Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
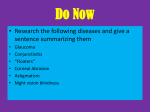
PJ, 04 Sep, p233-240 LandD_Layout 1 9/1/2010 2:20 PM Page 235 The Pharmaceutical Journal 235 Continuing professional development Care and advice for contact lens wearers It is believed that the idea of the contact lens came from Leonardo da Vinci and it took over 300 years before the concept was realised, in the form of a piece of blown glass that covered the whole white of the eye. Corneal contact lenses became available in 1936. By 2008, contact lenses were worn by around 3.5 million people in the UK. Marvyn Elton discusses salient points for pharmacists Marvyn Elton Most people wear contact lenses for their corrective function (eg, for myopia, hypermetropia or astigmatism) — lenses works by refracting light rays onto the retina — but the wearing of lenses for cosmetic purposes is becoming increasingly popular. Contact lenses lie on the cornea (see Panel 1, p236) and there are two main types: rigid gas permeable and soft. Types of contact lens Before the late 1970s, people wore contact lenses made of Perspex (polymethylmethacrylate or PMMA). These were the so-called hard lenses. When more modern materials (fluorocarbon or fluorosilicate materials) became available, the lenses were described as “rigid gas permeable” (RGP). RGP lenses do not fold and are typically smaller than the cornea, at around 9.0 to 9.6mm. Their material allows oxygen to diffuse through to the cornea. RGP lenses also move on the cornea and this allows the tear film to move. RGP lenses are useful if a person has a high prescription because thicker lenses can be used with relatively little danger to eye health. They also allow the best vision to be attained in conditions such as keratoconus (where the shape of the cornea is distorted) and can have a two to three year lifespan. Soft lenses are larger in diameter (about 14mm) than RGP lenses and completely cover the cornea so that the edge of the lens can be seen on the white of the eye (sclera). This type of lens is most commonly used because it is generally comfortable straight away and the fitting is easier and quicker. Soft lenses fold easily. They are hydrogels containing between 38 and 74 per cent water. The higher the water content, the softer and more comfortable the lens. High water content also results in greater oxygen permeability through the lens, so the healthier the lens is for the cornea. However, lenses with a higher water content have shorter lifespans and are more fragile. Most soft contact lens wearers wear daily, two-weekly or monthly disposable lenses (yearly lenses are becoming obsolete). Daily disposables are convenient because no cleaning or disinfection is required but they are very thin and are not as easy to handle as a monthly disposable lens, which contains more water so is thicker (which also tends to result in better vision and more comfort). A few monthly disposables are “extended wear”. They are made from silicone hydrogel and marketed for 30-day wear, 24 hours a day, including during sleep. These lenses feel greasy and, in my opinion, the visual acuity is not as good as with the conventional monthly disposables. Extended wear soft lenses first became available in the 1980s but they were linked to increasing rates of corneal infection and withdrawn. In 2001, silicone hydrogel extended wear lenses became available. It was hoped that there would be a reduction in the level of corneal infection compared with the older extended wear lenses but this has not been the case. Two studies carried out in Australia and New Zealand and one casecontrol study from Moorfields Eye Hospital, London, demonstrated no difference in the risk of corneal infection between the older and the newer extended wear lenses and indicated an increased risk of infection with overnight wear.1 (I do not fit 24 hour soft lenses because I am worried about corneal vascularisation and infection — see later.) Cleaning and disinfecting Most contact lenses require daily cleaning and disinfection to remove bacteria and deposits, such as protein and lipids, which can decrease visual acuity, damage the lens and pose a risk to eye health. Cleaning contact lenses used to be a process that required a number of steps and a number of products, such as a cleaner, a disinfectant, a product to neutralise the disinfectant and a protein remover. This complicated regimen, which could be difficult to follow correctly, has now been replaced with simpler one- or two-step systems. Contact lens solutions are classed as medical devices and all products meeting EU standards will bear a CE mark. RGP lenses Most RGP cleaning regimens involve a cleaning solution containing a surfactant, and a conditioning and disinfecting solution. Conditioning and disinfecting solutions contain ingredients such as polyhexamethylene biguanide (PHMB; also known as polyhexanide, polyaminopropyl biguanide and Dymed). PHMB is a broad spectrum antibacterial. It is bacteriostatic at low concentrations but is rapidly bactericidal at higher concentrations. It kills bacteria by causing an irreversible loss of essential cellular Reflect Plan Evaluate Act REFLECT 1 What is the treatment for Pseudomonas aeruginosa infection of the cornea? 2 What types of contact lens solutions are available? 3 Can you list three possible drug-contact lens interactions? Before reading on, think about how this article may help you to do your job better. components as a direct consequence of cytoplasmic membrane damage. Before inclusion in contact lens products, PHMB was used in the food, brewing and dairy industry. It was also used as a swimming pool disinfectant. PHMB is a long-chain polymer (molecular weight 1,300 compared with the 359 of chlorhexidine). The RGP lens is removed from the eye and placed in the palm of the hand. A few drops of cleaning solution are then placed in the palm and the lens is rubbed for about 30 seconds to help the cleaning process. The contact lens case is then filled with the conditioning and disinfecting solution and the lens is stored in the case for at least six hours The author Marvyn Elton, MCOptom, MRPharmS, is an optometrist practising in London and Essex (Vol 285) 4 September 2010 www.pjonline.com PJ, 04 Sep, p233-240 LandD_Layout 1 9/1/2010 2:29 PM Page 236 236 The Pharmaceutical Journal Learning & development (usually overnight). After disinfection, the wearer rinses the lenses with the conditioning and disinfecting solution before putting them in. The solution in the contact lens case should be thrown away and the case left to air dry. It is important to stress that conditioning and disinfecting solutions must be used after cleaning because there have been instances where people have cleaned an RGP lens and put it straight into the eye, resulting in a corneal abrasion and pain. In such cases, the eye should be washed out with 0.9 per cent saline or water, and a visit paid to an optometrist. Soft lenses Soft contact lenses that are reworn should be cleaned daily. Conventional monthly disposables are generally not old enough for deposits to build up but bacteria must be removed. There are two main types of cleaning and disinfecting product: hydrogen peroxide based and multipurpose. When recommending a solution an optometrist will consider the patient’s history, the lens to be worn and the likelihood of patient compliance. Teenagers, for example, can be lax with cleaning and disinfecting steps so a multipurpose solution might be preferred. Extended wear lenses do not require cleaning or disinfecting but if wearers wish to do so soft lens solutions can be used. Hydrogen peroxide The antimicrobial properties of hydrogen peroxide (H2O2) have been well known since its discovery in 1818. A 3 per cent solution was introduced as a method of disinfection for soft contact lenses in the early 1970s (as an alternative to boiling) and this is still considered to be the most effective disinfecting agent for soft contact lenses because it is able to kill large numbers of microorganisms quickly, including pseudomonas and acanthamoebae.2 However, the peroxide must be neutralised before the lenses can be worn (a neutralising tablet is placed in the contact lens container, producing water and oxygen). Forgetting to neutralise the peroxide is a danger and, along with the inconvenience of neutralisation, has reduced the use of peroxide systems. Multipurpose solutions Most soft lens wearers now use a single solution, which both cleans and disinfects. The lens is cleaned in the same way as an RGP (rubbing has been shown greatly to reduce the bacterial contamination). Some multipurpose solutions with a “no rub” feature are now available, but I still advise the soft lens wearer to rub both sides of the contact lens when cleaning. The contact lens case is filled with the solution and the lenses placed in it for overnight disinfection (or for a minimum of four hours). When the lenses are removed from the case they can be rinsed with the solution and worn. Multipurpose solutions generally contain: • A cleaning agent (a surfactant, such as poloxamer, tyloxapol or poloxamine, to stop protein and bacteria adhering to lenses) 4 September 2010 (Vol 285) www.pjonline.com PANEL 1: ANATOMY OF THE CORNEA The cornea is at the front of the eye. It is about 12mm in diameter and covers the iris. A healthy cornea is transparent and convex. The cornea is the main structure for bending the light rays to a focus on the retina, contributing about 70 per cent of the refracting power of the eye. Average corneal thickness is 550μm. The cornea consists of five layers. The outermost layer, as with all tissues, is the Light micrograph of outer corneal layers (Herve Conge ISM/SPL) epithelium. This is usually between 70 and 100μm thick. Underneath the epithelium is Bowman’s membrane. Below this is the stroma, which is the thickest corneal layer, and under this is Descemet’s membrane. The innermost layer is the endothelium. This is in direct contact with the aqueous fluid in the eye and continually pumps out fluid from the cornea, maintaining corneal transparency. The cornea is rich with nerve fibres (so corneal damage or infection can be extremely painful). Tear film keeps the cornea (and the conjunctiva) moist and this is necessary for corneal integrity and health. • A disinfectant • A moisturising or conditioning agent, which adheres to the lens surface (“wetting”) thus making it more comfortable to wear • Buffers and preservatives (solution discard dates can range between two and six months after opening) ISO/DIS 14729, the standard for the antimicrobial efficacy of soft lens care products, requires the solutions to demonstrate the required log reduction against three bacteria and two fungi. The primary standard for disinfection requires a 1 million organisms/ml challenge (6 log units) and for the organisms to be killed to the following levels: • Bacteria 99.9 per cent (3 log) reduction within the stated soaking time for Staphylococcus aureus, Pseudomonas aeruginosa and Serratia marcescens • Fungi 90 per cent (1 log) reduction within the stated soaking time for Candida albicans and Fusarium solani Common disinfectants used in multipurpose solutions include PHMB (eg, Complete Multi Purpose, ReNu) and polyquad. PHMB is effective at concentrations of 0.00003–0.0001 per cent Check your learning available online until 4 October 2010 www.pjonline.com/check and at such low levels the risk of adverse ocular reactions is minimised. Polyquad (also called polyquaternium-1) has a molecular weight of 5,000 so tends not to diffuse into the lens matrix. This minimises hypersensitivity reactions.3 Polyquad is a less potent antimicrobial than PHMB so is used in higher concentrations (0.001–0.01 per cent). It performs relatively poorly against fungi and acanthamoebae. (In Opti-Free Express solution, this problem is addressed by the addition of myristamidipropyl dimethylamine [MAPD]). Water Tap water must never be used in lens cleaning regimens, storage or in contact lens cases. This is because it contains sight-threatening microorganisms, such as acanthamoebae. Contact lens cases should be rinsed out with contact lens solutions and not tap water. Furthermore, I would not recommend wearing contact lenses in the shower or during swimming. Swimming while wearing swimming goggles over the contact lenses may be acceptable. Prescription swimming goggles are available. Switching solutions With so many apparently similar products available, consumers may wish to switch between products. It is my opinion that, in general, there should be no problem with changing to another multipurpose solution but pharmacists selling these products should advise the person to ensure that he or she complies with the instructions for use on the pack. It is worth noting, however, that the College of Optometrists advises the public not to switch solutions unless advised by their optometrist. Different solutions do contain different ingredients and at varying PJ, 04 Sep, p233-240 LandD_Layout 1 9/1/2010 2:20 PM Page 237 The Pharmaceutical Journal 237 Continuing professional development Corneal vascularisation Figure 1: small corneal abrasion (Marvyn Elton) Figure 2: mild acanthamoeba keratitis (Karl Southerton, Western Eye Hospital) concentrations and some patients may find a particular solution more compatible with their eyes than others. Moreover, some solutions have been found to stain certain lens materials.3 The ideal contact lens solution would kill all pathogens that can infect the eye and effectively remove deposits, and be non-toxic, easy to use and affordable. Eye health Contact lens wearers are at increased risk of eye infections and other ocular problems and pharmacists must be aware of this. If a lens wearer complains of an uncomfortable or painful eye, or the eye is red, or both, lenses must not be worn until symptoms resolve. Corneal abrasions and erosions If, when putting a lens in the eye or taking it out, the wearer’s fingernail or edge of an RGP lens accidently catches the cornea, this can cause a corneal abrasion (see Figure 1). Corneal abrasions are usually painful and can take a few days to heal. Once a person has had a corneal abrasion, they are at greater risk of recurrent corneal erosions. These erosions typically cause eye pain on waking in the morning (when we sleep the eye becomes drier and on opening the eyes, the eyelid pulls on the cornea causing an erosion and giving rise to severe pain). Optometrists can assess corneal disturbances with fluorescein, an orange dye that glows green under blue light (see Figure 1). I usually treat the pain of a corneal abrasion with 1 per cent cyclopentolate eyedrops to relax the iris and prevent iris spasm in response to light. The patient can also be given single use drops (eg, Minims) to use two or three times a day. A combination of the oxygen diffusible material in RGP lenses and tear film movement allows sufficient oxygen to get to the cornea from the air so wearers are not at risk of hypoxia in the eye. In contrast, soft lenses hardly move on the cornea — they generally grip onto the front of the eye so do not allow the tear film to circulate. In addition, soft lens material is not as oxygen permeable as RGP lens materials and, as a result, soft lens wearers have less oxygen reaching the cornea. If the lenses are worn too much the resulting hypoxia causes blood vessels to grow into the cornea from the limbus (the corneoirido junction). Corneal vascularisation is usually most prominent in the 10 o’clock to 2 o’clock positions around the iris. If one or more blood vessels extends 2mm into the cornea, the wearing time of the soft lens must be reduced. The danger of corneal vascularisation is that the blood vessels will continually grow and eventually reach the pupillary area, causing blindness. (I have seen a couple of cases of vascularisation causing blindness.) People wearing soft lenses most of the time (eg, five days a week and 12 hours a day), must have regular aftercare (ideally every six months) from their optometrist. Aftercare appointments involve the optometrist checking vision with the lenses but, most importantly, looking at the front of the eyes for corneal vascularisation. (If a soft lens wearer does not attend six-monthly aftercare appointments, I refuse to supply any more contact lenses.) Microbial keratitis The worst complication associated with contact lens wear is inflammation of the cornea (keratitis) caused by pathogens. Microbial keratitis can easily lead to blindness, even with treatment. The two worst organisms to infect the eye are Pseudomonas aeruginosa and acanthamoeba. The wearing of soft contact lenses is a big risk factor for pseudomonas and acanthamoeba corneal infection but the wearing of RGP lenses does not rule out infection. As well as improper contact lens care, overnight wearing of contact lenses is a major risk factor. Pseudomonas Pseudomonas aeruginosa is a Gram negative aerobic rod, measuring 0.5–0.8µm by 1.5–3.0µm. Nearly all strains are motile by means of a flagellum. Pseudomonas is commonly found in water and soil. It can also grow in distilled water. The bacterium is an opportunistic pathogen, exploiting some break in host defences. It can infect any tissue in the body as long as the tissue defences are compromised. It is also a common nosocomial pathogen. A patient presenting with a pseudomonas keratitis will commonly be a soft lens wearer. Inflammation is usually unilateral. The eye will typically be painful and red. Because of the eye pain, the eyelid will be shut and there will be a lot of watering. (It can be difficult to examine the front of the eye because the patient will want to keep the eye closed.) On examination, an optometrist would usually see a small, round, white opacity near the edge of the cornea. This is a corneal ulcer (also known as ulcerative keratitis or, when due to pseudomonas, pseudomonas keratitis). About 30 per cent of corneal ulcers are associated with wearing contact lenses. Bacteria can colonise the lens storage case or the lens itself. During contact lens wear, pathophysiological changes in the corneal epithelium occur, decreasing the defence capability of the eye. Bacteria can adhere to the contact lens and, when the lens is placed on the eye, detach from it and invade the compromised epithelium. If untreated, the bacteria will invade the underlying corneal layers and cause a full thickness corneal ulcer. The higher risk of disease in overnight lens wear has led to the speculation that contact lens induced corneal hypoxia predisposes contact lens wearers to a greater rate of corneal infection because of compromised corneal epithelial integrity, impaired wound healing and an increased susceptibility of corneal epithelial cells to bacterial binding.1 Patients diagnosed with microbial keratitis are admitted to hospital because hourly instillation of antibiotic eye-drops is required to try to control the infection — if the patient falls asleep (which may be unlikely due to the pain) a nurse will wake him or her up to instil the drops. Chloramphenicol eye-drops are ineffective against Pseudomonas aeruginosa and fluoroquinolones, such as ofloxacin or ciprofloxacin, are commonly prescribed. The hourly instillation of the drops may be necessary for weeks. Only once the infection is under control, is the dosage tapered. Gentamicin eye-drops can be used but, again, hourly instillation is required. Prednisolone eye-drops can be used (eg, one drop three times a day) for inflammation once the infection is under control. It is important not to use a steroid drop before this stage because steroids can exacerbate corneal ulcers and worsen infections. Even if treatment is successful, a corneal scar can be left. If this is in front of the pupil, vision will be reduced or the eye will be blind. Acanthamoeba Acanthamoeba is an amoeba Marvyn Elton will be available to answer questions online on the topic of this article until 20 September 2010 Ask the expert www.pjonline.com/ask-expert found in water and soil. Acanthamoeba species have two stages in their life cycle, a trophozoite stage that feeds on bacteria and fungi (if a lens storage case has become contaminated with pseudomonas, acanthamoebae can feed on it) and a nondividing cyst stage, which is resistant to stress. Wearing soft contact lenses is the most common risk factor for development of (Vol 285) 4 September 2010 www.pjonline.com PJ, 04 Sep, p233-240 LandD_Layout 1 9/1/2010 2:29 PM Page 238 238 The Pharmaceutical Journal Learning & development New and future technologies PANEL 2: CASE REPORTS 1. A 19-year-old man presented with a five-day history of red, painful eyes and he could not see. On examination, he had large corneal ulcers in both eyes; these were located in the central cornea rather than the corneal periphery (see Image), explaining the patient’s blindness. The patient was admitted to hospital for hourly instillation of ofloxacin eye-drops. Corneal epithelial scrapes confirmed that Pseudomonas aeruginosa and acanthamoebae were present. The patient was started on hourly PHMB 0.02 per cent eye-drops and propamidine 0.1 Large corneal ulcer (Karl Southerton, Western Eye Hospital) per cent drops in addition to the ofloxacin. Within a few days, both eyes became more comfortable, the ulcers were reducing in size and vision in both eyes improved. This patient was fortunate to regain normal visual acuity because, in some cases, corneal scars can cause permanent blindness. His case is of interest because he wore daily disposable lenses. On questioning, he said that he was reusing the lenses after disinfecting them. The disinfecting solution and the contact lens case were not available for analysis. It emphasises that even when a patient wears daily disposables, it is worth checking that these are not being misused. 2. A 34-year-old man presented with a three-day history of a red, painful right eye and blurred vision. On examination, there was mild disturbance of the cornea; that is, there were corneal epithelial erosions but no ulceration. However, because the eye was painful and the patient was a soft contact lens wearer he was assumed to have an early bacterial keratitis and started on ofloxacin eye-drops six times a day, prescribed in case Pseudomonas aeruginosa was present. Two days later there was no improvement in his symptoms; the corneal erosions were still present but were more linear and dendritic in appearance. The patient was thought to have a herpes simplex keratitis and was treated with aciclovir eye ointment five times a day. When there was still no improvement the following week, acanthamoeba keratitis was suspected. The patient was admitted to hospital and started on PHMB 0.02 per cent and propamidine 0.1 per cent eye-drops hourly. A corneal epithelial scrape confirmed the presence of acanthamoebae. There was good response to the treatment and as the eye improved the drops were tapered. On questioning this patient revealed that he was using tap water in his contact lens case. This case also shows how early acanthamoeba keratitis can look like a herpes simplex keratitis. acanthamoeba keratitis — 80–90 per cent of cases are contact lens wearers. Patients typically present with a red, painful eye (see Figure 2, p238), which he or she will try to keep closed. Like a pseudomonas keratitis, acanthamoeba keratitis is an ocular emergency, requiring hospital admission for hourly instillation of eye-drops and specialist attention. Polyhexamethylene biguanide (PHMB) 0.02 per cent eye-drops (eg, from Moorfields Pharmaceuticals) are used. Propamidine can also be used with the PHMB. As the keratitis improves, the dosage of the eye-drops can be tapered. The bottom line is that if a contact lens wearer complains of a red, painful eye chloramphenicol eye-drops or ointment must not be supplied. If the person wears soft contact lenses, alarm bells should ring loudly. In such cases the best action would be to send the person to an optometrist or eye casualty in hospital to rule out a pseudomonas or acanthamoeba infection. The pharmacist could write a letter to this effect for the patient to take. Topical chloramphenicol is ineffective against these two micro-organisms. I describe two cases in Panel 2. 4 September 2010 (Vol 285) www.pjonline.com Drug-lens interactions Pharmacists will be aware that many eyedrops cannot be used while wearing soft contact lenses because of the risk of adsorption of ingredients, typically preservatives such as benzalkonium chloride, onto them. Lenses should not be worn for the duration of treatment or preservative-free drops used, although, according the British National Formulary, RGP lenses can be worn. Eye ointments should not be used with contact lenses and oily eye-drops should be avoided. Consequences of drug-lens interactions include eye discomfort, contact lens damage and toxic interactions. Examples of interactions include: • Increased deposits (eg, with dopamine) • Lens discoloration (eg, with rifampicin and sulfasalazine) • Lens dehydration (eg, with isotretinoin) • Corneal oedema (eg, with oral contraceptives, especially high strength oestrogens) • Reduced blink reflex and eye movement (eg, with tricyclic antidepressants) • Reduced tear production (eg, with sedating antihistamines) An example of a recent advance in contact lens practice is orthokeratology (ortho-K), which uses specially designed RGP lenses, worn during sleep, to reshape the cornea. When removed in the morning, vision is corrected and there is no need for glasses or contact lenses during the day. Research into the field of contact lenses, new materials and new solutions continues. Pharmacists might be interested to know that there has also been research into the possibility of using contact lenses for drug delivery (eg, lens wear might enable glaucoma medicines to be given for up to 30 days).4 Signposting • The British Contact Lens Association website (www.bcla.org.uk) contains answers to frequently asked questions. • “Look after your eyes” (www.lookafteryoureyes. org), run by the College of Optometrists, explains common eye health issues. Resources • For further details of drug-lens interactions, read GL Muntigh’s “Drug and contact lens interactions” in SA Family Practice (2005;47:24–28). References 1 Stapleton F, Keay L, Jalbert I, Cole N. The epidemiology of contact lens related infiltrates. Review. Optometry and Visual Science 2007;84:4. 2 Griffiths H. Soft contact lens care products: an update. Optometry in Practice 2003;4:31–42. 3 Atkins N. Developments in lens care solutions. Optician 2006;231:6037. 4 Bowers Ciolino J, Hoare TR, Iwata NG, Behlau I, Dohlman CH, Langer R et al. A drug-eluting contact lens. Investigative Ophthalmology and Visual Science. Available at www.iovs.org (accessed on 23 August 2010). CPD articles are commissioned by The Journal and are not peer reviewed. PRACTICE POINTS Reading is only one way to undertake CPD and the regulator will expect to see various approaches in a pharmacist’s CPD portfolio. 1 Do you know your local opticians? FInd out how they might like you to refer people with eye problems requiring investigation with a slit lamp. 2 How would you advise a person wanting to switch multipurpose solutions? Use the article by Atkins N (reference 3) to inform your decision. 3 Make sure your staff are trained on the correct sale of chloramphenicol and how to deal with contact lens wearers. Consider making this activity one of your nine CPD entries this year.