Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Res Medica, May 1961, Volume II, Number 4
Page 1 of 9
Auscultation of the Heart - III
R. W. D. Turner
O.B.E., M.A. (Cantab.). M.D., F.R.C.P.Ed., F.R.C.P.Lond.
Abstract
The essential difference between a sound and a murmur is that the former is due to sudden alteration in the
speed of blood flow whereas a murmur results from turbulence developing in the blood stream. A murmur is
usually of longer duration and of higher frequency than a sound. The principal factors which influence
turbulence are the velocity of flow, the density and viscosity of the blood and the diameter of the vessel.
Another important factor is that a narrowed orifice, as from valvular stenosis, will give rise to eddies beyond
the obstruction. A similar effect is produced by a relatively narrow vessel opening into a wider one as in
dilatation of the first part of the aorta or pulmonary artery.
Murmurs may be heard in systole or diastole or may appear to be continuous throughout systole and diastole.
Diastolic and continuous murmurs are always due to organic disease but a systolic murmur may be present not
only without any functional disability but without any clinical, radiographic or electrocardiographic evidence of
organic heart disease.
Copyright Royal Medical Society. All rights reserved. The copyright is retained by the author and the Royal Medical Society, except
where explicitly otherwise stated. Scans have been produced by the Digital Imaging Unit at Edinburgh University Library. Res Medica is
supported by the University of Edinburgh’s Journal Hosting Service: http://journals.ed.ac.uk
ISSN: 2051-7580 (Online) ISSN: 0482-3206 (Print)
Res Medica is published by the Royal Medical Society, 5/5 Bristo Square, Edinburgh, EH8 9AL
Res Medica, May 1961, 2(4): 25-32
doi: 10.2218/resmedica.v2i4.362
Turner, R. W. D. Auscultation of the Heart III, Res Medica 1961, 2(4), pp.25-32
doi: 10.2218/resmedica.v2i4.362
AUSCULTATION OF THE
HEART-
Ill.
By R. W ·.D. TU RN ER
O.B.E .. M.A. (Cantab.). M.D .. F.R.C.P.Ed .. F.I<.C.P.Lond.
MURMURS
Give me a calm and thankful heart,
From every murmur free.
-from a hymn by Anne Steele, 1760.
The essential difference between a sound and a murmur is that the former
is due to sudden alteration in the speed of blood flow whereas a murmur
results from turbulence developing in the blood stream. A murmur is usually
of longer duration and of higher frequency than a sound. The principal factors
which influence turbulence are the velocity of flow, the density and viscosity
of the blood and the diameter of the vessel. Another important factor is
that a narrowed orifice, as from valvular stenosis, will give rise to eddies
beyond the obstruction. A similar effect is produced by a relatively narrow
vessel opening into a wider one as in dilatation of the first part of the aorta or
pulmonary artery.
Murmurs may be heard in systole or diastole or may appear to be continuous
throughout systole and diastole.
Diastolic and continuous murmurs are always due to organic disease but a
systolic murmur may be present not only without any functional disability
but without any clinical, radiographic or electrocardiographic evidence of
organic heart disease.
In all cases in which a murmur is heard there should be noted, as described
in Part I of this paper, the area over which it is audible, the position of
maximal intensity, the direction of apparent radiation, the intensity (preferably
graded), the quality (using simple adjectives), and, where possible, the precise
timing in systole or diastole. It should also be noted whether it is associated
with a palpable thrill and if there is any abnormality of the heart sounds. In
cases of doubt phonocardiography, radiography, electro-cardiography and
other accessory methods of examination may be required before a firm
conclusion can be drawn.
SYSTOLIC MURMURS
Systolic murmurs may occur in association with various forms of acquired
or congenital heart disease or as an isolated finding unassociated with any
evidence for organic disease and may then be termed innocent, incidental or
functional. A functional murmur is due to turbulence in the absence of
significant structural abnormality.
RES MEDICA
However, it is not always possible to be certain that an apparently innocent
systolic murmur is not due to mild organic heart disease nor, of course, from
a single examination that such disease may not in time be progressive.
The chief danger is usually that of engendering anxiety and it is very
important indeed to avoid this and also the imposition of unwarranted
restrictions.
Infants and children must be kept under observation and examined at
intervals because at this age it is quite impossible to be certain as to the
nature of a svstolic murmur.
In young adults it is best to arrange for re-examination after say I2 months
at any rate but at the same time to give strong reassurance that no restrictions
in activity arc indicated and a normal life F D Q be lead in every wav.
In older patients an isolated systolic murmur can usually "be ignored but
it should be remembered that an aortic systolic murmur may signify valvular
stenosis which does not become of dynamic importance until quite late in
life, for example, after the age of 50.
CLASSIFICATION OF SYSTOLIC MURMURS
INNOCENT
Pulmonary
Apical
3· Parasternal
I.
2.
ORGANIC
A.
B.
Forward Flow
I. Aortic
Aortic stenosis or sclerosis
Increased flow (Aortic incompetence)
Coarctation of aorta
2. Pulmonary
Pulmonary stenosis
Increased flow
Physiological
Left to Right shunts
Backward Flow
Mitral or Tricuspid incompetence
Ventricular septal defect
DTFFERENTTAL DTAGNOSIS OF SYSTOLIC MURMURS
If a systolic murmur can be heard its characteristics should be noted as
described above and also if there is any associated thrill, diastolic murmur,
change in heart sounds or other evidence for heart disease.
Aortic Systolic Murmur
The most usual cause for a svstolic murmur that is loudest in the aortic
area is aortic stenosis but a similar murmur mav derive from sclerosis of the
valve, dilatation of the ascending aorta or inc-reased left ventricular stroke
volume as in aortic regurgitation. Normally a systolic murmur may be heard
just above the clavicle and occasionally it is also audible just below.
Pulmonary Systolic Murmur
The most usual cause for a systolic murmur that is loudest in the pulmonary
area is normal blood flow in the young; or increased blood flow with exercise,
emotion, pregnancy, anaemia, thyrotoxicosis or with a left to right shunt; or
pulmonary stenosis.
AUSCULTATION
Left Parasternal Systolic Murmur
The most usual cause for a systolic murmur that is loudest at the mid or
lower left sterna] border is one of the innocent varieties, tricuspid incompetence or congenital heart disease.
Mitral Area
The most usual cause for an apical systolic murmur is mitral incompetence
or an apparently innocent murmur.
It must be remembered that the murmur of aortic stenosis may be loudest
at the left sterna] border or even at the apex and that a basal systolic murmur
'conducted into the neck ' is not diagnostic of aortic stenosis but may be
present in pulmonary stenosis or congenital heart disease. Other causes for
a praecordial systolic murmur include coarctation of the aorta and patency
of the ductus arteriosus in infancy or with pulmonary hypertension.
If one comes to think of it, it is remarkable that blood flow through the
heart, past valves and protuberances and round bends should be so silent
and not surprising that minor irregularities of no structural consequence should
cause eddies associated with a murmur.
AORTIC SYSTOLIC MURMURS
An aortic systolic murmur may be due to aortic valvular stenosis or sclerosis,
to increased blood flow across the valve or to dilatation of the ascending aorta.
Aortic Stenosis
Characteristically the murmur of aortic stenosis is loudest in mid-systole
because this corresponds with the period of maximal blood flow.
Usually it can be appreciated by ear that the murmur ends before the
second heart sound and often that there is a distinct gap between the first
heart sound and the beginning of the murmur. Phonocardiographically it can
be shown to be "diamond-shaped".
An aortic systolic murmur may be loudest in the "aortic area," over the
sternum or down the left sterna] border or sometimes even at the apex.
Unless faint it can also be heard over the carotid arteries in the neck.
Even when the murmur is not loudest to the right of the upper sternum
signifying its probable source of origin it may be recognised as originating
in the aortic valve because it is also well heard in this region and in the neck
and because of associated features such as a systolic thrill maximal over the
right upper chest, weakness or absence of the aortic second sound and from
the fact that the murmur is loudest in mid-systole.
111ere may also, of course, be an early diastolic murmur from associated
aortic incompetence.
It is important to emphasise that the loudness of the mnrmnr bears no
close relation to the degree of stenosis.
PULMONARY SYSTOLIC MURMURS
A pulmonary systolic murmur may be due to pulmonary stenosis, to
increased blood flow across the pulmonary valve or to dilatation of the main
pulmonary artery. A pulmonary systolic murmur is probably the most
frequent of all innocent murmurs.
Pulmonary Stenosis
As with aortic stenosis the characteristic murmur of pulmonary stenosis is
loudest in mid-systole corresponding with the period of maximal ejection and
as with aortic stenosis there is no close relationship between the intensity
of the murmur and the degree of stenosis.
RES M E DICA
The murmur is usually accompanied by a systolic thrill and the intensity of
the thrill corresponds with the loudness of the murmur.
In pulmonary stenosis the second heart sound may be finely split, widely
split, faint or absent depending on the degree of stenosis.
Increased Pulmonary Blood Flow
A systolic murmur from increased blood flow across the pulmonary valve
may be associated with any hyperkinetic state such as pregnancy, anaemia or
thyrotoxicosis. It is often also heard in young persons especially on exercise.
In pathological states increased pulmonary flow may be associated with a
left to right shunt e.g. with patency of the ductus arteriosus, an1 atrial septal
defect or a ventricular septal defect.
Parasternal Systolic Murmurs
A systolic murmur which is loudest at the mid or lower left stcrnal border
is usually due to tricuspid incompetence, congenital heart disease or is one of
the innocent varieties.
Tricuspid Incompetence
Tricuspid incompetence may be clue to organic deformity of the cusps from
rheumatic endocarditis or to dilatation of the valve ring from cardiac failure.
In severe cases systolic pulsation in the jugular veins and over the liver may
be present. This murmur often increases in intensity during deep inspiration.
Congenital Heart Disease
The most usual cause is a ventricular septal defect. In such cases a corresponding systolic thrill is usually palpable.
Innocent Murmurs
This subject is discussed on page-
APICAL SYSTOLIC 1\1URMURS
A systolic murmur which is loudest at the apex always raises the possibility
of mitral incompetence and is perhaps the most frequent source of uncertainty.
If there is a past history of rheumatic fever, the murmur is heard out
towards the left axilla1 and if there is any radiographic evidence of left atrial
enlargement this diagnosis must be made. Even if there is no other abnormality whatsoever it still cannot be denied that minimal rheumatic mitral
disease may be developing and, if possible, the examination should be repeated
a year later. However, the undesirability of making an error and diagnosing
organic heart disease when none is present is far more important and of so
much greater potential harm than mistaking a minor organic murmur that
this slight risk may reasonably be taken. In the occasional instance even
bacterial endocarditis may subsequently develop in mild rheumatic mitral
disease but on balance there can be no question that this risk also should be
accepted. From the practical point of view minor mitral incompetence is of
no dynamic significance and the patient should be reassured that the heart is
healthy.
ISOLATED SYSTOLIC MURMURS
Isolated (' innocent,' 'incidental ' or 'functional ') systolic murmurs are of
frequent occurrence in health and often pose a problem for the physician
either because such a finding is made during the examination of a patient
who has some condition unrelated to the heart or during the routine medical
examination of school children, or of candidates for the armed forces, superannuation or life insurance.
When there is evidence of cardiac enlargement or when a diastolic murmur
AUSCULTATION
is also heard, organic disease of the heart can be diagnosed with confidence
but frequently no other abnormality is present. In such cases attention to
detail, experience and commonsense are all important. The decision that a
murmur is innocent depends not only on the absence of any evidence of
organic heart disease but on the characteristics of the murmur itself.
The history is unlikely to be helpful in the type of case under consideration
because symptoms related to the heart will not be present. If there is an
unequivocal past history of rheumatic fever, more potential significance must
be attached to a murmur but so often a history of possible rheumatic fever
is inconclusive. Also a patient who has had rheumatic fever may have an
innocent murmur and it is well known that some 40 per cent. of all those
with unequivocal evidence of rheumatic heart disease give no history of
rheumatic fever.
The characteristic features of the various organic conditions associated
with a systolic murmur including valvular and congenital heart disease have
already been described.
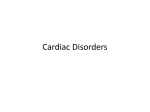
[]
PRE·SYSTOLIC MURMUR
EARLY DIASTOLIC
PAN·SYSTOLIC
MURMUR
DJ
MID·SYSTOLIC MURMUR
MURMUR
DJ
MID-DIASTOLIC MURMUR
LATE SYSTOLIC MURMUR
HEART MURMURS
The physician must make quite sure that there is no clinical evidence of
cardiac hypertrophy or enlargement, that there is no thrill, that the heart
sounds and the pulses are normal and that no diastolic murmur is present. If
there is any doubt about enlargement a radiograph should be taken.
Isolated systolic murmurs unassociated with any recognisable form of heart
disease may be loudest at the apex, at the base or at the left sterna} border.
In general it may be said that the louder the murmur the more likely is it
to be of organic origin and few murmurs louder than Grade 2-3 are innocent.
Also the harsher the murmur the more likely is it to be organic.
Innocent murmurs tend to be of relatively short duration and of high
frequency but inevitably the dividing line from organic murmurs is not sharp.
Also they tend to vary with respiration, posture and pressure of the
stethoscope on the chest wall more than do organic murmurs.
Late Systolic Murmur
A particular variety of innocent murmur is one which develops in late
systole shortly before the second heart sound, is loudest at the apex and may
amount to Grade 3 or more in intensity.
This characteristic murmur is of maximal intensity at the apex and just
RES MEDICA
before the second sound. The first part of systole is silent. The murmur may
be so loud and harsh that on this account it is often mistaken for organic heart
heart disease. It is therefore all the more important to recognise. Unfortunately,
as so often in medicine, there is no absolute rule and it is probable that a
late systolic murmur may occasionally be associated with organic mitral
incompetence, possibly with shortening of the chordae tendinae.
Pulmonary area
A pulmonary systolic murmur, loudest to the left of the upper sternum, is
a frequent finding especially in young people and in pregnancy. Presumably
it is due to blood flowing through the pulmonary valve but there is no
evidence of valvular stenosis, dilatation of the pulmonary artery or any other
abnormality.
Parasternal
These murmurs are usually of maximal intensity between the apex beat and
the sternal border and may be faint or loud, fine or coarse but are of short
duration and end about mid-systole. There will be no thrill or change in heart
sounds.
CLASSIFICATION OF DIASTOLIC MURMURS
EARLY
MID
Aortic incompetence or Pulmonary incompetence.
1.
2.
LATE
Mitral stenosis or Tricuspid stenosis
Increased flow
Mitral
Patent ductus arteriosus
Ventricular septal defect
Tricuspid
Atrial septal defect
Mitral or Tricuspid stenosis
PRE-SYSTOLIC MURMURS
In patients with sinus rh_ythm a pre-systolic murmur may be due to stenosis
of the mitral or tricuspid valves.
Mitral Stenosis
The classical physical signs of mitral stenosis are a loud slapping first heart
sound preceded by a pre-systolic murmur, and an opening snap followed by a
rumbling mid-diastolic murmur.
This cadence gives rise to the onomatopoeic "fftou ta ta rrou" first
described by Duroziez.
The first or pre-systolic element of this sequence occurs late in ventricular
diastole, synchronous with the forceful rapid passage of blood into the
ventricle produced by atrial systole. It is therefore only heard in patients with
sinus rhythm and disappears with the onset of atrial fibrillation.
This murmur is usually loudest at the apex and may be accompanied by a
thrill
An isolated pre-systolic murmur, that is without an associated mid-diastolic
murmur, is only found in the early or mild stages of mitral stenosis.
Tricuspid Stenosis
A pre-systolic murmur similar in quality to that of mitral stenosis may be
AUSCULTATION
31
heard in patients with tricuspid stenosis. This possibility should always be
considered in patients with mitral valvular disease, especially if the pre-systolic
murmur is well heard in the region of the sternum and is louder in deep
inspiration which increases blood flow across the valve. In such cases there is
likely to be a prominent ' a ' wave in the jugular venous pulse.
Occasionally a pre-systolic murmur is heard in patients with aortic incompetence but without mitral stenosis and has been called the Austin Flint
murmur after the man who first described it. The importance of this murmur
has been exaggerated and its mechanism of production is still disputed. It will
therefore not be discussed further.
MID-DIASTOLIC MURMURS
A mid-diastolic murmur may be heard in mitral or tricuspid stenosis or in
patients with increased blood flow across the valve without stenosis, i.e. with
an intracardiae shunt.
The most characteristic sign of mitral stenosis is a long rumbling middiastolic murmur, loudest at or localised to the apex. If, as is so often the case,
atrial fibrillation is present there will be no pre-systolic murmur but there
may be a loud first heart sound and an opening snap as already discussed.
Tbis murmur is best heard or may only be heard if the patient is lying
down and turned towards the left side or if blood flow is increased by exercise.
These manoeuvres, therefore, should be part of the routine examination of
any patient suspected of having valvular heart disease.
It used to be thought that a mid-diastolic murmur at the apex was diagnostic
of mitral stenosis but with the increased precision in auscultation which came
with phonocardiography and in particular with the stimulus to careful
auscultation brought by the advent of cardiac surgery, it has been recognised
that a murmur similar in time but usually different in quality may occur in
patients with congenital heart disease, associated with increased blood flow
across the mitral valve.
EARLY
DIASTOLIC
MURMURS
Au early diastolic murmur, i.e. one beginning immediately after the second
heart sound is characteristic of aortic or pulmonary valvular incompetence.
These two causes are not always easy to differentiate, the distinction, when
possible, being made not from the qualities of the murmurs but from consideration of associated features.
Aortic Incompetence
This is usually loudest in the 3rd and 4th intercostal space close to the left
sternal border. It may also be heard in the "aortic area" and, if loud, at the
apex. When the murmur is audible at the apex it can usually be appreciated
that there is no gap between the second heart sound and the beginning of the
murmur, in contrast to the mid-diastolic murmur of mitral stenosis when there
is a distinct gap and possibly an opening snap as discussed below.
The murmur is usually best heard with a diaphragm chest piece and with
the patient sitting up or standing and with the breath held in expiration. It
is well to remember these points if quiet murmurs are not to be overlooked.
The murmur of aortic incompetence is usually high pitched and blowing in
quality. If harsh or musical and especially if heard best to the right rather than
to the left of the sternum some cause other than rheumatic fever should be
considered such as syphilis, bacterial endocarditis or trauma.
32
RES MEDICA
Although, in general, a loud murmur will be associated with severe
incompetence there is no close correlation between these two features and
many striking discrepancies. The severity of valvular incompetence and
consequent regurgitation cannot in fact be assessed by auscultation but only
by examination of the peripheral circulation and by seeking evidence of left
ventricular hypertrophy. However, the signs of aortic incompetence are often
modified by associated valvular stenosis.
With free regurgitation there will be a full, bounding "water hammer or
Corrigan pulse and a low diastolic blood pressure with a high systolic pressure
and therefore a high pulse pressure. Exaggerated arterial pulsations may be
obvious in the carotid and other arteries and capillary pulsation in the nail
beds or retinal vessels. A pistol shot may be heard over a medium sized
vessel such as the brachial or femoral artery if the vessel is lightly compressed
with the bell of the stethoscope.
Pulmonary Incompetence
As early diastolic murmur from pulmonary incompetence was first described
by Graham Steele in a patient with severe pulmonary hypertension from
mitral stenosis. This murmur is similar in quality to that of aortic incompetence and likewise will be audible down the left sterna] border. It is impossible
to distinguish the two by auscultation and the probability as to which valve
is at fault must be decided by seeking signs of aortic regurgitation in the
peripheral circulation on the one hand and of pulmonary hypertension on
the other.
Pulmonary hypertension will be indicated by a loud second heart sound
and clinical or electrocardiographic evidence for right ventricular hypertrophy.
There will also be radiographic enlargement of the main pulmonary artery.
CONTINUOUS MURMURS
The most frequently heard continuous murmur is that due to patency of
the ductus arteriosus, a condition with which the student should be familiar.
The murmur is that of an arterio-venous fistula but the differential G L D J Q R V L V will not be discussed being the province of the specialist.
*
*
*
*
In the first part of this paper it was suggested that the recently introduced
Leathan modification of the Bowles stethoscope was probably best. Further
experience has shown that this model has certain defects and the student is
therefore advised to use the standard bell and diaphragm chest piece manuI D F W X U H G bv Messrs. Thackray of Leeds.