Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
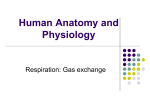
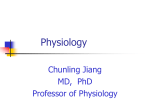
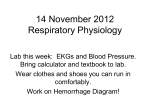
470 VENTILATION, PERFUSION MATCHING Papazian L, Thomas P, Garbe L, et al. (1995) Bronchoscopic or blind sampling techniques for the diagnosis of ventilator-associated pneumonia. American Journal of Respiratory and Critical Care Medicine 152: 1982–1991. Rello J, Ollendorf DA, Oster G, et al. (2002) Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest 122: 2115–2121. Richards MJ, Edwards JR, Culver DH, et al. (1999) Nosocomial infections in medical intensive care units in the United States: National Nosocomial Infections Surveillance System. Critical Care Medicine 27: 887–892. Torres A, Carlet J, Bouza E, et al. (2001) Ventilator-associated pneumonia. European task force on ventilator-associated pneumonia. European Respiratory Journal 17: 1034–1045. Vincent JL, Bihari DJ, Suter PM, et al. (1995) The prevalence of nosocomial infection in intensive care units in Europe: results of the European prevalence of infection in intensive care (EPIC) study. Journal of the American Medical Association 274: 639–644. VENTILATION, PERFUSION MATCHING P D Wagner, University of California – San Diego, La Jolla, CA, USA & 2006 Elsevier Ltd. All rights reserved. Abstract The lungs exist primarily to exchange gases between the environment and the blood. This is accomplished by three linked processes: convective transport of air to the alveoli (ventilation), diffusion of gas molecules between alveolar gas and pulmonary capillary blood, and convective transport in blood by cardiac pumping (perfusion). The lung is unique because these processes are accurately described by simple mass balance considerations, which show that the ventilation/perfusion ratio (V̇A/Q̇) is the key determinant of alveolar gas exchange. When the V̇A/Q̇ is not the same everywhere throughout the lungs, V̇A/Q̇ inequality is said to exist, causing hypoxemia, hypercapnia, and reduced O2 uptake and CO2 elimination. This compromises tissue metabolism, and may cause tissue hypoxia and acidosis. Clinical assessment of V̇A/Q̇ inequality is thus important, and uses three measures: alveolar–arterial PO2 difference, physiological deadspace, and physiological shunt. The body has three principal ways of compensating for continuing V̇A/Q̇ inequality. First, mixed venous PO2 falls and PCO2 rises, usually restoring V̇O2 and V̇CO2, but causing further hypoxemia and hypercapnia. Second, ventilation increases, stimulated partly by hypoxemia and hypercapnia. While usually effective in normalizing arterial PCO2 , PO2 often remains low. Third, cardiac output may rise, increasing mixed venous, and thus arterial, PO2 . Description Basic Principles The principal function of the lungs is the uptake of O2 from the atmosphere into the circulating blood, and the elimination of CO2 produced by metabolism. This requires three major gas transport processes: ventilation (see Ventilation: Overview) to bring inspired air to the alveoli, and alveolar gas to the atmosphere; diffusion (see Diffusion of Gases) to transfer gases across the alveolar–capillary blood–gas barrier; and blood flow (see Pulmonary Circulation) to transport gases in blood between the lungs and body tissues. Other gases, including inhaled pollutants and anesthetics, are exchanged similarly. The same principles of gas exchange apply to all gases, whether they form chemical species in blood or are carried simply in physical solution, and for both uptake and elimination. Except for a few situations, the process of diffusion reaches equilibration. That is, alveolar and endcapillary partial pressures of gases are not significantly different. Here it will be considered that diffusion equilibration exists. Ventilation is tidal, and tidal volume is usually small (B500 ml) compared to alveolar volume (B3000 ml). Because anatomical deadspace (the volume of the conducting airways) is B150 ml, the amount of fresh air reaching alveoli with each breath is only 500–150 or B350 ml. Each breath thus ‘‘tops up’’ the alveolar volume by only about 10%. Respiratory frequency is B15 breaths min 1. This pattern of small but frequent breaths causes alveolar gas concentrations to vary minimally within each breath. They are therefore taken to be constant (under steady-state conditions). Despite pulsatile pulmonary blood flow, endcapillary and arterial blood gas concentrations are also taken to be constant in time. Because the amounts of inhaled gases depend on ventilation, and the amounts transported in the blood depend on blood flow, it is apparent that ventilation and blood flow critically affect the amounts of gas exchanged, and also the alveolar and blood concentrations and partial pressures. These concepts can be considered more concretely by describing gas exchange using the laws of mass balance. These laws acknowledge that all molecules of a gas removed from alveolar gas during gas uptake appear in the blood, while during gas elimination, all molecules removed from the blood appear in the alveolar gas. Ventilation, Perfusion, and Gas Exchange Using O2 as the example, the laws of mass balance are now applied to steady-state gas exchange to VENTILATION, PERFUSION MATCHING 471 quantify the relationships between ventilation, blood flow, and alveolar (and endcapillary) concentrations (and partial pressures). The volume of O2 inhaled per minute is the product of the total inspired alveolar ventilation (V̇I) and the fractional concentration of O2 in inspired gas (FIO2 ): ½1 Volume inhaled ¼V’ I FIO2 law of partial pressures. V’ I and V’ A are almost identical, differing only when the amount of O2 taken up does not equal the amount of CO2 eliminated. Normally, V’ O2 is B300 ml min 1, V’ CO2 is B240 ml min 1. The difference, 60 ml min 1, is small in comparison to normal alveolar ventilation, which is usually 5–6 l min 1. While taking V’ I ¼ V’ A will introduce a small error, for ease of presentation, equality will be assumed so that The volume of O2 exhaled per minute is the product of the total expired alveolar ventilation (V̇A) and the fractional concentration of O2 in alveolar gas (FAO2 ): ’ ¼ k ½Cc0 CVO =½PIO PAO V’ A=Q 2 2 2 O2 Volume exhaled ¼V’ A FAO2 ½2 The difference between these must be the amount of O2 transferred from the atmosphere to the pulmonary capillary blood, that is, the V’ O2 : V’ O2 ¼ V’ I FIO2 V’ A FAO2 ½3 We can apply identical considerations to the pulmonary circulation. The volume of O2 that leaves the capillaries en route to the left atrium per minute is ’ and the the product of pulmonary blood flow (Q) concentration of O2 in that blood (Cc0O2 ): ’ Cc0 Volume leaving ¼ Q O2 ½4 However, the blood entering the pulmonary circulation carries O2 , and the volume of O2 in this venous ’ and blood entering per minute is the product of Q concentration of O2 in the venous blood: ’ CVO Volume entering ¼ Q 2 ½5 The difference between the volumes of O2 leaving and entering the pulmonary circulation/min is the amount of O2 taken up from the alveolar gas (V’ O2 ): ’ Cc0 Q ’ CVO V’ O2 ¼ Q 2 O2 ½6 Equations [3] and [6] both describe the amount/min of O2 taken up by the lungs (which in a steadystate equals tissue metabolic rate), and may thus be combined: ’ Cc0 Q ’ CVO V I FIO2 V’ A FAO2 ¼ Q 2 O2 Which may be rearranged to ’ ¼ ½Cc0 CVO =½ðV’ I=V’ AÞ FIO FAO ½7 V’ A=Q 2 2 2 O2 or ’ ¼ k ½Cc0 CVO =½ðV’ I=V’ AÞ V’ A=Q 2 O2 PIO2 PAO2 ½8 where k allows fractional concentrations (F) to be replaced by partial pressures (P) based on Dalton’s ½9 Now because alveolar and endcapillary PO2 values are taken to be the same (see above and Diffusion of Gases), Cc0O2 is the O2 concentration corresponding to the alveolar PO2, PAO2 . This equation therefore states: for a given composition of the venous blood (CVO2 ) and inspired gas (PIO2 ), the alveolar PO2 (PAO2 ) is uniquely determined by the ratio of venti’ lation to blood flow (V’ A=Q). In a region of lung having a low value of V̇A/Q̇ (e.g., partial airway obstruction), PAO2 must be low. If airway obstruction is complete, V̇A is zero, and local PO2 equals that of venous blood. If the local V̇A/Q̇ ratio is high (e.g., partial vascular obstruction), PAO2 will be high. If vascular obstruction is complete, Q̇ is zero, and PAO2 must equal that of inspired gas. Identical principles may be applied to all other gases, and similar relationships will be obtained. For CO2 this becomes ’ ¼ k ½CVCO Cc0 =½PACO PICO V’ A=Q 2 2 2 O2 ½10 The unique relationship between V̇A/Q̇ and PAO2 (and between V̇A/Q̇ and PACO2 ) is shown in Figure 1. Normal total alveolar ventilation and pulmonary blood flow are each about 5–6 l min 1. Therefore, the overall lung V̇A/Q̇ ratio is B1.0. Figure 1 shows that PAO2 is B100 mmHg and PACO2 is B40 mmHg at that V̇A/Q̇ ratio. Hence, these values are those expected in a perfectly homogeneous lung with a normal V̇A/Q̇ ratio. They are very close to what is seen in young normal subjects, suggesting close matching of ventilation to blood flow throughout the many alveoli in their lungs. Ventilation/Perfusion Inequality and Gas Exchange All normal subjects have what is called ventilation/ perfusion (V̇A/Q̇) inequality. This is defined as the situation where the V̇A/Q̇ ratio is not the same everywhere throughout the lungs. It results from both gravitational and nongravitational influences on how both ventilation and blood flow are distributed (see Pulmonary Circulation. Ventilation: Overview). 472 VENTILATION, PERFUSION MATCHING 50 Alveolar P CO2 (mmHg) Alveolar PO2 (mmHg) 140 120 100 O2 80 60 40 20 0 0.001 (a) 0.01 0.1 1 10 100 40 30 CO2 20 10 0 0.001 1000 (b) Ventilation/perfusion ratio 0.01 0.1 1 10 100 Ventilation/perfusion ratio 1000 (c) 140 Alveolar PCO2 (mmHg) Alveolar PO2 & P CO2 (mmHg) The O2–CO2 diagram 50 O2 120 100 80 60 40 CO2 20 0 0.001 40 30 20 10 0 0.01 0.1 1 10 100 Ventilation/perfusion ratio 0 1000 (d) 20 40 60 80 100 120 140 160 Alveolar PO2 (mmHg) Figure 1 (a) Alveolar PO2 (P AO2 ) depends on the ventilation/perfusion (V̇A/Q̇) ratio, based on eqn [8]. When the V̇A/Q̇ ratio is normal (B1), P AO2 ¼ 100 mmHg. When V̇A/Q̇ is both very low and very high, P AO2 is insensitive to V̇A/Q̇. Part (b) shows the corresponding relationship for P AO2 , and part (c) superimposes the two for comparison. Part (d) plots P ACO2 against P AO2 , creating the O2–CO2 diagram, where each point on the line corresponds to a unique value of V̇A/Q̇. The left end of the line represents a V̇A/Q̇ of 0, reflecting mixed venous blood composition; the right end similarly reflects inspired gas and an infinitely high V̇A/Q̇. When V̇A/Q̇ inequality exists, gas exchange becomes inefficient. Specifically, arterial PO2 falls, arterial PCO2 rises, and pulmonary V’ O2 and V’ CO2 both fall, failing to meet the body’s metabolic needs to supply O2 and eliminate CO2. Unless V’ O2 and V’ CO2 are restored, either by removing the cause of inequality or by the compensatory mechanisms discussed below, tissue damage will ensue. How V̇A/Q̇ inequality causes these changes is conveniently illustrated in a simple model of inequality in a ‘two alveolus’ lung. Figure 2(a) depicts a perfect lung for reference, and two examples of inequality. In Figure 2(b) an inhaled foreign object has reduced ventilation in one alveolus by 90%; in Figure 2(c) a blood clot has reduced blood flow in one alveolus similarly by 90%. In both cases, this is the only perturbation. Thus, total alveolar ventilation and pulmonary blood flow remain normal, and the distribution of blood flow in Figure 2(b) and of ventilation in Figure 2(c) are unchanged from control. Moreover, venous blood composition is the same in all three cases. Therefore, these examples illustrate pure effects of inequality prior to any compensatory changes (described below) that would normally occur. PAO2 and PACO2 in each alveolus in Figure 2 were obtained from the relationships in Figure 1. In Figure 2(a), each alveolus has the same V̇A/Q̇ ratio of 1.0, and thus has the same PAO2 and PACO2 . As the expired gas streams from the two alveoli mix, overall exhaled PO2 must be the same as PAO2 in each alveolus, that is, 100 mmHg. So too, mixed exhaled PACO2 must be 40 mmHg. Turning to the vascular side, each ‘pulmonary vein’ carries blood at the same PO2 of 100 mmHg and PCO2 of 40 mmHg. Thus, mixed arterial blood must also have these values. Consequently, there is no difference between mixed alveolar and mixed arterial PO2 (or PCO2 ) in this perfect lung. V’ O2 is 300 ml min 1 and V’ CO2 240 ml min 1, numbers determined by inserting PAO2 ¼ 100 into eqn [3], and PACO2 ¼ 40 into the corresponding equation for CO2. In Figure 2(b), exemplifying partial airway obstruction, the same analysis is now applied, using Figure 1 to determine the alveolar PO2 and PCO2 for the two alveoli. With 90% reduction in ventilation of the left alveolus, its V̇A/Q̇ ratio becomes 0.1, while redistribution of ventilation to the right alveolus makes its V̇A/Q̇ ratio 1.6. PAO2 and PACO2 (Figure 1) VENTILATION, PERFUSION MATCHING 473 VA (total) = 5.2 VA (total) = 5.2 100 (mixed exhaled PO ) 2 40 (mixed exhaled PCO ) Q (total) = 6.0 VO = 300 2 VCO = 240 115 (mixed exhaled PO ) 2 36 (mixed exhaled PCO ) Q (total) = 6.0 VO = 199 2 VCO = 213 2 2 2 2 VA : VA : 2.6 PAO : 2 PACO : 2 Q: VA /Q : 2.6 PAO : 2 PACO : 100 40 100 40 3 0.9 0.3 47 46 2 Q: 3 0.9 100 (mixed arterial PO2) 40 (mixed arterial PCO2) (a) VA/Q : 4.9 119 35 3 3 0.1 1.6 58 (mixed arterial PO ) 2 40 (mixed arterial PCO ) 2 (b) V A (total) = 5.2 108 (mixed exhaled PO ) 2 31 (mixed exhaled PCO ) Q (total) = 6.0 VO 2 = 263 2 VCO = 182 2 VA : 3 PAO : 2 PACO : 141 17 2 Q: VA/Q: 3 75 44 0.3 5.7 10 0.53 75 (mixed arterial PO ) 2 42 (mixed arterial PCO ) 2 (c) Figure 2 (a) This shows a lung divided into two hypothetical alveoli, each receiving 50% of the total alveolar ventilation and perfusion. Each therefore has the same V̇A/Q̇ ratio, making the lung homogeneous. This lung exchanges normal amounts of O2 and CO2; arterial PO2 and PCO2 are 100 and 40 mmHg, respectively. (b) Severe airway obstruction in one airway, reducing alveolar V̇A/Q̇ tenfold. The result is arterial hypoxemia and hypercapnia, and reduced O2 uptake and CO2 elimination. (c) Severe pulmonary vascular obstruction, also causing hypoxemia, hypercapnia, and reduced gas exchange. P AO2 and P ACO2 for each alveolus in all three models are derived from eqns [8] and [10]. are shown. As the two alveoli exhale and their gas streams mix, the mixed exhaled PO2 (PEO2 ) must be the average of the PAO2 values from each, weighted by the amounts of exhaled gas coming from each. This is simply applying principles of mass conservation: PEO2 ¼ ½PAO2 ðleftÞ V’ AðleftÞ þ PAO2 ðrightÞ V’ AðrightÞ=V’ AðtotalÞ ¼ 115 mmHg ½11 Similar mixing of the endcapillary blood from the two alveoli produces a mixed arterial PO2 of 58 mmHg. Here, the mixing computation is done using endcapillary O2 concentrations, not partial pressures. The PO2 corresponding to this mixed arterial O2 concentration is then read from the oxygen–hemoglobin dissociation curve (see Oxygen–Hemoglobin Dissociation Curve). When eqn [3] is used with the mixed expired PO2 above, V’ O2 for the entire lung is seen to be only 199 ml min 1. V’ CO2 is also reduced, to 213 ml min 1. Thus, this model of V̇A/Q̇ inequality shows substantial arterial hypoxemia and slight hypercapnia (compared to A), and reduced ability to exchange both O2 (34% reduction in V’ O2 ) and CO2 (11% reduction in V’ CO2 ). In Figure 2(c), the model of pulmonary vascular obstruction, an identical analysis shows that mixed exhaled PO2 and PCO2 will be 108 and 31 mmHg respectively; mixed arterial PO2 and PCO2 will be 75 and 42 mmHg, respectively, and V’ O2 and V’ CO2 for the entire lung are both reduced, to 263 (12% reduction) and 182 (24% reduction) mmHg, respectively. The important result is that it does not matter whether the cause of the V̇A/Q̇ inequality resides in the airways or the vasculature, hypoxemia and hypercapnia will occur, as will a reduction in the amount 474 VENTILATION, PERFUSION MATCHING of both O2 and CO2 that the lungs can exchange. The absolute effects differ with the nature of the inequality, and in particular the model in Figure 2(b) affects O2 more than CO2 while the model in Figure 2(c) affects CO2 more than O2. Compensation for Ventilation/Perfusion Inequality The reductions in V’ O2 and V’ CO2 described above prevent the lungs from meeting the tissue metabolic requirements. If the V̇A/Q̇ inequality is not corrected, compensatory mechanisms must be brought into play to restore V’ O2 and V’ CO2 . Three principal mechanisms exist. The first is a fall in venous PO2 (and rise in venous PCO2 ). This happens immediately and requires no conscious effort or energy expenditure. It is effective because prior to developing V̇A/Q̇ inequality, venous PO2 is high enough (B40 mmHg) to provide enough room for such a fall. This can usually restore the arterio venous O2 concentration difference and therefore V’ O2 (and V’ CO2 ). However, it causes a further fall in arterial PO2 (and rise in arterial PCO2 ). In the model in Figure 2(b), this mechanism can restore the V’ O2 and V’ CO2 of the entire lung. Venous PO2 would have to fall by about 10 mmHg and venous PCO2 would have to increase by about 5 mmHg. Arterial PO2 and PCO2 would now be 48 and 45 mmHg respectively, showing more hypoxemia and hypercapnia than before compensation occurred. In Figure 2(c), corresponding changes restore V’ O2 and V’ CO2 , resulting in venous PO2 and PCO2 values lower by about 2 and higher by about 16 mmHg, respectively. Arterial PO2 falls to 63 and PCO2 rises to 57 mmHg, respectively. While this primary, rapid, automatic process achieves the major objective of restoring both V’ O2 and V’ CO2 , the fall in arterial PO2 and rise in arterial PCO2 put the patient at greater risk of tissue hypoxia and acidosis than even the initial disturbance of V̇A/Q̇ relationships caused. The second compensatory mechanism is an increase in ventilation. This mitigates arterial hypoxemia and hypercapnia, reducing tissue hypoxia and acidosis. The stimuli to increasing ventilation in the face of V̇A/Q̇ inequality (arterial hypoxemia, acidosis, and especially hypercapnia) are discussed in the article Ventilation: Control. Depending on the cause of V̇A/Q̇ inequality, increased ventilation may not be possible, as for example when severe chest trauma is responsible. But when in the models of Figure 2 ventilation is progressively increased, arterial PO2 and PCO2 gradually improve. Since V’ O2 and V’ CO2 have already been restored by the first compensatory mechanism, they remain normal as ventilation is raised. Figure 3 shows the effects of ventilatory compensation in the two models of Figure 2. Note that arterial PCO2 is much easier to normalize than is arterial PO2 , especially in the model of airway obstruction with very low V̇A/Q̇ ratios. This directly reflects the differences in the shapes and slopes of the O2 and CO2 dissociation curves in blood (see Carbon Dioxide. Oxygen–Hemoglobin Dissociation Curve). Because the curve for CO2 is nearly linear while that for O2 is quite nonlinear, arterial PCO2 is easier to normalize than is arterial PO2 . This difference in ability to restore arterial PO2 and PCO2 by increased ventilation often leads to a large increase in ventilation, sufficient to cause hypocapnia, while still not normalizing arterial PO2 (as the model suggests in Figure 3(b)). Figure 3 shows the progression of expected arterial blood gas values that would be anticipated stage by stage as these compensation processes occurred for the two models in Figure 2. It should be realized that while these stages are presented sequentially, in real life they would be occurring essentially together over a short time frame and would probably all be in place by the time a physician saw the patient. An important conclusion from analyzing this sequence of events is that just because a patient with V̇A/Q̇ inequality may present with hypoxemia but not hypercapnia, it should not be thought that inequality affects only O2 and not CO2. In fact, some patterns of inequality, especially those in which areas of very high V̇A/Q̇ ratio develop, can affect CO2 more than O2 (Figure 2(c)). The third way in which the body can compensate for V̇A/Q̇ inequality is by increasing cardiac output. This is not infrequently seen in young asthmatic patients, and in the intensive care unit in patients who have high cardiac outputs from sepsis and other pathologies. What an increase in cardiac output allows is an increase in the venous PO2 . This can be deduced from eqn [6], otherwise known as the Fick principle. This equation shows that for a given metabolic rate ’ results in a (V’ O2 ), and increase in cardiac output (Q) reduction in the arteriovenous O2 concentration difference, and in turn a rise in venous PO2 . When low V̇A/Q̇ ratio regions exist, an increase in venous PO2 will result in an increase in arterial PO2 . For example, in model B, increasing cardiac output from 6 to 10 l min 1 permits an increase in arterial PO2 from 48 to 55 mmHg. While this seems modest, arterial O2 saturation would rise from about 83% to almost 90%, significantly enhancing the arterial O2 concentration. While increases in either or both ventilation and cardiac output allow both arterial PO2 and PCO2 to move towards normalization, two points need VENTILATION, PERFUSION MATCHING 475 50 110 Arterial PCO 2 (mmHg) Arterial PO2 (mmHg) 100 90 80 70 60 50 40 30 Obstruction : Venous PO2 : Ventilation : O2 uptake : 45 40 35 30 25 Pre Post 41.6 41.6 32.5 32.3 32.2 32.1 32.0 31.9 31.8 5.2 5.2 300 199 Obstruction : Venous PCO2 : 7.5 Ventilation : 300 300 300 300 300 300 300 CO2 elimination : 5.2 5.8 6.0 6.3 6.5 7.0 5.2 5.2 5.2 5.8 6.0 6.3 240 213 240 240 240 240 6.5 7.0 7.5 240 240 240 (b) 110 60 100 55 Arterial PCO2 (mmHg) Arterial PO2 (mmHg) (a) Pre Post 45.8 45.8 50.2 45.4 44.1 42.4 41.2 38.7 36.6 90 80 70 60 50 Ventilation : O2 uptake : 40 35 30 25 40 Obstruction : Venous PO2 : 50 45 Pre Post 41.6 41.6 39.8 41.3 41.2 40.8 40.4 39.5 38.7 5.2 5.2 5.2 300 263 300 300 6.0 7.0 7.5 8.0 Obstruction : Venous PCO2 : Ventilation : 9.0 10.0 300 300 300 300 300 (c) CO2 elimination : Pre Post 45.8 45.8 62.4 54.7 47.9 45.1 42.6 38.4 35.0 5.2 5.2 240 182 5.2 6.0 7.0 7.5 240 240 240 240 8.0 9.0 10.0 240 240 240 (d) Figure 3 Compensation for V̇A/Q̇ inequality in the models of Figure 2, showing how arterial PO2 (a, c) and PCO2 (b, d) respond. Parts (a) and (b) reflect airway obstruction; parts (c) and (d) vascular obstruction. In each case, the second bar shows effects of inequality prior to compensation. The third bar shows restoration of V’ O2 and V’ CO2 by changes in mixed venous PO2 and PCO2 alone. The remaining bars show responses to increasing alveolar ventilation. See text for more details. further consideration. First, increasing ventilation and cardiac output are both energy requiring, and patients with already compromised ventilatory or cardiac pumps may not be able to respond well. Second, in those patients who do respond with brisk increases in ventilation and/or cardiac output, the improvement in their arterial blood gases may lead the physician to underestimate the extent of the underlying V̇A/Q̇ inequality. In other words, patients who show substantial increases in either ventilation or cardiac output and have nearly normal arterial blood gases may still have considerable V̇A/Q̇ inequality, and should be managed with this in mind. Assessment of Ventilation/Perfusion Inequality The detailed assessment of V̇A/Q̇ inequality is difficult, especially in clinical settings. Most often, the lung is modeled as consisting of three virtual alveoli. One of these is unventilated, but perfused, and is labeled as a ‘shunt’. Another is ventilated but not perfused, and is labeled as a ‘deadspace’. The third is labeled the ‘ideal’ alveolus, and is both perfused and ventilated. The objective in assessing V̇A/Q̇ inequality in this framework is to (1) apportion total ventilation between the ideal and deadspace alveoli on the one hand, and (2) apportion total cardiac output between the ideal and shunt alveoli on the other. This is a gross oversimplification of reality in almost all patients, but does provide a quantitative index of V̇A/Q̇ inequality that can be useful in guiding therapy. To apportion ventilation between the ideal and deadspace alveoli, one must measure both arterial PCO2 (PaCO2 ) and the PCO2 of mixed expired gas (PECO2 ). On the presumption that the deadspace alveolus contains no CO2 (because it is unperfused and therefore cannot get CO2 from the blood), while the 476 VENTILATION, PERFUSION MATCHING PCO2 of the ideal alveolus equals that of the measured arterial blood, a conservation of mass analysis (much like that in eqn [11]) shows that the fraction of the total ventilation received by the deadspace alveolus (commonly referred to as VD/VT) comes to V D=V T ¼½PaCO2 PECO2 =PaCO2 ½12 This is called the ‘physiological’ deadspace because it is measured using functional variables, and because it includes all causes of deadspace in a single outcome measure. Specifically, the normal contribution to deadspace from the conducting airways is a part of VD/VT, as are additional components caused by the presence of any regions of high V̇A/Q̇ ratio, if any. In other words, VD/VT would be around 0.3 in a normal subject because the conducting airway volume is about 150 ml while the tidal volume is about 500 ml (150/500 ¼ 0.3). Any value of VD/VT higher than this would suggest the presence of alveolar regions of high V̇A/Q̇ ratio. This conclusion must be accepted with caution however, since changes in tidal volume can have an obvious, significant effect on VD/VT since the numerator, conducting airway volume, is relatively constant as tidal volume changes. To overcome this limitation, multiplying VD/VT by measured tidal volume will yield an absolute value for VD per breath. This should be about 150 ml in a normal person irrespective of tidal volume, and so an increase above such a value is a better indication of the presence of areas of high V̇A/Q̇ ratio. In reality, conducting airway volume varies with body size, and a commonly used estimate is about 1 ml per pound of body mass, correcting mass for obesity when significant. To estimate perfusion in the ‘shunt’ alveolus, a similar mass conservation approach is taken, but in this case one uses measures of O2 exchange. One must measure both arterial and venous (pulmonary arterial) O2 concentrations (CaO2 and CvO2 , respectively). The endcapillary O2 concentration in the ideal alveolus (Cc0O2 ) cannot be measured but is needed and is thus calculated from an estimate of its alveolar PO2. The equation that describes the perfusion of the shunt alveolus as a fraction of the total cardiac output (QS/Q̇T) is ’ T ¼ ½Cc0 CaO =½Cc0 CvO QS=Q 2 2 O2 O2 ½13 Unlike the case for VD/VT, QS/Q̇T in normal subjects is essentially zero. Thus, any elevation (perhaps allowing 0.01–0.02 to encompass the range of normal responses) is abnormal. An important consideration in applying this equation arises when CvO2 is not in fact measured, but is assumed. As the equation shows, an error in CvO2 will give rise to an incorrect value for QS/Q̇T. The second major consideration when using this equation relates to the meaning of the value obtained as QS/Q̇T. In the case where there is truly a pure shunt in the patient’s lung (e.g., in lobar consolidation, in atelectasis, or in the event of a right to left intracardiac communication), the value obtained accurately estimates the fraction of the cardiac output that is perfusing the abnormal pathway. However, in the relatively more common setting where areas of low V̇A/Q̇ ratio are present rather than true shunts, the value of QS/Q̇T must be thought of as the fraction of the cardiac output that would flow through a hypothetical shunt pathway and lead to the same arterial PO2 as measured in the patient. Because alveolar (and thus endcapillary) PO2 in low V̇A/Q̇ regions is higher than in venous blood flowing through a pure shunt pathway, the actual perfusion rate in low V̇A/Q̇ areas will always exceed that obtained from eqn [13]. A special consideration relates to use of eqn [13] when FIO2 is raised, as is often the case in the ICU. The higher the FIO2 , the less will regions of low V̇A/Q̇ ratio interfere with O2 exchange. In particular, when FIO2 is 1.0, each ventilated alveolus, no matter what its V̇A/Q̇ ratio is, contains only O2, CO2, and water vapor as the resident N2 is eliminated. This means that even in regions of very low V̇A/Q̇ ratio, alveolar PO2 will be several hundred mmHg, and allow full saturation of endcapillary blood. In practice, this means that QS/Q̇T breathing pure O2 will be zero even if V̇A/Q̇ inequality is present, unless there is also a shunt. It also means that when both V̇A/Q̇ inequality and shunt coexist in the same lungs, QS/Q̇T measured while breathing air will exceed that measured while breathing pure O2. Measuring QS/Q̇T under both conditions therefore affords a way to separately assess the magnitude of V̇A/Q̇ inequality and shunt. This well-established technique should be used with some caution, however. This is because by giving pure O2 to a patient, some alveoli that were ventilated, albeit poorly, on room air, may cease to be ventilated and collapse, thereby increasing the size of the shunt. Furthermore, increasing FIO2 may release hypoxic vasoconstriction in these hypoxic areas, raising their perfusion levels, and increasing the measured shunt fraction even more. A third method for characterizing V̇A/Q̇ inequality is to determine the alveolar–arterial PO2 difference (AaPO2 ). As Figure 2 shows, the difference between mixed alveolar and arterial PO2 is normally close to zero. However, V̇A/Q̇ inequality increases alveolar and reduces arterial PO2 , causing AaPO2 to increase. While arterial PO2 is easily measured from a blood sample, mixed alveolar PO2 is difficult to measure, and is thus calculated from the alveolar gas equation. This equation uses eqn [3] above and the VENTILATION, PERFUSION MATCHING 477 corresponding equation for CO2 to estimate alveolar PO2 (PAO2 ) as PAO2 ¼ PIO2 PACO2 =R þ PACO2 FIO2 ½ð1 RÞ=R ½14 A simpler version ignores the third term because it generally is only 1–2 mmHg: PAO2 ¼ PIO2 PACO2 =R ½15 where R is the ratio of V’ CO2 to V’ O2 (the respiratory exchange ratio). Then AaPO2 ¼ PAO2 PaO2 ½16 Most often, one uses the measured arterial PCO2 (PaCO2 ) in place of the alveolar value, because they are generally quite similar. This means that the AaPO2 can be calculated from just the arterial PO2 and PCO2 , provided one knows PIO2 (inspired PO2 ) and R. PIO2 is usually easy to determine, but R is often assumed. It should be recognized that small errors in R can cause substantial errors in AaPO2 . The final expression is AaPO2 ¼ PIO2 PaCO2 =R PaO2 The Multiple Inert Gas Elimination Technique Another approach to assessing the amount of V̇A/Q̇ inequality is to use what is known as the multiple inert gas elimination technique (MIGET) to measure directly the frequency distribution of ventilation/perfusion ratios throughout the lungs. This method makes use of the fact that the degree to which any particular inert gas is eliminated by the lungs from the body (after being introduced by either inhalation or intravenous infusion) depends on the distribution of ventilation and blood flow throughout the lungs. The degree of elimination also depends on the blood solubility of the gas, and it turns out that it is necessary to have about six or so gases of widely differing solubilities to obtain sufficient information from which to compute the distribution. The physiological basis of this method is the same mass balance principle discussed extensively above Asymptomatic asthma, .PaO2 = 79; FEV1 = normal Normal subject 1.8 1.8 Normal VA /Q 1.2 0.9 0.6 0.0 No shunt No low VA /Q No high VA /Q 1.2 0.9 0.6 0.3 (a) 0.01 0.1 1 10 Ventilation/perfusion ratio 0 100 (b) Severe, chronic asthma, .PaO2 = 53; FEV1 = 35% predicted 1.8 0.01 0.1 1 10 Ventilation/perfusion ratio 100 COPD: predominant emphysema Normal VA /Q Normal VA /Q 1.5 Low VA /Q 1.2 0.9 0.6 No shunt No high VA /Q Ventilation ( ), Blood flow ( ) Ventilation ( ), Blood flow ( ) No high VA /Q 1.8 1.5 1.2 0.6 0.0 0 0.01 0.1 1 10 Ventilation/perfusion ratio 100 High VA /Q 0.9 0.3 0.0 (c) Low VA /Q No shunt 0.0 0 0.3 Normal VA /Q 1.5 Ventilation ( ), Blood flow ( ) Ventilation ( ), Blood flow ( ) 1.5 0.3 ½17 No shunt 0 (d) Low VA /Q 0.01 0.1 1 10 Ventilation/perfusion ratio 100 Figure 4 V̇A/Q̇ distribution showing how ventilation and blood flow are distributed with respect to V̇A/Q̇ ratio throughout the lungs. The normal distribution (a) is narrow and symmetrical; that in mild asthma (b) and severe asthma (c) contains normal areas and also areas of very low V̇A/Q̇ ratio, the latter due to partial airway obstruction; that in emphysema (d) has, in addition to normal regions, areas of very high V̇A/Q̇ probably caused by continued ventilation through poorly perfused ‘holes’ in the lung. 478 VESICULAR TRAFFICKING for O2 and CO2, and shown in eqns [9] and [10]. From the measured pattern of elimination of the several gases, mathematical procedures are used to calculate the distribution of V̇A/Q̇ ratios that best fit the elimination pattern over all six gases. The results are expressed as two separate but linked frequency distributions – one for ventilation and one for blood flow as in Figure 4. These distributions show how ventilation and blood flow are distributed along the V̇A/Q̇ ratio axis from essentially zero to essentially infinity. Figure 4(a) shows the distribution in a young normal subject; Figure 4(b) exemplifies mild asthma, Figure 4(c) severe asthma, and Figure 4(d) emphysema. The normal subject shows a narrow distribution around a mean V̇A/Q̇ of about 1, devoid of areas of very low or high V̇A/Q̇ ratio. The asthmatic lung contains substantial regions of very low V̇A/Q̇ ratio, but does not have areas of abnormally high ratio. The low V̇A/Q̇ areas in asthma presumably reflect partially obstructed airways, and may be seen even when forced expiratory volume in 1 s (FEV1) is normal or only slightly reduced. In contrast, the lung with emphysema shows abnormalities in the high V̇A/Q̇ domain, likely the result of continued ventilation of poorly perfused ‘holes’ in the lung parenchyma. The MIGET provides the most complete picture of V̇A/Q̇ inequality currently available that is usable in intact humans. It is a complex technique that demands considerable expertise and attention to detail, and remains a useful research tool in areas such as understanding the pathophysiology of, and therapeutic responses to, new treatments for lung diseases. See also: Carbon Dioxide. Diffusion of Gases. Oxygen–Hemoglobin Dissociation Curve. Pulmonary Circulation. Ventilation: Overview; Control. Further Reading Kelman GR (1968) Computer programs for the production of O2– CO2 diagrams. Respiration Physiology 4: 260–269. Rahn H and Fenn WO (1955) A Graphical Analysis of the Respiratory Gas Exchange. Washington, DC: American Physiological Society. Riley RL and Cournand A (1949) ‘‘Ideal’’ alveolar air and the analysis of ventilation/perfusion relationships in the lung. Journal of Applied Physiology 1: 825–847. Riley RL and Cournand A (1951) Analysis of factors affecting partial pressures of oxygen and carbon dioxide in gas and blood of lungs: theory. Journal of Applied Physiology 4: 77–101. Wagner PD (1978) Measurement of the distribution of ventilation/ perfusion ratios. In: Davies DG and Barnes CD (eds.) Regulation of Ventilation and Gas Exchange, pp. 217–260. New York: Academic Press. Wagner PD and West JB (1980) Ventilation–perfusion relationships. In: West JB (ed.) Ventilation, Blood Flow and Diffusion, pp. 219–262. New York: Academic Press. West JB (1969) Ventilation/perfusion inequality and overall gas exchange in computer models of the lung. Respiration Physiology 7: 88–110. West JB (1990) Ventilation/Blood Flow and Gas Exchange. Oxford and Philadelphia: Blackwell Scientific Publications and Lippincott. West JB and Wagner PD (2000) Ventilation, blood flow and gas exchange. In: Murray JF and Nadel JA (eds.) Textbook of Respiratory Medicine, pp. 55–89. Philadelphia, PA: Saunders. VESICULAR TRAFFICKING N E Vlahakis, Mayo Clinic Rochester, Rochester, MN, USA & 2006 Elsevier Ltd. All rights reserved. Abstract Vesicular trafficking is a continuous and dynamic process in all cells of the body, in which lipid vesicles move from the cell surface to intracellular lipid endosomes (endocytosis) or from organelles and endosomes to the cell surface (exocytosis). It functions as both a homeostatic process for maintenance of quiescent cell function and a stress response to ensure rapid protein synthesis, targeted intracellular transport, and expression of proteins on the cell surface or their release to the extracellular environment. Vesicles are primarily composed of lipid molecules that serve not only as a mechanical barrier to the perivesicular environment but also a physical support for their protein cargo during transport within the cell. Membrane lipids also provide a physical structure to prime vesicles for budding or fusion or to modulate protein function and resultant transduction of cellular signaling. Respiratory epithelium is polarized and the apical and basolateral membranes are maintained by tightly controlled and membrane-specific vesicular trafficking pathways to maintain this polarized phenotype. Any defect in this transport machinery can result in inadequate responses to cellular stressors or respiratory disease, such as cystic fibrosis and interstitial lung disease. The vesicular trafficking process in type II alveolar pneumocytes has many unique features and is essential for surfactant secretion and reuptake. In addition, a rapid and targeted trafficking response is required for alveolar cells to add lipids to the cell surface to prevent cell rupture or to ‘patch’ cell breaks. Description General Mechanisms of Vesicular Trafficking Lipid vesicles originate in the endoplasmic reticulum (ER), budding from the ER as a means to distribute