Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
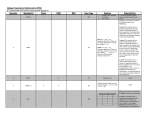
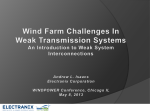
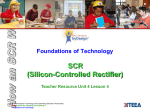
Supplemental Table 1 Inclusion and Exclusion Criteria for the AVOID-HF Trial Inclusion Criteria 1. Age ≥ 18 years 2. Male or non-pregnant female patients 3. Admitted to the hospital with a primary diagnosis of acutely decompensated HF 4. On regularly scheduled daily oral loop diuretics 5. Fluid overload manifested by at least two of the following: a. Pitting edema ≥ 2+ of the lower extremities b. Jugular venous distention > 8 cm c. Pulmonary edema or pleural effusion on chest x-ray d. Paroxysmal nocturnal dyspnea or ≥ two- pillow orthopnea e. Respiration rate ≥ 20 per minute. 6. Have received ≤ 2 IV loop diuretics doses before randomization 7. Must be able to be enrolled into the trial ≤ 24 hours of their admission to the hospital 8. Provide written informed consent form as required by the local IRB Exclusion Criteria 1. Acute coronary syndromes 2. Renal insufficiency with a sCr ≥ 3.0 mg/dl or planned renal replacement therapies 3. Systolic blood pressure < 90 mmHg at time of enrollment 4. Pulmonary Arterial Hypertension not secondary to left heart disease 5. Contraindications to systemic anticoagulation 6. Hematocrit > 45% 7. Inability to obtain venous access 8. Hemodyanmic instability severe enough to require IV positive inotropic agents, IV vasodilators or both 9. Use of iodinated radiocontrast material within the previous 72 hours or planned study requiring IV contrast during the current hospitalization 10. Severe concomitant disease expected to prolong hospitalization 11. Severe concomitant disease expected to cause death in ≤ 90 days 12. Sepsis or ongoing systemic infection 13. Severe uncorrected valvular stenosis 14. Active myocarditis 15. Hypertrophic obstructive cardiomyopathy 16. Constrictive pericarditis or restrictive cardiomyopathy 17. Liver cirrhosis 18. Previous solid organ transplant 19. Requirement for mechanical ventilatory support 20. Presence of a mechanical circulatory support device 21. Unwillingness or inability to complete follow up 22. Active drug or alcohol abuse 23. Participation in another clinical trial 1 Supplemental Table 2 Secondary End-Points of the AVOID-HF Trial I. Efficacy a. Total fluid removed during the index hospitalization b. Net fluid removed during the index hospitalization c. Weight loss at 72 hours after randomization d. Total weight loss during the index hospitalization e. Time to freedom from congestion, freedom from congestion is defined as i. jugular venous distention of < 8 cm ii. no orthopnea t iii. race peripheral edema or no edema f. Freedom from congestion, defined as i. jugular venous distention of < 8 cm ii. no orthopnea iii. trace peripheral edema or no edema at hospital discharge g. Changes in B-type natriuretic peptide (BNP) levels over time (72 hours, discharge, 30, 60 and 90 days) II. Clinical a. Length of stay (LOS) during the index hospitalization b. Total number of days re-hospitalized for HF at 30 and 90 days after discharge c. Total number of Emergency Department (ED) or unscheduled office visits requiring IV therapy for HF , including diuretics and/or positive inotropic agents and/or vasodilators at 30 and 90 days after discharge d. Total number of HF re-hospitalizations at 30 and 90 days after discharge e. Total number of cardiovascular (CV) re-hospitalizations at 30 and 90 days after discharge f. Total number of days for CV re-hospitalizations at 30 and 90 days after discharge g. All cause re-hospitalization rates at 30 and 90 days h. Mortality rates up to 90 days after randomization i. j. Days alive and out of hospital at 30 and 90 days after discharge Quality of life assessed using the Kansas City Cardiomyopathy Questionnaire (KCCQ) at 30-, 60- and 90-days after discharge k. Global clinical score at 30 and 90 days after discharge III. Safety a. Changes in renal function variables after treatment up to 90 days after randomization i. serum creatinine (sCr) ii. blood urea nitrogen (BUN) iii. BUN/sCr iv. glomerular filtration rate (eGFR) estimated with the Modification of Diet in Renal Disease(MDRD) formula 2 Supplemental Table 3 Treatment Guidelines for the Loop Diuretic Arm The goal of therapy is for the patient to reach dry weight and rapidly transition to oral medications suitable for outpatient therapy. A. At Randomization UO > 5 L/day → Reduce current diuretic regimen if desired UO 3-5 L/day → Continue current diuretic regimen UO < 3 L/day → See table Current Dose Suggested Dose Loop (/day) thiazide Loop (/day) thiazide A ≤ 80 + or 40 mg IV bolus+5 mg/hr 0 B 81-160 + or 80 mg IV bolus+10 mg/hr) 5 mg metolazone QD C 161-240 + or 80 mg IV bolus + 20 mg/hr 5 mg metolazone BID D > 240 + or 80 mg bolus + 30 mg/hr 5 mg metolazone BID “Loop” refers to IV furosemide. 1 mg bumetanide or 10 mg torsemide = 40 mg furosemide B. At 24 Hours Persistent Volume Overload Present UO > 5 L/day → Reduce current diuretic regimen if desired UO 3-5 L/day → Continue current diuretic regimen UO < 3 L/day → Advance to next step on table C. At 48 Hours Persistent Volume Overload Present UO > 5 L/day → Reduce current diuretic regimen if desired UO 3-5 L/day → Continue current diuretic regimen UO < 3 L/day → Advance to next step on table and consider: a) IV inotropes if SBP < 110 mmHg and EF<40% or RV systolic dysfunction. b) Nitroglycerin or Nesiritide if SBP > 120 mmHg (any EF) and Severe Symptoms D. At 72 Hours Persistent Volume Overload Present UO > 5 L/day → Reduce current diuretic regimen if desired UO 3-5 L/day → Continue current diuretic regimen UO < 3 L/day → Advance to next step on table and consider: a) IV inotropes if SBP < 110 mmHg and EF<40% or RV systolic dysfunction. b) Nitroglycerin or Nesiritide if SBP > 120 mmHg (any EF) and Severe Symptoms c) Right Heart Catheterization E. Repeat 72 hour step until treatment complete F. Patient evaluation guideline a. Every 6 hours evaluate recent BP, HR, UO, Net intake/output b. Every 12 hours evaluate serum chemistries G. Consider Decreasing or Holding Diuretic Dose if: a. sCr rises by >30% or 0.4 mg/dl (whichever is less) compared to prior measurement b. Resting SBP decreases > 20mmHg compared to prior 6 hours or drops <80mmHg c. Resting HR >30bpm compared to prior 6 hours or > 120 bpm H. Consider Completion of Therapy if ONE of the following: 1. Resolution of congestion (all of following): 3 a. Jugular venous pressure <8cm H20 b. No orthopnea c. Trace or no peripheral edema 2. Best Achievable “Dry Weight” has been reached a. Hemodynamic evidence of poor tolerance of fluid removal by persistent hemodynamic changes AND b. Net negative <1 liter/24hr 3. Persistent elevation in sCr >1.0 mg/dl above baseline at start of IV Diuretic Treatment 4. Persistent hemodynamic instability I. After Completion of IV Loop Diuretic Therapy: 1. If satisfactory “dry weight” has been reached AND sCr is stable: b. Initiate oral loop diuretics with goal to keep net even (new dose of loop diuretics may be less than baseline dose in some patients) c. GDMT 2. If sCr, hemodynamics, or UO are NOT stable: a. Hold diuretics until creatinine is stable for minimum of 12 hours, and then initiate oral diuretics as above b. If elevated sCr or hemodynamic instability persist, then consider bolus of IV fluid Abbreviations: BID: twice daily; BP= Blood Pressure; BPM=Beats per Minute; EF=Ejection Fraction; GDMT: Guidelines Determined Medical Therapy; HR= Heart Rate; IV=Intravenous; QD=once daily; RV=Right ventricle; SBP= Systolic Blood Pressure; sCr= serum creatinine level; UO= Urine Output. 4 Supplemental Table 4 Treatment Guidelines for the Aquapheresis Arm General Comments: 1. Once an initial UF rate is chosen, avoid increasing the UF rate unless there are clear indications to do so. 2. Because patients’ plasma refill rate usually declines as fluid is removed, it should be expected that UF rate will need to be decreased during the course of therapy. A. Choose Initial UF Rate: SBP <100mmHg: 150cc/hr SBP 100-120mmHg: 200cc/hr SBP >120mmHg: 250cc/hr B. Decrease starting UF rate by 50cc/hr if any of the following are present: a. RV > LV systolic dysfunction b. sCr increase 0.3mg/dl above recent baseline c. Baseline sCr > 2.0mg/dl d. History of instability with diuresis or UF in the past C. Re-evaluate UF. rate every 6 hours: 1. Evaluate recent BP, HR, UO, Net intake/output, sCr 2. Consider decreasing Aq. by 50cc/hr and checking STAT sCr (unless sent in past 2 hours) if: a. sCr rise >15% or >0.2mg/dl (whichever is less) compared to prior measurement b. resting SBP decreases > 10mmHg compared to prior 6 hours, but remains >80mmHg c. UO drops > 50% compared to prior 6 hours, but remains >125cc/6hr d. resting HR increases by >20bpm compared to prior 6 hours, but remains <120bpm 3. Strongly consider holding UF and checking STAT sCr if: a. sCr rise by >30% or >0.4mg/dl (whichever is less) compared to prior measurement b. resting SBP decreases > 20mmHg compared to prior 6 hours or is < 80mmHg c. UO < 125cc/6hr d. resting HR increases by 30bpm compared to prior 6 hours or is >120bpm 4. If UF held, re-evaluate after laboratory values are available: a. If hemodynamics are stable and sCr has plateaued, then consider re-starting UF at rate 50-100cc/hr less than previous rate b. If persistent volume overload is present, then consider: i. IV inotropes in patients with LVEF < 40% or RV systolic dysfunction ii. Weaning venodilators, especially in patients with HFpEF iii. Right heart catheterization D. Consider completion of UF therapy If ONE of the following occurs: 1. Resolution of congestion (all of following): a. Jugular venous pressure <8cm H20 b. No orthopnea c. Trace or no peripheral edema 2. Best Achievable “Dry Weight” has been reached a. Evidence of poor tolerance of fluid removal AND b. UF rate <100cc/hr or net negative <1 liter/24hr 3. Persistent elevation in sCr >1.0 mg/dl above baseline at start of UF treatment 5 4. Persistent hemodynamic instability E. After completion of UF Therapy: 1. If satisfactory “dry weight” has been reached AND sCr is stable: a. Initiate oral loop diuretics with goal to keep net even (new dose of loop diuretics may be less than baseline dose in some patients) b. GDMT 2. If sCr, hemodynamics, or UO are NOT stable: a. Hold diuretics until sCr is stable for minimum of 12 hours, then: i. If “Dry Weight” /adequate decongestion has been reached then initiate oral diuretics as above ii. If “Dry Weight”/adequate decongestion has NOT been reached then initiate IV diuretics a. If elevated sCr or hemodynamic instability persist, then consider bolus of IV fluids Abbreviations: BP= Blood Pressure; BPM=Beats per Minute; GDMT= Guidelines Directed Medical Therapy; HR= Heart Rate; IV=Intravenous; LV= Left Ventricle; RV=Right ventricle; SBP= Systolic Blood Pressure; sCr= serum creatinine level; UF= Ultrafiltration; UO=Urine Output. 6 Supplemental Table 5 Change of Quality of Life According to the Kansas City Cardiomyopathy Questionnaire From Baseline to 30, 60 and 90 days of Follow Up after Discharge Interval Baseline 30 Days P Value* 60 Days P Value* 90 Days P Value* AUF N=107 25.4±19.4 (0-92) N=85 31.0±24.3 (0-92) < 0.001 N=76 34.0±21.5 (0-83) < 0.001 N=72 36.0±23.0 (0-100) < 0.001 ALD N=110 28.6±22.6 (0-100) N=90 26.1± 23.0 (0-100) < 0.001 N=72 31.4±22.4 (0-92) < 0.001 N=76 33.6±23.0 (0-92) < 0.001 P Value 0.433 (a) 0.182 (a) 0.450 (a) 0.558 (a) a: P-value is from Wilcoxon's rank-sum test. *b: P-value is testing difference from baseline and from Wilcoxon's rank-sum test. 7 Supplemental Table 6 Change in Global Clinical Score from Baseline to 30, 60 and 90 Days Follow-up after Discharge Interval AUF ALD P Value Baseline N=107 N=110 0.122 (a) 28.3±18.6 31.8±18.6 (2-80) (0-76) N=85 N=91 28.2±20.1 25.4± 18.1 (0-70) (0-77) P Value* < 0.001 < 0.001 60 Days N=76 N=72 31.6±20.3 28.0±20.3 (1-78) (1-85) P Value* < 0.001 < 0.001 90 Days N=72 N=76 31.6±20.4 30.6±21.1 (1-79) (0-86) < 0.001 < 0.001 30 Days P Value* 0.449 (a) 0.197 (a) 0.697 (a) a: P-value is from Wilcoxon's rank-sum test. *b: P-value is testing difference from baseline and from Wilcoxon's rank-sum test 8 Supplemental Table 7 Number of Subjects with at Least One Serious Adverse Event Related to Study Therapy by MedDRA System Organ Class and Preferred Term MedDRA System Organ Class MedDRA Preferred Term AUF (N=110) ALD (N=111) P-value 16 (14.55%) 6 ( 5.41%) 0.026 CARDIAC FAILURE 0 (0.0%) 3 (2.7%) 0.246 CARDIO-RESPIRATORY ARREST 1 (0.9%) 0 (0.0%) 0.498 GASTROINTESTINAL DISORDERS GASTROINTESTINAL HAEMORRHAGE 2(1.8%) 0(0. 0%) 0.247 INFECTIONS AND INFESTATIONS INFECTION 1(0.9%) 0(0.0%) 0.498 INVESTIGATIONS BLOOD CREATININE INCREASED 1(0.9%) 0(0.0%) 0.498 CARDIAC OUTPUT DECREASED 1(0.9%) 0 (0.0%) 0.498 DEHYDRATION 1(0.9%) 0(0.0%) 0.498 HYPERKALAEMIA 1(0.9%) 0(0.0%) 0.498 NERVOUS SYSTEM DISORDERS NEUROLOGICAL SYMPTOM 1(0.9%) 0(0.0%) 0.498 RENAL AND URINARY DISORDERS HAEMATURIA 1(0.9%) 0 (0.0%) 0.498 RENAL FAILURE ACUTE 2(1.8%) 2(1.8%) >0.999 RENAL FAILURE CHRONIC 2(1.8%) 0(0.0%) 0.247 DEEP VEIN THROMBOSIS 1(0.9%) 0(0.0%) 0.498 HYPOTENSION 2 (1.8%) 1(0.9%) 0.622 SERIOUS ADVERSE EVENTS RELATED TO STUDY PRODUCT CARDIAC DISORDERS METABOLISM AND NUTRITION DISORDERS VASCULAR DISORDERS N includes all randomized and treated subjects. P-value is based on two randomized arms. P-value is from Fisher's Exact test. 9 Supplemental Figure 1 Supplemental Figure 1: Flow of subjects through the study protocol. 10 Proportion of Patients alive and free of HF Supplementary Figure 2 Time to HF Event or Death after Discharge 1.00 0.98 0.96 0.94 0.92 0.90 0.88 0.86 0.84 0.82 0.80 0.78 0.76 0.74 0.72 0.70 0.68 0.66 0.64 0.62 0.60 0.58 0.56 0.54 0.52 0.50 AQ LD 0 10 20 30 40 50 60 70 80 90 Time to HF event or death (days) AUF 105 ALD 108 81 75 52 50 20 16 Supplementary Figure 2 Legend: Supplemental Figure 2: Log rank analysis of the time to first heart failure event or death from any cause after discharge from index hospitalization up to 90 days in the AUF (squares) and ALD (triangles) groups. The difference between groups was not statistically significant (p=0.297) due to the smaller than originally planned sample size. 11 Study Sites and Principal Investigators Site Name Advocate Heart Institute St. Luke’s Hospital Northern Indiana Research Alliance St. Thomas Research Huntsville Hospital Site State IL MO IN TN AL Principal Investigator (M.D.) Stan Skaluba Andrew Kao Mark Jones Donald Chomsky James Smelser Mission Hospital/ Ashville Cardiology Associates NC Benjamin Trichon Drexel University Hospital PA Howard Eisen Sharp Memorial/ San Diego Cardiac Center CA Brian Jaski Washington Hospital Piedmont Heart Institute DC GA Samer Najjar Nirav Raval Hillcrest Hospital/ Oklahoma Heart Institute OK Alan Kaneshige St. John’s Mercy Hospital University of California at Los Angeles Abbington Memorial Hospital Hennepin County Medical Center Ohio State University Hospital University of Minnesota University of Cincinnati Tacoma General Hospital Mayo Clinic Scottsdale Morton Plant Medical Center Cleveland Clinic Northwestern University University of California at San Diego MO CA PA MN OH MN OH WA AZ FL OH IL CA Seth Barbanell Gregg Fonarow Robert Watson Brad Bart Garrie Haas S. Carolina Masri Andrew Burger Viral Shah David Eric Steidley Mahesh Amin Mazen Hanna Robert Gordon Eric Adler Virginia Commonwealth University Med Center VA Richard Cooke Scottsdale Healthcare Research Institute AZ Kris Vijay Minneapolis VA Medical Center Emory University Good Samaritan Hospital - Dayton Brooke Army Medical Center MN GA OH TX Inderjit Anand Divya Gupta George T. Broderick James Watts 12 Clinical Events Committee Name Peter E Carson, MD Address Washington DC VA Medical Center 50 Irving St. NW Washington, DC 20422 JoAnn Lindenfeld, MD Vanderbilt University 1211 Medical Center Dr, Nashville, TN 37232 Nashville, TN Barry Greenberg, MD University of California, San Diego Cardiology Department 9444 Medical Center Drive La Jolla, CA 92037-7411 13