Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
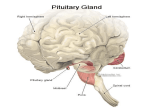
BHS 116.2 – Physiology Notetaker: Vivien Yip Date: 2/6/2013, 1st hour Page1 Final Exam Review **Not inclusive, anything covered during the quarter may appear on the exam 65- 66 Questions (New) GI/liver material will make up 2/3 of exam Chemical structure of hormones - Proteins, peptides - Steroids - Tyrosine derivatives - Signaling and target cells - Plasma receptors - Signalling cascades lead to end result - Cyclic amp cascade - Gq phospholipase C cascade - Steroid hormone and thyroid hormone o Lipid soluble can directly diffuse to target cell o Bind nuclear receptor o Sometimes cytoplasmic receptor o Hormone receptor complex that activates transcription Anterior pituitary hormones - Not tropic - What they are - What they do - All of them are tropic except prolactin - Stimulate targets to secrete another hormone - Prolactin is the only one that does not do that Hypothalamic hypophyseal portal system - Anterior pituitary secretion relies on releasing factors/inhibiting factors released from hypothalamus - Stimulate or inhibit anterior pituitary cell to secrete their hormones Regulation of anterior pituitary hormone secretion - Negative feedback from the end hormone back onto the anterior pituitary and or the hypothalamus to inhibit secretion - Final hormone will have its own target - Once there is enough of target hormone in the blood, no need for anterior pituitary or hypothalamic hormone to continue secretion - Rarely will see anterior pituitary hormone - Only the target that is involved in negative feedback process Main stimuli: GH - Stimulating and inhibiting factor released by hypothalamus - Inhibitory: somatostatin - Stimulatory: GHRH - Depending on which factor is released, will get stimulation or inhibition of GH release - GH has different effects on target o Metabolic Triggered by GH itself o Growth promoting actions Carried by IGF 1 GH stimulate liver to secrete IGF1 IGF trigger growth in target tissue Posterior Pituitary - 2 hormones released BHS 116.2 – Physiology Notetaker: Vivien Yip - - Date: 2/6/2013, 1st hour Page2 Produced in the hypothalamus o ADH/vasopressin o Oxytocin No hypophyseal portal system Axons of neurons that travel through pituitary stalk and release hormone in the posterior pituitary gland Pathologies - Pituitary adenoma (anterior pituitary) o Visual system symptoms are due to compression of nerves o Bitemporal hemianopsia (optic chiasm is compressed) o Optic atrophy (compression of chiasm lasts a long time will stop blood supply) o Lateral growth (into cavernous sinus) will compress cranial nerves that supply the EOMs diplopia o Hormonal symptoms: whichever cell type is oversecreting - Diabetes insipidus (posterior pituitary) o Excess urination due to excess water in the body o Hypothalamic or posterior pituitary damage o Decreased or no ADH secretion o Body is unable to reabsorb the water from renal tubules Thyroid Hormone Synthesis - Requires iodine - T3 and T4 are the primary thyroid hormones - T4 is most abundant - T3 is most active and efficient at stimulating activity TH Secretion - Primary action on target is to increase metabolism - Increase metabolic rate - Permissive action: increases ability of other hormones to work (sympathetic nervous system) o Increase/enhance sympathetics Hyperthyroidism - Thyrotoxicosis – excess thyroid hormone o Negative feedback leads to very small amounts of TSH o Elevated T3 and T4 Graves Disease - Most common of hyperthyroidism - Autoimmune disease - Antibodies stimulate the TSH receptor - TSH receptor is constantly stimulated o TSI o TBII o TGI Thyroid Adenoma - NOT autoimmune disease - Secretory function of the rest of the normal thyroid gland is shut down - Decreased TSH - Cancerous part of gland hypersecretes thyroid hormone - Genetic analysis indicates mutation in TSH receptor (as if constantly active) Hypothyroidism - Hashimoto thyroiditis - Decreased thyroid hormone secretion BHS 116.2 – Physiology Notetaker: Vivien Yip - Date: 2/6/2013, 1st hour Page3 Autoimmune disease that destroys the gland itself TSH levels are high Lack of negative feedback Goiters - Endemic goiter pathology o Due to iodine deficiency o Elevated levels of TSH o Unable to produce mature thyroid hormone - Idiopathic nontoxic goiter pathology o Normal iodine levels o Mild thyroiditis o Abnormal thyroid enzyme systems Adrenal Cortex - Mineralocorticoids o Zona glomerulosa o Aldosterone o Major regulator in electrolyte and water balance - Glucocorticoids o Cortisol o Zona fasiculata o Role in CHO, fat and PRO metabolism - Androgens Aldosterone - Increases renal K+ secretion - Increase renal reabsorption of Na+ o Increase in H2O retention - Net effect is to increase the total amount of Na+ and decrease K+ in the ECF and to increase ECF volume o Important in long term maintenance of blood pressure Cortisol - Released in response to mental or physical stress - Transmit signals to hypothalamus o Release CRH - Stimulates anterior pituitary o Release ACTH - Stimulates cortisol release from adrenal cortex - Increase blood glucose o At the expense of protein and fat stores - Enough glucose for brain and skeletal muscles o Triggers insulin resistance in other tissues - Elevated amino acids and fats as well Adrenal medulla - Modified part of sympathetic nervous system - Release catecholamines: epinephrine (adrenaline) and norepinephrine o Both are tyrosine derivatives Calcium Absorption - Body keeps a tight regulation on the ECF concentration of Ca2+ - Slight changes can induce a large change in the body - Calcium intake from diet will make its way out of the body at some point - If not enough coming from diet, bone will be major source of calcium BHS 116.2 – Physiology Notetaker: Vivien Yip Date: 2/6/2013, 1st hour Page4 Vitamin D - Formed in the skin - Natural precursor with the help of sunlight - Absorbed mostly through diet - Required to absorb calcium from digestive system o Need active Vit D3 to do this - Add 1 hydroxyl group in the liver o Requires PTH (major) or decreased phosphate levels in blood to trigger 2 nd hydroxyl reaction in the kidney o Now get active form of Vit D3 o That can now stimulate absorption of calcium and phosphate from GI tract Parathyroid hormone (PTH) - Acute and chronic effects - Primary job is to raise plasma calcium levels - Acute form o Stimulate osteocytes and osteoblasts o Remove calcium from the amorphous pool of calcium salts o Short term elevation of PTH response - Chronic o PTH always present o Osteoclasts are activated o Break down mineralized bone o Release both calcium and phosphate into the blood Bone production and calcification - Amorphous pool (first source for calcium) - If chronic effects, o Break down bone by activating osteoclasts PTH effects on ECF concentration of Ca2+ and PO4- Trigger kidneys to excrete phosphate - Decrease plasma levels of phosphate - PTH also stimulates kidneys to reabsorb calcium - Increase plasma concentration of calcium Regulation of plasma Ca++ by Vitamin D & PTH - Increase dietary uptake of calcium - Increase renal tubule reabsorption of calcium - Stimulate bone to mobilize calcium - Act on bone and kidneys directly - Indirect action on intestines through Vit D Negative feedback with PTH and calcitonin secretion - Elevated calcium levels trigger calcitonin - Decrease calcium levels back to normal is the goal of calcitonin Osteoporosis - Occurs naturally w/ age - Decreased mineralization - Senile osteoporosis o Reduced bone formation o Reduced osteoblast activity - Postmenopausal o More severe o Decreased osteoblast activity and bone formation o Increased osteoclast activity and bone resorption BHS 116.2 – Physiology Notetaker: Vivien Yip Date: 2/6/2013, 1st hour Page5 Addison Disease - Hypoadrenalism o Affect aldosterone and cortisol levels - Primary adrenal insffucieicny o Autoimmune adrenalitis o Infections o Metastatic neoplasms Cushing Syndrome - Hypercortisolism - 4 causes: pituitary cushing, adrenal cushing, paraneoplastic cushing, iatrogenic cushing (most common cause) Hypothyroidism - Not very common - Parathyroid gland does not secrete sufficient PTH - Hypocalcemia - Not triggering the kidneys to resorb more calcium Primary hyperparathyroidism - Hypercalcemia - Hypersecretion of PTH Secondary hyperparathyroidism - Vit D deficiency - Renal disease o Cause hypocalcemia o Constantly stimulating parathyroid gland Pancreas - Alpha cells o Glucagon - Beta cells o Insulin Insulin Receptor - Once bound, becomes an active enzyme - Triggers GLUT 4 to be inserted into membrane - Makes target tissue permeable to glucose - Most tissues are impermeable to tissues except brain and liver without insulin Insulin target tissues - Adipose - Liver Regulation of insulin secretion - Blood glucose increase - Insulin secretion increases - Storage hormone, reduce glucose levels - Promotes storage for long term use fo glucose fat and amino acids Glucagon - Responds to decreased blood glucose levels - Triggers an increase in blood glucose - Insulin and glucagon act oppositely Type 1 diabetes BHS 116.2 – Physiology Notetaker: Vivien Yip - Date: 2/6/2013, 1st hour Page6 Autoimmune Hyperglycemia Insulin deficiency Attack on beta cells, preventing insulin release All other symptoms stem from hyperglycemia Type II diabetes - Insulin resistance initially - Later on, can result in insulin deficiency - Know long term effects - Sorbitol pathway Alimentary Tract - Functions: move food through, digestion, absorption of nutrients - Regulatory mechanism: nervous and hormonal - Cross section of gut o Mucosa o Submucosa o Muscularis externa Outer longitudinal layer: peristalsis Circular layer: mixing o Serosa Slow wave potential - Smooth muscle - Interstitial cells of Cajal - Slow wave of subthreshold depolarization - If triggered by depolarizing factors near threshold - Stretch, Acetylcholine, parasympathetics and GI hormones - Know the difference between depolarizing and hyperpolarizing factor Enteric Nervous System - Myenteric o Control movement o Peristalsis and mixing - Submucosal plexus o Control secretion of GI tract Ingestion of Food - 3 stages o Voluntary o Pharyngeal o Esophageal Function of Stomach - Storage of food (main function) - Start digestive process - Antrum: thicker muscular layer and pushes food through pyloric sphincter to duodenum - Pyloric pump o Strong contractions and push a little bit of chime each time o It is always released in very small amounts to digest in small intestines Regulation of stomach emptying - Amount of chyme stimulates emptying and motility - Fluidity of chyme - Enterogastric reflex BHS 116.2 – Physiology Notetaker: Vivien Yip - Date: 2/6/2013, 1st hour Page7 Intestinal hormones (CCK, and secretin) Released when food is pushed into small intestines Movement of small intestine - Gastroenteric reflex o Initiated by distension of stomach o Increases motility - Hormonal control o Gastrin, CCK, insulin and serotonin all increase intestinal motility o Secretin and glucagon inhibit small intestine motility Movements of Colon - Main storage Secretion of Saliva - Salivary amylase, begins CHO digestion - Breakdown complex starches into simpler sugars - Lysozyme, breakdown bacterial cell walls - Antibody IgA also attacks bacteria - Mucus produced to help lubricate bolus of food to go down esophagus easier - Ductal cells: absorb sodium and chloride - Saliva is very devoid of sodium and chloride (we are very sensitive to salt) Summary of Gastric Secretion - Know what each of these cells secrete and what is triggering their secretion: - Mucous cells: protective mechanism - Chief cells - Parietal cells - Enterochromaffin cells - G cells - D cells - Acetylcholine produced by nervous system will stimulate the activity of most of these cells - Major inhibitory factor will be the somatostatin produced by D cells - Pepsinogen is an inactive enzyme o HCl is used to convert into the active pepsin o Pepsin can convert more pepsinogen to active pepsin Phases of Gastric Secretion - Cephalic phase o Sight and thought of food - Gastric Phase o Most abundant secretions occur when food has entered the GI o Once food leaves, there is a decrease in gastric secretion - Intestinal Phase Pancreatic Secretion - Exocrine portion: key role - Glandular cells will secrete digestive enzymes - Ductal cells secrete sodium bicarbonate to decrease acidity of chyme - Protect smooth muscle epithelium - Major enzymes involved are produced by pancreas - Only enzymes before that is salivary amylase and pepsinogen in the stomach - Primary enzymes produced by pancreas - Proteases will be inactive (activated in small intestine) - Trypsinogen to trypsin - Pancreatic amylase is released in active form BHS 116.2 – Physiology Notetaker: Vivien Yip Date: 2/6/2013, 1st hour Page8 Regulation of Pancreatic Secretion - Food in the duodenum primarily fat and protein trigger CCK release - CCK stimulate glandular/acinar cells to release pancreatic ezyme - Acetylcholine can also stimulate glandular cells Secretion of Bile by liver - Stored in gall bladder - CCK triggers release - Emulsify fats so that pancreatic lipase can break down more easily - Role in transporting products Digestion and Absorption of Carbohydrate Summary - Know the breakdown to absorption - Begins digestion in the mouth - Continues in small intestine - Epithelium of the small intestine (enterocytes) have small enzymes attached to its surface - Final digestion of carbohydrate and protein occurs in the enterocytes Glucose and galactose are taken up via co transport - Fructose is taken up by itself via facilitated diffusion - All 3 are transported out into the blood Protein Digestion - Starts in the stomach - Pepsin is the first enzyme - Mostly digested by pancreatic proteases - Aminopeptidase on surface of enterocytes are taken up - Amino acids are taken up via co-transport with sodium - small peptides taken up via hydrogen co-transporter - Only small amino acids are released in the blood Fat digestion - mechanical breakdown occurs via mixing movements - bile breaks down larger fat particles into smaller manageable particles - Triglycerides become free fatty acids and monoglycerides still lipid soluble o bile salts brings these to surface of enterocytes o can diffuse directly into target cell - Repackaged into triglycerides o form chylomicrons, large lipid particles o chylomicrons are exocytosed out of the enterocytes o enter lymphatic system o bypass portal system o eventually makes it to circulation to liver where it is processed