrated that age, gender and previous medical treatment were not significantly associated with the outcome, whereas Tc99m pertechnetate thyroid uptake > 20.9% (OR= 4.023) , moderate and markedly enlarged thyroid gland (OR= 3.309) and the low given dose (OR= 2.601) were identified as significant prognostic risk factors for treatment failure and previous thyroidectomy for treatment success (OR= 3.071) (odds ratio; 95% confidence interval = 2.218 -7.297, 1.707 - 6.414, 1.403 - 4.822 and 1.109 - 8.502 respectively). Response to the second dose: A second dose was given to the 129 non responded patients after a mean time of 6.77 months (minimum 3 months and maximum 12 months). Of these 63 patients received 8 mCi and 66 received 12 mCi. The overall response rate to the second therapy dose significantly increased compared to the first one by 27.8 % with development of euthyroidism in 56 patients (17.4%) and hypothyroidism in 136 patients (42.4%). There was no statistically significant difference in the response rate between the patients who received 8 mCi and who received 12 mCi (P value = 0.921), also there was no statistically significant difference in the response rate in relation to size of thyroid gland, Tc99m pertechnetate thyroid uptake, previous surgical treatment, age and gender (p values 0.265, 0.665, 0.242, 0.209 and 0.923 respectively) as shown in table 6. Fifty two patients from the 79 non responded in the first group received second dose of 8 mCi while the remaining 27 patients received 12 mCi. 8 There was no statistically 9 significant difference in the response rate between the patients received 8 mCi (86%) and 12 mCi (92.6 %) with P value = 0.422. No statistically significant difference in the response rate in relation to size of thyroid gland, Tc-99m pertechnetate thyroid uptake and previous surgical treatment was found (p values = 0.436, 0.225 and 0.361 respectively). Eleven from the 50 non responded patients in the second group were received second dose 8 mCi while the other 39 patients received 12 mCi. There was no statistically significant difference in the response rate between the patients received 8 mCi (90.9 %) and 12 mCi (384.6 %) with P value = 0.595 and no statistically significant difference in the response rate in relation to size of thyroid gland, Tc99m pertechnetate thyroid uptake and previous surgical treatment (p values = 0.418, 0.117 and 0.471 respectively). Thirteen patients from the remaining 16 non responders to the second dose responded to the 3rd RAI-131 dose with development of euthyroidism in 7 patients (43.8 %) and hypothyroidism in the remaining 6 patients (37.5%). The 4th dose controlled the remaining 3 patients with development of hypothyroidism in 2 patients and euthyroidism in the third. The median dose for controlling GD was 12 mCi (minimum 8 mCi which controlled 23.7% of the patients and maximum 47 mCi), the doses of 12 mCi, 16 mCi, 20 mCi, 24 mCi, 28 mCi, 32 mCi, 36 mCi, 43 mCi and 47 mCi increase the overall control rate to 59.8 %, 74.1%, 85%, 96%, 96.9%, 97.8%, 99.4%, 99.7% and 100% respectively as shown in table 7. The mean dose number for controlling the hyperthyroidism was 1.46 ± 0.62 (range 1- 4). The first dose controlled 59.8% of the patients, this percent increased to 95% after the second dose, 99.1% following the third one and 100% after the fourth dose 9 10 as shown in table 8. Discussion: About 80% of experts from Europe preferred to start treatment with ATDs in patients over 21 years and 70% of those in the United States RAI is the initial treatment modality of choice (21). In Egypt the ATDs represent, for most endocrinologists, the initial choice of treatment. This trend was reflected in the present study, where only 22.4% of the patients underwent RAI as initial treatment modality, while 77.6% patients were previously treated with ATDs. The influence of ATDs on the outcome of RAI treatment has received attention. Some studies have suggested that ATD treatment before or after RAI may provide a radioprotective effect for the thyroid with significantly shortened the biological half-life of RAI result in reduction of the absorbed dose and increased failure rate of single-dose RAI treatment (16-17) (22). Thionamide withdrawal was among the predictive factors for treatment success in a 10-mCi fixed-dose approach (23). More over Alexander et al. treated 261 Graves’ patients with a mean dose of 14.6 mCi of RAI demonstrated high risk of treatment failure in patients pretreated with anti-thyroid medications for greater than 4 months(12). Other studies stated that this effect confined to the use of propylthiouracil only (18). In contrast Braga et al. (24) and Andrade et al. (25) demonstrated that methimazole pretreatment has no effect on the final treatment result, including the time required for cure or the 1-year success rate of RAI therapy. Thientunyakit T et al. (26) showed that duration of anti-thyroid drug given prior to radioiodine therapy seemed not related to the treatment outcome. Moura-Neto also found that no statistically significant association between thyroid function outcome to a fixed, 10 11 15 mCi approach for treatment of Graves’ hyperthyroidism and drug used (methi-mazole or propylthiouracil; maintenance or withdrawal of thionamides prior to therapy (27). Our results were in agreement with the later ones, where we don’t find statistical significant difference between pre-iodine medical treatment or its duration and the outcome to RAI131 therapy. Surgery is no longer recommended as first-line therapy for GD and use in selective cases where RAI is not preferred and ATDs fail to control the disease(3). Lal et al. concluded that total thyroidectomy (TT) is much better than Subtotal thyroidectomy (STT) (28). In the present study, STT was performed in only 49 patients (15.3%) with recurrent of disease in all of them at a median period of 66 months, confirming the literature data of using it as an alternative option in selected patients. The size of thyroid gland is an important factor influencing the outcome of therapy; In our study, mildly enlarged glands had more controlled rate than moderate or markedly enlarged thyroid gland with higher incidence of hypothyroidism ( P = 0.042). This result is in agreement with the other multiple studies which have demonstrated that patients with larger-volume thyroid glands to fail to respond to a single dose of radioiodine (2327-29-30-31-32). The impact of thyroid uptake on the RAI outcome has been investigated using either 131I or Tc99m pertechnetate. Alexander et al (12) found that patients who have higher 24hour thyroid RAI uptake values were at higher risk than others for treatment failure. Kung et al. (32) also identified 4-hour RAI uptake among the variables that could predict early treatment outcome for Graves’ disease. These results were in agreement with other 11 12 works demonstrating higher failure rates in patients with higher iodide thyroid uptake values which could reflect faster iodide turnover in thyroid cells thus making the residence time of therapeutic I-131 in the gland shorter (33). The authors suggested that a higher radioactivity of RAI be given to these patients. Using Tc99-m sodium pertechnetate Zantut-Wittmann et al. (23) have reported that in a 10 mCi fixed dose approach the pre-RIT Tc99-m sodium pertechnetate uptake under 12% among the predictive factors for treatment success. In contrast, Moura-Neto et al. stated that no statistically significant association between thyroid function outcome to a fixed 15 mCi approach for treatment of GD and Tc-99m sodium pertechnetate thyroid uptake prior to therapy(27). Tc-99 m pertechnetate uptake is routinely used in our department as a surrogate measure of thyroid uptake because it has been proved to possess a good correlation with iodide 125 uptake (34). Moreover, it is much less expensive, reliable and convenient method allows uptake within 20 minutes after intravenous injection of the radionuclide and the therapeutic dose of RAI can be administered immediately after. We found that Tc-99m pertechnetate thyroid uptake more than 20.9% was among the poor prognostic factors for the response, thus higher dose is recommended. The different RAI doses have different impact on the thyroid gland function, less than half of the patients (49%) in group 1 who received low dose of RAI achieved cure. On the other hand 69.4 % from the second group, who received higher dose of RAI, had achieved cure. This means that higher dose of RAI increase response rate by ~ 20.4 %. Franklyn et al.(35) and Sankar et al.(36) studied the therapeutic outcome of low fixed dose of RAI, the former concluded that persistent hyperthyroidism after 6 months was 12 13 present in 55.9% of the patients using small fixed dose of 5 mCi of RAI and the latter recommended increase dose of RAI to achieve response. This agree with Nordyke and Gilbert (29) who analyzed a series of 605 patients treated with RAI to find out the optimal dose to achieve cure and they concluded that cure was directly related to the dose of RAI administered and the optimal dose for curing hyperthyroidism is approximated by starting with 10 mCi and increasing it for unusually large glands or for special patient circumstances. In the present study, 88% of patients achieved cure after administration of second dose of RAI with no statistically significant difference was found between the success rate and the given dose, only few patients require 3rd or 4th doses. This is in concordant with Sanyal et al. (37) and Franklyn et al. (35) studies that demonstrated high cure rate to the second dose of RAI ( 82.4% and 74.5% respectively) with only few require other doses. Although it is very rare, McDermott et al.(38) reported thyroid storm in a small number of patients between 1 and 14 days after treatment with RAI. In the present study thyroid storm did not encountered in any patient. Also, Levy et al.(39) in a series of 7000 patients treated with RAI in one centre, none developed this complication. Ponto et al. (40) concluded that RAI therapy for GD is associated with definite increased risk of GO in around 20% of patients (either developing new cases or worsening of preexisting one). However In the present work there was worsening of exophtalmus in 9.6 % of the patients and three new cases were developed (1.3%) among the rest who did not have 13 14 prior exopthalmos, they were among the 177 patients who developed permanent hypothyroidism. Conclusion: Radioiodine is clearly successful in curing hyperthyroidism in GD patients by 100 % after 4 doses; therefore it should be used as a first standard line in treatment. Treatment results using fixed RAI dose are comparable to those studies of patients treated with RAI using the prescribed absorbed dose method. The standard-dose prescription strategy is therefore an efficient, cost-effective and is also convenient to the patient. It may be possible to improve cure rates using a single fixed-dose regimen without increasing the dose in all patients. This might be achieved by the identification of subjects with poor prognostic factors who are unlikely to respond to standard doses and by administering larger doses only to these individuals. A higher fixed (12 mCi) is more effective than lower dose (8 mCi) for treatment of GD leading to better control of the disease following the first dose. Higher response rate are expected in patients who underwent previous surgery, on contrary patients with larger goiters and high thyroid uptake > 20.9% had 3.3 and 4 times less chance of remission. This different impact of different doses on the response rate is applied to the first dose, but not to the second dose where the response rate to the second dose is nearly similar in both low and high dose groups. References: [1]. McKenzie, J M, Zakarija, M and Sato, A. Humoral immunity in Graves' disease. Clinics in endocrinology and metabolism 1978; 7:31-45. 14 15 [2]. Reid, JR and Wheeler, SF. Hyperthyroidism: diagnosis and treatment. American family physician 2005; 72:623-630. [3]. Bahn, RS, Burch, HB, Cooper, DS, Garber, JR, Greenlee, MC, Klein, I, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists Endocrine practice 2011; 17:456-520. [4]. Isgoren, S, Daglioz Gorur, G, Demir, H, and Berk, F. Radioiodine therapy in Graves' disease: is it possible to predict outcome before therapy?. Nuclear medicine communications 2012; 33:859-863. [5]. Hedley, AJ, Lazarus, JH, McGhee, SM, Jones, RB, Sharp, PF, Naven, LM, et al.. Treatment of hyperthyroidism by radioactive iodine. Summary of a UK national survey prepared for the Royal College of Physicians Committee on Endocrinology and Diabetes. Journal of the Royal College of Physicians of London 1992; 26:348-351. [6]. Franklyn,JA, Daykin, J, Drolc, Z, Farmer, M, and Sheppard, MC. Long-term follow-up of treatment of thyrotoxicosis by three different methods. Clinical endocrinology 1991; 34:71-76. [7]. Iagaru, A and McDougall, IR. Treatment of thyrotoxicosis. Journal of nuclear medicine 2007; 48:379-389. [8]. Kalinyak, JE and McDougall, IR. How should the dose of iodine-131 be determined in the treatment of Graves' hyperthyroidism?. The Journal of clinical endocrinology and metabolism 2003; 88:975-977. [9]. Yau,JS, Chu, KS, Li JK, Chan, KW, Lau, IT, Yum, SW, et al. Usage of a fixed dose of radioactive iodine for the treatment of hyperthyroidism: one-year outcome in a regional hospital in Hong Kong. Hong Kong medical journal 2009; 15:267-273. 15 16 [10]. Jarlov, AE, Hegedus, L, Kristensen, LO, Nygaard, B and Hansen, JM, et al. Is calculation of the dose in radioiodine therapy of hyperthyroidism worth while?. Clinical endocrinology 1995; 43:325-329. [11]. Allahabadia, A, Daykin, J, Holder, RL, Sheppard, MC, Gough, SC and Franklyn, JA. Age and gender predict the outcome of treatment for Graves' hyperthyroidism. The Journal of clinical endocrinology and metabolism. 2000; 85:1038-1042. [12]. Alexander, EK. and Larsen, PR. High dose of (131)I therapy for the treatment of hyperthyroidism caused by Graves' disease. The Journal of clinical endocrinology and metabolism 2002; 87:1073-1077. [13]. Neto, AM, Tambascia, MA, Brunetto, S, Ramos, CD and Zantut-Wittmann, DE. Extremely high doses of radioiodine required for treatment of Graves' hyperthyroidism: a case report. Cases journal 2009; 2:8479. [14]. Walter, MA, Christ-Crain, M, Eckard, B, Schindler, C, Nitzsche, EU, Muller-Brand, J, et al. Radioiodine therapy in hyperthyroidism: inverse correlation of pretherapeutic iodine uptake level and post-therapeutic outcome. European journal of clinical investigation 2004; 34:365-370. [15]. Clerc, J, Izembart, M, Dagousset, F, Jais, JP, Heshmati, HM, Chevalier, A, et al. Influence of dose selection on absorbed dose profiles in radioiodine treatment of diffuse toxic goiters in patients receiving or not receiving carbimazole. Journal of nuclear medicine 1993; 34:387-393. [16]. Tuttle, RM, Patience, T and Budd, S. Treatment with propylthiouracil before radioactive iodine therapy is associated with a higher treatment failure rate than therapy with radioactive iodine alone in Graves' disease. Thyroid 1995; 5:243-247. 16 17 [17]. Sabri,O, Zimny, M, Schulz, G, Schreckenberger, M, Reinartz, P, Willmes K, et al. Success rate of radioiodine therapy in Graves' disease: the influence of thyrostatic medication. The Journal of clinical endocrinology and metabolism 1999; 84:1229-1233. [18]. Imseis, RE, Vanmiddlesworth, L, Massie, JD, Bush, AJ and Vanmiddlesworth, NR. Pretreatment with propylthiouracil but not methimazole reduces the therapeutic efficacy of iodine-131 in hyperthyroidism. The Journal of clinical endocrinology and metabolism 1998; 83:685-687. [19]. Maisey, MN, Natarajan, TK, Hurley, PJ and Wagner HN, Jr. Validation of a rapid computerized method of measuring 99mTc pertechnetate uptake for routine assessment of thyroid structure and function. J Clin Endocrinol Metab 1973; 36:317-322. [20]. Martin P Sandler and William H Martin. Thyroid imaging. In: Martin P Sandler, R Edward Coleman, James A Patton, Frans JTh. Wackers and Alexander Gottschalk eds. Diagnostic nuclear medicine. Philadelphia: Lippincott Williams & Wilkins, 2003: 607-651. [21]. Wartofsky, L, Glinoer, D, Solomon, B, Nagataki, S, Lagasse, R, Nagayama, Y ,et al. Differences and similarities in the diagnosis and treatment of Graves' disease in Europe, Japan, and the United States. Thyroid 1991; 1:129-135. [22]. Hancock, LD, Tuttle, RM, LeMar, H, Bauman, J and Patience, T. The effect of propylthiouracil on subsequent radioactive iodine therapy in Graves' disease. Clinical endocrinology 1997; 47:425-430. [23]. Zantut-Wittmann, DE, Ramos, CD, Santos, AO, Lima, MM, Panzan, AD, Facuri, FV, et al. High pre-therapy [99mTc]pertechnetate thyroid uptake, thyroid size and thyrostatic drugs: predictive factors of failure in [131I]iodide therapy in Graves' disease. Nuclear medicine communications 2005; 26:957-963. 17 18 [24]. Braga, M, Walpert, N, Burch, HB, Solomon, BL and Cooper, DS. The effect of methimazole on cure rates after radioiodine treatment for Graves' hyperthyroidism: a randomized clinical trial. Thyroid 2002; 12:135-139. [25]. Andrade, VA, Gross, JL and Maia, AL. The effect of methimazole pretreatment on the efficacy of radioactive iodine therapy in Graves' hyperthyroidism: one-year follow-up of a prospective, randomized study. The Journal of clinical endocrinology and metabolism 2001; 86:3488-3493. [26]. Thientunyakit, T, Thongmak, S and Premprapha, T. Comparative evaluation of two different dosage calculation protocols of iodine-131 in the treatment of hyperthyroidism. Journal of the Medical Association of Thailand 2010; 93:969-977. [27]. Moura-Neto, A, Mosci, C, Santos, AO, Amorim, BJ, de Lima, MC, Etchebehere, EC, et al. Predictive factors of failure in a fixed 15 mCi 131I-iodide therapy for Graves' disease. Clinical nuclear medicine 2012; 37:550-554. [28]. Lal, G, Ituarte, P, Kebebew, E, Siperstein, A, Duh, QY and Clark, OH. Should total thyroidectomy become the preferred procedure for surgical management of Graves' disease?. Thyroid 2005; 15:569-574. [29]. Nordyke, RA and Gilbert FI, Jr. Optimal iodine-131 dose for eliminating hyperthyroidism in Graves' disease. Journal of nuclear medicine 1991; 32:411-416. [30]. Watson, AB, Brownlie, BE, Frampton, CM, Turner, JG and Rogers, TG. Outcome following standardized 185 MBq dose 131I therapy for Graves' disease. Clinical endocrinology 1988; 28:487-496. 18 19 [31]. Allahabadia,A, Daykin, J, Sheppard, MC, Gough, SC and Franklyn, JA. Radioiodine treatment of hyperthyroidism-prognostic factors for outcome. The Journal of clinical endocrinology and metabolism 2001; 86:3611-3617. [32]. Kung, AW, Choi, P, Lam, KS, Pun, KK, Wang, C and Yeung, RT. Discriminant factors affecting early outcome of radioiodine treatment for Graves' disease. Clinical radiology 1990; 42:52-54. [33]. Murakami, Y, Takamatsu, J, Sakane, S, Kuma, K and Ohsawa N. Changes in thyroid volume in response to radioactive iodine for Graves' hyperthyroidism correlated with activity of thyroid-stimulating antibody and treatment outcome. The Journal of clinical endocrinology and metabolism 1996; 81:3257-3260. [34]. Dige-Petersen, H, Kroon, S, Vadstrup, S, Andersen, ML, and Roy-Poulsen, NOA. A comparison of 99Tc and 123I scintigraphy in nodular thyroid disorders. European journal of nuclear medicine 1978; 3:1-4. [35]. Franklyn, JA, Daykin, J, Holder, R and Sheppard, MC. Radioiodine therapy compared in patients with toxic nodular or Graves' hyperthyroidism. QJM 1995; 88:175-180. [36]. Sankar, R, Sekhri, T, Sripathy, G, Walia, RP and Jain, SK. Radioactive iodine therapy in Graves' hyperthyroidism: a prospective study from a tertiary referral centre in north India. The Journal of the Association of Physicians of India 2005; 53:603-606. [37]. Sanyal, D, Mukhhopadhyay, P, Pandit, K, Chatterjee, J, Raychaudhuri,M, Mukherjee, S , et al. Early treatment with low fixed dose (5 mCi) radioiodine therapy is effective in Indian subjects with Graves' disease. Journal of the Indian Medical Association 2008; 106:360-361, 372. [38]. McDermott, MT, Kidd, GS, Dodson LE, Jr and Hofeldt, FD. Radioiodine-induced thyroid storm. Case report and literature review. The American Journal of Medicine 1983; 75:353-359. 19 20 [39]. Levy, WJ, Schumacher, OP and Gupta, M. Treatment of childhood Graves' disease. A review with emphasis on radioiodine treatment. Cleveland Clinic journal of medicine 1988; 55:373-382. [40]. Ponto, KA, Zang, S and Kahaly, GJ. The tale of radioiodine and Graves' orbitopathy. Thyroid 2010; 20:785-793. Figure Legend Figure 1: ROC curve for Tc 99m pertechnetate thyroid scan uptake according to response to 1st dose. 20 Response to Reviewers The reason for choose a higher dose of 12 mCi because the protocol in our institution is to give a maximum dose of 12 mCi in Graves` disease patients. Author Ethics Checklist Nuclear Medicine Communications Author Ethics Checklist Please complete this form in Word by entering information where indicated by arrowheads. Full and informative answers are needed. This document is for the editors’ quick reference; please make sure you have also included relevant information in your submitted article. Ensure document is unprotected in “Tools” in the menu bar in order to write in it. Title of paper: ►Response rate and factors affecting outcome of fixed dose of RAI 131 therapy in Graves` disease: A 10 year Egyptian experience Names of authors: ► Maha Abd Elkareem Elsayed- Wajeeh Abdulrazak Derwish and Hosna Mohamed Moustafa Office use only Sub. no.: Vol/Issue: 1. DUPLICATE PUBLICATION includes papers, or letters to the Editor previously published in this, or another journal. Abstracts of papers presented at meetings and published in the proceedings of such meetings do not constitute duplicate publication, but should be disclosed by including a note at the beginning of the paper, i.e. "Data presented previously at (state meeting) and published as abstract in (give reference)". Have you published these data previously? If so, Have you acknowledged this? ► No 2. CONFLICT OF INTEREST includes financial support from the biomedical industry or other commercial sources in the form of research grants, bench fees, consultancy or lecture fees, travelling expenses, payment of registration fees, consultancy appointments, posts held in the biomedical industry or equipment manufacturers, stock holdings in the company, free supply of drugs and the like. These should be assessed in relation to each author. If conflict of interest is present, we will publish a statement to that effect at the end of your paper, unless you have valid objections to this. Have any of the authors any conflict of interest? Please state details. ► No 3. CONSENT Please confirm that: all appropriate subjects’ consents have been obtained prior to submission of your manuscript. any information that identifies a patient has been removed from any images you have submitted. ► Yes 4. ETHICS All research studies need to be approved by the local Research Ethics Committee. Was your study? If you feel that Ethical committee approval is not required, please give reasons. ► Yes 5. AUTHORS CONTRIBUTIONS Please state briefly how each of the authors contributed to the study, to data analysis and to the writing of your paper. For a person to qualify as an author, their contribution should be sufficient for them to assume responsibility for the study. ► Dr.Wajeeh Abdulrazak, share in collecting the recorded data from thyroid clinic database. Prof Hosna Moustafe, the research was her idea, she supervise the work and review the scientific material. Dr. Maha share in collecting the recorded data, writing the review article. 6. STATISTICAL ANALYSIS Kindly please let me know who performed the statistical analysis of your data. ► Manar Mohamed Moneer, MD .Professor and Head of Biostatistics and Cancer Epidemiology. National Cancer Institute.Cairo university Other information for the Editor that may be relevant: ► None Name of person completing this form: (Please print if handwritten) ► Maha Abd Elkareem Date: ► 7-3-2014 LWW Copyright Transfer and Disclosure Form Click here to download LWW Copyright Transfer and Disclosure Form: Maha Abd Elkareem.pdf LWW Copyright Transfer and Disclosure Form Click here to download LWW Copyright Transfer and Disclosure Form: Hosna Mohamed Moustafa.pdf LWW Copyright Transfer and Disclosure Form Click here to download LWW Copyright Transfer and Disclosure Form: Wajeeh Abdulrazak Derwish.pdf Manuscript (All Manuscript Text Pages, including Title Page, References and Figure Legends) 1 Response rate and factors affecting outcome of fixed dose of RAI131 therapy in Graves` disease: A 10 year Egyptian experience Maha Abd El-Kareem M.D, Wajeeh Abdulrazak Derwish M.sc and Hosna Mohamed Moustafa M.D Department of radiotherapy and nuclear medicine (NEMROCK), Nuclear medicine unit, Cairo University. Abstract Purpose: Evaluate response and compare success rate of two different doses of I-131 therapy in treatment of Graves` disease and investigate the factors that may affect outcome. Patient and methods: Retrospective analysis was performed on 321 patients treated with I-131 for Graves` disease. Group 1 (155 patients) received 8 mCi and Group 2 (166 patients) received 12 mCi. The therapy was considered successful if euthyroidism or hypothyroidism was achieved within one year of therapy. The outcome was compared with multiple parameters. Results: Significant difference in the outcome between the two groups was found in favor of the second group (P<0.001). Logistic regression analysis revealed that lower dose, Tc99 pertechnetate thyroid uptake > 20.9 %, moderate and marked goiter were independent variables that significantly associated with less response rate (OR 2.601, 4.023 and 3.309 respectively), while prior surgical treatment with higher response rate (OR 3.071). No correlation between outcome and age, presence of exopthalomos, previous treatment with 1 2 methimazole and its duration was found. Response rate to the second dose was significantly increased compared to the first one by 27.8 %, there was no correlation among the above mentioned factors and its outcome. The third dose controlled 81.3 % of the remaining patients and the rest were achieved controlled after the fourth dose. Conclusions: I-131 is very effective therapy for Graves` disease with cure rate 100% after 4 doses. Higher first dose activity is recommended in the presence of poor prognostic factors. Second dose is not necessary increased in the non responders. Keywords: Graves` disease; radioactive iodine therapy; fixed dose- Tc-99 pertechnetate thyroid uptake. Introduction: Graves` disease (GD) is the most common cause of hyperthyroidism responsible for approximately 50-60% of the cases (1). The most common clinical presentations related to the cardiovascular system. Other disease manifestations include Graves’ ophthalmopathy and myxedema(2). Diagnostic modalities include suppressed serum TSH and an elevated serum FT4, FT3 levels, thyroid scintigraphy either with Tc99m pertechnetate or radioactive iodine-131 (RAI-131) and ultrasonography (U.S) to detect the presence of an associated nodules (3). Three therapeutic modalities are commonly used today; anti-thyroid drugs (ATDs), RAI-131 and surgical treatment (3). The aim of RAI -131 treatment is to cure the hyperthyroidism by rendering the patient either euthyroid or hypothyroid through destruction of the over-functioning thyroid tissues (4). The use of RAI-131 in treatment of GD is increasing, particularly as a first line treatment (5) as it is easy to administer, relatively inexpensive, reliable , safe and highly effective with a cure rate approaching 100% after one or more dose (6) . Different 2 3 methods have been used for determining the administered activity, varied from fixed doses to adjusted calculations based on gland size, iodine uptake and turnover (7). The dose calculation method aims to optimize the therapeutic results through administration of radioactive iodine in proportional to the size of the gland, increasing the probability of cure and providing the lowest possible radiation dose to the rest of the body (8). There is little evidence that using a calculated dose has any advantage over a fixed-dose regimen in preventing hypothyroidism or improvement in cure rate (9), but it increases significantly the cost of the therapy owing to increase the procedure complexity (10). Taking in mind that the radioactive iodine therapy is relatively inexpensive, thus the increase in its cost to determine the administered activity must be clearly justified (10). There are some predictive factors associated with RAI-131 success rate. Previous works have shown lower treatment success rates in young male patients, more severe cases of hyperthyroidism (11)(12) , larger goiters (12) (13) and in cases with low or high pretreatment thyroid uptake (12) (14). The influence of pretreatment with anti-thyroid drugs on the efficacy of radioiodine therapy is controversial. Some authors believe that the thyrostatic drugs methimazole (MMI) and propylthiouracil (PTU) have a radioresistance effect and can lead to half-life reduction and accelerate turnover (15) (16) (17), but others have shown an effect confined to PTU only (18). Patients and Methods: We retrospectively evaluated 321 hyperthyroid patients due to GD referred to the nuclear medicine unit, Kasr Al ainy hospital (NEMROK), Cairo University, during the period of January 2000 till January 2010 for RAI-131 therapy as first or as a second treatment modality (following medical or surgical treatment). Our 3 4 institutional medical ethics committee approved the protocol. The diagnosis of GD was primarily based on clinical (hyperthyroid manifestations and diffusely enlarged thyroid gland) and laboratory data, including high serum free T4 level (FT4; reference Values, RV = 0.9 - 1.8 ng/dL) and low serum thyrotropin levels (TSH; RV = 0.41- 4.5 µ IU/mL). The patients who had thyrotoxicosis due to toxic multi-nodular goiter (Plummer disease), toxic autonomous adenoma, GD associated with (cold) nodule by (scan) or palpation respectively and patients who not completed the follow up were excluded from the study. Data were retrieved from the thyroid clinic database include: age at diagnosis, gender, symptoms, dose and duration of anti-thyroid drugs , previous surgical treatment, clinical data for the presence of palpable nodules & other neck swellings and the presence or absence of eye signs, TSH level and thyroid scan using Tc-99m pertechnetate that was done 20 min after intravenous injection of 5 mCi of the tracer to evaluate the associated nonfunctioning (cold) nodule and quantitation of thyroid uptake using the methodology previously described by Maisey et al(19) and simplified for routine use. The reference values for Tc-99m pertechnetate uptake range from 0.3 to 4 % (20). Gland size were determined by combining clinical examination (palpation) and thyroid scan and was divided in to either normal size (impalpable), mild (palpably enlarged but not visible) and moderate or markedly enlargement (palpable and visible goiter). In view of our socioeconomical circumstances; the simple fixed dose protocol has considerable cost saving advantages, we have adopted this protocol for the treatment of GD in our institution. The patients were divided according to the given RAI-131 dose in to 2 groups: Group 1: 4 5 received 8 mCi (155 patients) (48.3%) and Group 2: received 12 mCi (166 patients) (51.7%), they are the commonly preferred doses in the treatment of GD in our institute. Anti-thyroid drugs, if given before therapy, were withdrawn a week before therapy and for a minimum of 1 week after to avoid any drug influence on the therapeutic effectiveness. Iodine-containing medications were also discontinued several weeks before therapy; in addition, the patients were started on a low-iodine diet for 10 days before therapy, fasted before and for 2 hours after the administration of the dose to achieve higher absorption. Patients were advised to avoid physical contact and transfer of secretions to others for several days after treatment. Regular clinical and laboratory follow up to evaluate therapeutic efficacy was done and the patients were classified according to the outcome in to: Euthyroidism: Absence of signs or symptoms of hyperthyroidism or hypothyroidism with normal serum TSH value without levothyroxin therapy. Resistant to therapy: persistence of thyrotoxic manifestation and suppressed TSH value or by requirement of repeat administration of RAI-131 therapy within 6 months of the therapy and Hypothyroidism: presence of symptoms or signs of hypothyroidism together with elevated TSH value on two occasions four weeks apart, that require permanent treatment with levothyroxine. RAI-131 treatment was considered to be successful if the patient was either euthyroid or hypothyroid. Statistical methods: Data was analyzed using IBM SPSS advanced statistics version 20 (SPSS Inc., Chicago, IL). Numerical data were expressed as mean and standard deviation or median and range as appropriate. Qualitative data were expressed as frequency and percentage. Chi-square test (Fisher’s exact test) was used to examine the relation between 5 6 qualitative variables. For quantitative data, comparison between two groups was done using Mann-Whitney test (non-parametric t-test). The receiver operator characteristic (ROC) curve was used to identify the best threshold for thyroid uptake to discriminate success and failure of RAI-131 therapy. Multivariate analysis was done using forward stepwise logistic regression method for the significant factors affecting response on univariate analysis. Odds ratio (OR) with 95% confidence interval (CI) were used for risk estimation. P-value < 0.05 was considered significant. Results:. Baseline, pre-therapy clinical characteristics and commonly presenting symptoms for the patients are listed in Table 1 and 2. The recorded data documented development of early complications within the 1st 3 months in 31 patients (9.6%), included transient mild increased thyrotoxic manifestations in 21 patients and transient hypothyroidism which occurred for 8 patients, 5 after a high dose and 3 after low dose. Six of the 8 patients developed transient hypothyroidism after 1st dose, while the remaining 2 patients developed it after 2nd dose. Also neck pain developed in 2 patients. There was statistically significant difference in the incidence of early complications between the patients who received 8 mCi and the second group who received 12 mCi, in favor of the latter group (p = 0.024), whereas as there was no statistically significant difference between age, gender, presence of exopthaloms, size of thyroid gland and thyroid uptake and early complications either between the two groups as shown in the table (3) or in each group separately (not included). Exopthalmos was increased in 9 patients (9.6%) after RAI-131 therapy and remained stationary in rest. Three new cases (1.3%) developed exophthalmos from the remaining 6 7 227 patients and they were among the 170 patients who had permanent hypothyroidism (1.7%). No relation was found between the presence of exopthalmos and development of early complications as shown in tables 3. The success rate to the first given dose was 59.8% with development of euthyroidism in 56 patients (17.4%) and hypothyroidism in 136 patients (42.4%). There was statistically significant difference in the successes rate between the patients who received 8 mCi (49%) and 12 mCi (69.9%) P <0.001. Of the 76 patients in whom therapy was successful in group1, 25 (16.1%) developed euthyroidism and 51(32.9 %) developed hypothyroidism and at a median period of 6 months (range: 3 –18 months) and among the 116 responding patients in the second group, euthyroidism was achieved in 37 patients (22.3%) and hypothyroidism in 79 patients (47.6%) with a median cure time 4 months (range: 2 –18 months). There was no statistically significant association between age, presence of ophthalmopathy and previous medical treatment & its duration and outcome, whereas there was statistically significant difference regarding gender, size of thyroid gland, Tc99m pertechnetate thyroid uptake and previous surgical treatment as demonstrated in table 4. We did not find any relationship between the previous use of methimazole & its duration and the outcome of patients either in the whole study population or G1 and G2 separately (tables 4 and 5 A&B). Thyroid uptake was analyzed using ROC curve to discriminate the group of patients who achieved success with treatment from the group that remained hyperthyroid and we found a thyroid uptake threshold of 20.9 % with a sensitivity of 76.1 % and specificity of 65.4 7 8 % for treatment success (Fig. 1). We were unable to find an adequate cutoff value for base line TSH level. Multiple logistic regression analysis demonstrated that age, gender and previous medical treatment were not significantly associated with the outcome, whereas Tc99m pertechnetate thyroid uptake > 20.9% (OR= 4.023) , moderate and markedly enlarged thyroid gland (OR= 3.309) and the low given dose (OR= 2.601) were identified as significant prognostic risk factors for treatment failure and previous thyroidectomy for treatment success (OR= 3.071) (odds ratio; 95% confidence interval = 2.218 -7.297, 1.707 - 6.414, 1.403 - 4.822 and 1.109 - 8.502 respectively). Response to the second dose: A second dose was given to the 129 non responded patients after a mean time of 6.77 months (minimum 3 months and maximum 12 months). Of these 63 patients received 8 mCi and 66 received 12 mCi. The overall response rate to the second therapy dose significantly increased compared to the first one by 27.8 % with development of euthyroidism in 56 patients (17.4%) and hypothyroidism in 136 patients (42.4%). There was no statistically significant difference in the response rate between the patients who received 8 mCi and who received 12 mCi (P value = 0.921), also there was no statistically significant difference in the response rate in relation to size of thyroid gland, Tc99m pertechnetate thyroid uptake, previous surgical treatment, age and gender (p values 0.265, 0.665, 0.242, 0.209 and 0.923 respectively) as shown in table 6. Fifty two patients from the 79 non responded in the first group received second dose of 8 mCi while the remaining 27 patients received 12 mCi. 8 There was no statistically 9 significant difference in the response rate between the patients received 8 mCi (86%) and 12 mCi (92.6 %) with P value = 0.422. No statistically significant difference in the response rate in relation to size of thyroid gland, Tc-99m pertechnetate thyroid uptake and previous surgical treatment was found (p values = 0.436, 0.225 and 0.361 respectively). Eleven from the 50 non responded patients in the second group were received second dose 8 mCi while the other 39 patients received 12 mCi. There was no statistically significant difference in the response rate between the patients received 8 mCi (90.9 %) and 12 mCi (384.6 %) with P value = 0.595 and no statistically significant difference in the response rate in relation to size of thyroid gland, Tc99m pertechnetate thyroid uptake and previous surgical treatment (p values = 0.418, 0.117 and 0.471 respectively). Thirteen patients from the remaining 16 non responders to the second dose responded to the 3rd RAI-131 dose with development of euthyroidism in 7 patients (43.8 %) and hypothyroidism in the remaining 6 patients (37.5%). The 4th dose controlled the remaining 3 patients with development of hypothyroidism in 2 patients and euthyroidism in the third. The median dose for controlling GD was 12 mCi (minimum 8 mCi which controlled 23.7% of the patients and maximum 47 mCi), the doses of 12 mCi, 16 mCi, 20 mCi, 24 mCi, 28 mCi, 32 mCi, 36 mCi, 43 mCi and 47 mCi increase the overall control rate to 59.8 %, 74.1%, 85%, 96%, 96.9%, 97.8%, 99.4%, 99.7% and 100% respectively as shown in table 7. The mean dose number for controlling the hyperthyroidism was 1.46 ± 0.62 (range 1- 4). The first dose controlled 59.8% of the patients, this percent increased to 95% after the second dose, 99.1% following the third one and 100% after the fourth dose 9 10 as shown in table 8. Discussion: About 80% of experts from Europe preferred to start treatment with ATDs in patients over 21 years and 70% of those in the United States RAI is the initial treatment modality of choice (21). In Egypt the ATDs represent, for most endocrinologists, the initial choice of treatment. This trend was reflected in the present study, where only 22.4% of the patients underwent RAI as initial treatment modality, while 77.6% patients were previously treated with ATDs. The influence of ATDs on the outcome of RAI treatment has received attention. Some studies have suggested that ATD treatment before or after RAI may provide a radioprotective effect for the thyroid with significantly shortened the biological half-life of RAI result in reduction of the absorbed dose and increased failure rate of single-dose RAI treatment (16-17) (22). Thionamide withdrawal was among the predictive factors for treatment success in a 10-mCi fixed-dose approach (23). More over Alexander et al. treated 261 Graves’ patients with a mean dose of 14.6 mCi of RAI demonstrated high risk of treatment failure in patients pretreated with anti-thyroid medications for greater than 4 months(12). Other studies stated that this effect confined to the use of propylthiouracil only (18). In contrast Braga et al. (24) and Andrade et al. (25) demonstrated that methimazole pretreatment has no effect on the final treatment result, including the time required for cure or the 1-year success rate of RAI therapy. Thientunyakit T et al. (26) showed that duration of anti-thyroid drug given prior to radioiodine therapy seemed not related to the treatment outcome. Moura-Neto also found that no statistically significant association between thyroid function outcome to a fixed, 10 11 15 mCi approach for treatment of Graves’ hyperthyroidism and drug used (methi-mazole or propylthiouracil; maintenance or withdrawal of thionamides prior to therapy (27). Our results were in agreement with the later ones, where we don’t find statistical significant difference between pre-iodine medical treatment or its duration and the outcome to RAI131 therapy. Surgery is no longer recommended as first-line therapy for GD and use in selective cases where RAI is not preferred and ATDs fail to control the disease(3). Lal et al. concluded that total thyroidectomy (TT) is much better than Subtotal thyroidectomy (STT) (28). In the present study, STT was performed in only 49 patients (15.3%) with recurrent of disease in all of them at a median period of 66 months, confirming the literature data of using it as an alternative option in selected patients. The size of thyroid gland is an important factor influencing the outcome of therapy; In our study, mildly enlarged glands had more controlled rate than moderate or markedly enlarged thyroid gland with higher incidence of hypothyroidism ( P = 0.042). This result is in agreement with the other multiple studies which have demonstrated that patients with larger-volume thyroid glands to fail to respond to a single dose of radioiodine (2327-29-30-31-32). The impact of thyroid uptake on the RAI outcome has been investigated using either 131I or Tc99m pertechnetate. Alexander et al (12) found that patients who have higher 24hour thyroid RAI uptake values were at higher risk than others for treatment failure. Kung et al. (32) also identified 4-hour RAI uptake among the variables that could predict early treatment outcome for Graves’ disease. These results were in agreement with other 11 12 works demonstrating higher failure rates in patients with higher iodide thyroid uptake values which could reflect faster iodide turnover in thyroid cells thus making the residence time of therapeutic I-131 in the gland shorter (33). The authors suggested that a higher radioactivity of RAI be given to these patients. Using Tc99-m sodium pertechnetate Zantut-Wittmann et al. (23) have reported that in a 10 mCi fixed dose approach the pre-RIT Tc99-m sodium pertechnetate uptake under 12% among the predictive factors for treatment success. In contrast, Moura-Neto et al. stated that no statistically significant association between thyroid function outcome to a fixed 15 mCi approach for treatment of GD and Tc-99m sodium pertechnetate thyroid uptake prior to therapy(27). Tc-99 m pertechnetate uptake is routinely used in our department as a surrogate measure of thyroid uptake because it has been proved to possess a good correlation with iodide 125 uptake (34). Moreover, it is much less expensive, reliable and convenient method allows uptake within 20 minutes after intravenous injection of the radionuclide and the therapeutic dose of RAI can be administered immediately after. We found that Tc-99m pertechnetate thyroid uptake more than 20.9% was among the poor prognostic factors for the response, thus higher dose is recommended. The different RAI doses have different impact on the thyroid gland function, less than half of the patients (49%) in group 1 who received low dose of RAI achieved cure. On the other hand 69.4 % from the second group, who received higher dose of RAI, had achieved cure. This means that higher dose of RAI increase response rate by ~ 20.4 %. Franklyn et al.(35) and Sankar et al.(36) studied the therapeutic outcome of low fixed dose of RAI, the former concluded that persistent hyperthyroidism after 6 months was 12 13 present in 55.9% of the patients using small fixed dose of 5 mCi of RAI and the latter recommended increase dose of RAI to achieve response. This agree with Nordyke and Gilbert (29) who analyzed a series of 605 patients treated with RAI to find out the optimal dose to achieve cure and they concluded that cure was directly related to the dose of RAI administered and the optimal dose for curing hyperthyroidism is approximated by starting with 10 mCi and increasing it for unusually large glands or for special patient circumstances. In the present study, 88% of patients achieved cure after administration of second dose of RAI with no statistically significant difference was found between the success rate and the given dose, only few patients require 3rd or 4th doses. This is in concordant with Sanyal et al. (37) and Franklyn et al. (35) studies that demonstrated high cure rate to the second dose of RAI ( 82.4% and 74.5% respectively) with only few require other doses. Although it is very rare, McDermott et al.(38) reported thyroid storm in a small number of patients between 1 and 14 days after treatment with RAI. In the present study thyroid storm did not encountered in any patient. Also, Levy et al.(39) in a series of 7000 patients treated with RAI in one centre, none developed this complication. Ponto et al. (40) concluded that RAI therapy for GD is associated with definite increased risk of GO in around 20% of patients (either developing new cases or worsening of preexisting one). However In the present work there was worsening of exophtalmus in 9.6 % of the patients and three new cases were developed (1.3%) among the rest who did not have 13 14 prior exopthalmos, they were among the 177 patients who developed permanent hypothyroidism. Conclusion: Radioiodine is clearly successful in curing hyperthyroidism in GD patients by 100 % after 4 doses; therefore it should be used as a first standard line in treatment. Treatment results using fixed RAI dose are comparable to those studies of patients treated with RAI using the prescribed absorbed dose method. The standard-dose prescription strategy is therefore an efficient, cost-effective and is also convenient to the patient. It may be possible to improve cure rates using a single fixed-dose regimen without increasing the dose in all patients. This might be achieved by the identification of subjects with poor prognostic factors who are unlikely to respond to standard doses and by administering larger doses only to these individuals. A higher fixed (12 mCi) is more effective than lower dose (8 mCi) for treatment of GD leading to better control of the disease following the first dose. Higher response rate are expected in patients who underwent previous surgery, on contrary patients with larger goiters and high thyroid uptake > 20.9% had 3.3 and 4 times less chance of remission. This different impact of different doses on the response rate is applied to the first dose, but not to the second dose where the response rate to the second dose is nearly similar in both low and high dose groups. References: [1]. McKenzie, J M, Zakarija, M and Sato, A. Humoral immunity in Graves' disease. Clinics in endocrinology and metabolism 1978; 7:31-45. 14 15 [2]. Reid, JR and Wheeler, SF. Hyperthyroidism: diagnosis and treatment. American family physician 2005; 72:623-630. [3]. Bahn, RS, Burch, HB, Cooper, DS, Garber, JR, Greenlee, MC, Klein, I, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists Endocrine practice 2011; 17:456-520. [4]. Isgoren, S, Daglioz Gorur, G, Demir, H, and Berk, F. Radioiodine therapy in Graves' disease: is it possible to predict outcome before therapy?. Nuclear medicine communications 2012; 33:859-863. [5]. Hedley, AJ, Lazarus, JH, McGhee, SM, Jones, RB, Sharp, PF, Naven, LM, et al.. Treatment of hyperthyroidism by radioactive iodine. Summary of a UK national survey prepared for the Royal College of Physicians Committee on Endocrinology and Diabetes. Journal of the Royal College of Physicians of London 1992; 26:348-351. [6]. Franklyn,JA, Daykin, J, Drolc, Z, Farmer, M, and Sheppard, MC. Long-term follow-up of treatment of thyrotoxicosis by three different methods. Clinical endocrinology 1991; 34:71-76. [7]. Iagaru, A and McDougall, IR. Treatment of thyrotoxicosis. Journal of nuclear medicine 2007; 48:379-389. [8]. Kalinyak, JE and McDougall, IR. How should the dose of iodine-131 be determined in the treatment of Graves' hyperthyroidism?. The Journal of clinical endocrinology and metabolism 2003; 88:975-977. [9]. Yau,JS, Chu, KS, Li JK, Chan, KW, Lau, IT, Yum, SW, et al. Usage of a fixed dose of radioactive iodine for the treatment of hyperthyroidism: one-year outcome in a regional hospital in Hong Kong. Hong Kong medical journal 2009; 15:267-273. 15 16 [10]. Jarlov, AE, Hegedus, L, Kristensen, LO, Nygaard, B and Hansen, JM, et al. Is calculation of the dose in radioiodine therapy of hyperthyroidism worth while?. Clinical endocrinology 1995; 43:325-329. [11]. Allahabadia, A, Daykin, J, Holder, RL, Sheppard, MC, Gough, SC and Franklyn, JA. Age and gender predict the outcome of treatment for Graves' hyperthyroidism. The Journal of clinical endocrinology and metabolism. 2000; 85:1038-1042. [12]. Alexander, EK. and Larsen, PR. High dose of (131)I therapy for the treatment of hyperthyroidism caused by Graves' disease. The Journal of clinical endocrinology and metabolism 2002; 87:1073-1077. [13]. Neto, AM, Tambascia, MA, Brunetto, S, Ramos, CD and Zantut-Wittmann, DE. Extremely high doses of radioiodine required for treatment of Graves' hyperthyroidism: a case report. Cases journal 2009; 2:8479. [14]. Walter, MA, Christ-Crain, M, Eckard, B, Schindler, C, Nitzsche, EU, Muller-Brand, J, et al. Radioiodine therapy in hyperthyroidism: inverse correlation of pretherapeutic iodine uptake level and post-therapeutic outcome. European journal of clinical investigation 2004; 34:365-370. [15]. Clerc, J, Izembart, M, Dagousset, F, Jais, JP, Heshmati, HM, Chevalier, A, et al. Influence of dose selection on absorbed dose profiles in radioiodine treatment of diffuse toxic goiters in patients receiving or not receiving carbimazole. Journal of nuclear medicine 1993; 34:387-393. [16]. Tuttle, RM, Patience, T and Budd, S. Treatment with propylthiouracil before radioactive iodine therapy is associated with a higher treatment failure rate than therapy with radioactive iodine alone in Graves' disease. Thyroid 1995; 5:243-247. 16 17 [17]. Sabri,O, Zimny, M, Schulz, G, Schreckenberger, M, Reinartz, P, Willmes K, et al. Success rate of radioiodine therapy in Graves' disease: the influence of thyrostatic medication. The Journal of clinical endocrinology and metabolism 1999; 84:1229-1233. [18]. Imseis, RE, Vanmiddlesworth, L, Massie, JD, Bush, AJ and Vanmiddlesworth, NR. Pretreatment with propylthiouracil but not methimazole reduces the therapeutic efficacy of iodine-131 in hyperthyroidism. The Journal of clinical endocrinology and metabolism 1998; 83:685-687. [19]. Maisey, MN, Natarajan, TK, Hurley, PJ and Wagner HN, Jr. Validation of a rapid computerized method of measuring 99mTc pertechnetate uptake for routine assessment of thyroid structure and function. J Clin Endocrinol Metab 1973; 36:317-322. [20]. Martin P Sandler and William H Martin. Thyroid imaging. In: Martin P Sandler, R Edward Coleman, James A Patton, Frans JTh. Wackers and Alexander Gottschalk eds. Diagnostic nuclear medicine. Philadelphia: Lippincott Williams & Wilkins, 2003: 607-651. [21]. Wartofsky, L, Glinoer, D, Solomon, B, Nagataki, S, Lagasse, R, Nagayama, Y ,et al. Differences and similarities in the diagnosis and treatment of Graves' disease in Europe, Japan, and the United States. Thyroid 1991; 1:129-135. [22]. Hancock, LD, Tuttle, RM, LeMar, H, Bauman, J and Patience, T. The effect of propylthiouracil on subsequent radioactive iodine therapy in Graves' disease. Clinical endocrinology 1997; 47:425-430. [23]. Zantut-Wittmann, DE, Ramos, CD, Santos, AO, Lima, MM, Panzan, AD, Facuri, FV, et al. High pre-therapy [99mTc]pertechnetate thyroid uptake, thyroid size and thyrostatic drugs: predictive factors of failure in [131I]iodide therapy in Graves' disease. Nuclear medicine communications 2005; 26:957-963. 17 18 [24]. Braga, M, Walpert, N, Burch, HB, Solomon, BL and Cooper, DS. The effect of methimazole on cure rates after radioiodine treatment for Graves' hyperthyroidism: a randomized clinical trial. Thyroid 2002; 12:135-139. [25]. Andrade, VA, Gross, JL and Maia, AL. The effect of methimazole pretreatment on the efficacy of radioactive iodine therapy in Graves' hyperthyroidism: one-year follow-up of a prospective, randomized study. The Journal of clinical endocrinology and metabolism 2001; 86:3488-3493. [26]. Thientunyakit, T, Thongmak, S and Premprapha, T. Comparative evaluation of two different dosage calculation protocols of iodine-131 in the treatment of hyperthyroidism. Journal of the Medical Association of Thailand 2010; 93:969-977. [27]. Moura-Neto, A, Mosci, C, Santos, AO, Amorim, BJ, de Lima, MC, Etchebehere, EC, et al. Predictive factors of failure in a fixed 15 mCi 131I-iodide therapy for Graves' disease. Clinical nuclear medicine 2012; 37:550-554. [28]. Lal, G, Ituarte, P, Kebebew, E, Siperstein, A, Duh, QY and Clark, OH. Should total thyroidectomy become the preferred procedure for surgical management of Graves' disease?. Thyroid 2005; 15:569-574. [29]. Nordyke, RA and Gilbert FI, Jr. Optimal iodine-131 dose for eliminating hyperthyroidism in Graves' disease. Journal of nuclear medicine 1991; 32:411-416. [30]. Watson, AB, Brownlie, BE, Frampton, CM, Turner, JG and Rogers, TG. Outcome following standardized 185 MBq dose 131I therapy for Graves' disease. Clinical endocrinology 1988; 28:487-496. 18 19 [31]. Allahabadia,A, Daykin, J, Sheppard, MC, Gough, SC and Franklyn, JA. Radioiodine treatment of hyperthyroidism-prognostic factors for outcome. The Journal of clinical endocrinology and metabolism 2001; 86:3611-3617. [32]. Kung, AW, Choi, P, Lam, KS, Pun, KK, Wang, C and Yeung, RT. Discriminant factors affecting early outcome of radioiodine treatment for Graves' disease. Clinical radiology 1990; 42:52-54. [33]. Murakami, Y, Takamatsu, J, Sakane, S, Kuma, K and Ohsawa N. Changes in thyroid volume in response to radioactive iodine for Graves' hyperthyroidism correlated with activity of thyroid-stimulating antibody and treatment outcome. The Journal of clinical endocrinology and metabolism 1996; 81:3257-3260. [34]. Dige-Petersen, H, Kroon, S, Vadstrup, S, Andersen, ML, and Roy-Poulsen, NOA. A comparison of 99Tc and 123I scintigraphy in nodular thyroid disorders. European journal of nuclear medicine 1978; 3:1-4. [35]. Franklyn, JA, Daykin, J, Holder, R and Sheppard, MC. Radioiodine therapy compared in patients with toxic nodular or Graves' hyperthyroidism. QJM 1995; 88:175-180. [36]. Sankar, R, Sekhri, T, Sripathy, G, Walia, RP and Jain, SK. Radioactive iodine therapy in Graves' hyperthyroidism: a prospective study from a tertiary referral centre in north India. The Journal of the Association of Physicians of India 2005; 53:603-606. [37]. Sanyal, D, Mukhhopadhyay, P, Pandit, K, Chatterjee, J, Raychaudhuri,M, Mukherjee, S , et al. Early treatment with low fixed dose (5 mCi) radioiodine therapy is effective in Indian subjects with Graves' disease. Journal of the Indian Medical Association 2008; 106:360-361, 372. [38]. McDermott, MT, Kidd, GS, Dodson LE, Jr and Hofeldt, FD. Radioiodine-induced thyroid storm. Case report and literature review. The American Journal of Medicine 1983; 75:353-359. 19 20 [39]. Levy, WJ, Schumacher, OP and Gupta, M. Treatment of childhood Graves' disease. A review with emphasis on radioiodine treatment. Cleveland Clinic journal of medicine 1988; 55:373-382. [40]. Ponto, KA, Zang, S and Kahaly, GJ. The tale of radioiodine and Graves' orbitopathy. Thyroid 2010; 20:785-793. Figure Legend Figure 1: ROC curve for Tc 99m pertechnetate thyroid scan uptake according to response to 1st dose. 20