Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
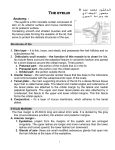
Grand Rounds Conference Reema Syed, MBBS University of Louisville Department of Ophthalmology and Visual Sciences October 3, 2014 Subjective CC: “droopy right eyelid” HPI: 7 month old male referred to Oculoplastics clinic by Peds Ophthalmology for evaluation of right upper lid ptosis. Ptosis was present since birth, however, child was noted to have a fixation preference for OS at his pediatric ophthalmologist recently. Patching OS was started for 1 hour/day History POH: ptosis OD PMH: full term, uncomplicated vaginal delivery, no birth trauma Eye Meds: None, patching OS 1hr/day Meds: none Allergies: None Family Hx: “lazy eye” (father) Objective OD OS VA (sc): CS-UM CSM Pupils: 4 to 2 mm 4 to 2 mm No anisocoria or RAPD IOP: 15 15 EOM: Full Full orthophoric in primary gaze Cycloplegic refraction: +1.00 +1.00 x90 +1.00 +1.00 x90 Objective PLE: Lids OD upper lid position does not change with feeding No palpable masses Eyelid crease minimal Palpebral fissure 5 mm Marginal reflex 1 mm distance - 1 Levator function 2-4 mm OS wnl normal 9 mm 4 mm 10-12 mm Objective Conjunctiva/Sclera Cornea Anterior Chamber Iris Lens Vitreous ON MVP Normal OU Clear OU formed OU Normal OU No heterochromia Clear OU Normal OU c/d 0.2, sharp and pink OU Normal OU Assessment 7 month old M with upper lid ptosis and poor levator function OD, without any other ocular or systemic anomalies who has recently developed amblyopia OD DDx: - Isolated unilateral congenital ptosis - Marcus Gunn jaw winking syndrome - Blepharophimosis syndrome - Congenital third nerve palsy - Congenital Horner's syndrome - Congenital fibrosis of extra-ocular muscles - Upper eyelid mass (neurofibroma, dermoid cyst) - Pseudo-ptosis Congenital Ptosis • Caused by maldevelopment of levator palpebrae superioris due to abnormal innervation • normal muscle tissue replaced by fibrous and fatty tissue • Characterized by decreased levator function, lid lag, lagophthalmos - May be sporadic or familial (gene unknown) - Strabismus 30%, anisometropia 12%, amblyopia 20% - 2/3 unilateral, 1/3 bilateral – may be asymmetric - Surgery usually delayed until 3-5 yrs of age unless: - Deprivational or anisometropic amblyopia Ocular torticollis Amount of upper lid excursion Levator function 11 mm or more Normal 8-10 mm Good 5-7 mm Fair 4 mm or less Poor Treatment Options - Levator resection: - used when levator function is good - amount of upper eyelid excursion used to determine the amount of muscle to be resected * Smith B, Della Rocca R, Nesi F. Ophthalmic Plastic and Reconstructive Surgery. Vol 1. Philadelphia: CV Mosby, 1987:Fig. 30-27 -Frontalis suspension: -used when absent or poor levator function -most commonly used for congenital ptosis -eyelid suspended directly from the frontalis so that movement of the brow can be used to elevate the eyelid *Amato M , Monheit B and Shore J. Ptosis surgery. Volume 5, Chapter 78, fig 13 Choice of sling material Advantages Disadvantages Autogenous Fascia Lata - Gold standard - Excellent tensile strength - Best long-term results - Recurrence unlikely - Need for another surgical site - increased risk of infection - Minimum age 3 yrs Allogenic Fascia Lata - any age - Second donor site not required - Small chance of rejection - transmission of infection from donor to recipient Supramid - any age - Second donor site not required - High chance of recurrence due to degradation of sling material Silicone - Not associated with recurrence - Can be adjusted intra and post-operatively to adjust lid margin height over time Complications Under/over correction Asymmetric eyelid contour Scarring Wound dehiscence Eyelid crease asymmetry Lagophthalmos with exposure keratitis Back to our patient Underwent silicone rod frontalis suspension OD 1 week post-op • Retrospective chart review of 4 patients with ocular torticollis due to bilateral congenital or acquired ptosis who underwent surgical correction • pre and post operative systemic symptoms in 1 adult and developmental milestones in 3 children are described • Adult patient: 62 yr M with history of severe bilateral ptosis for 10 yrs presented to his PCP with debilitating upper back pain for 3 yrs. Pain persisted despite multiple referrals and therapies. Abnormal head posture due to ptosis found on ophthalmic exam. Pain began to resolve within a week of surgical correction of ptosis • Children: 12m , 10m, 5m olds with bilateral ptosis and development of head-tilt, chin up position. No amblyopia but severe delays in gross motor development without delay in any other milestones. Caught-up with motor milestones within a few months of corrective surgery References BCSC Orbit, Eyelids and Lacrimal System BCSC Pediatric Ophthalmology and Strabismus Smith B, Della Rocca R, Nesi F. Ophthalmic Plastic and Reconstructive Surgery Amato M , Monheit B and Shore J. Ptosis surgery Loff HJ et al. transconjunctival frontalis suspension: a clinical evaluation. Ophthal Plast Reconstr Surg. 1999; 15(5): 349-354. Baroody M et al. Advances in the diagnosis and treatment of ptosis. Curr Opin Ophthal. 2005; 16(6):351-355 Lee M, et al. Frontalis Sling Operation using silicone rod compared with preserved fascia lata for cogenital ptosis. Ophthalmology 2009; 116(1) 123-129. Thank you