Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Aldosterone
in
Cerebral Salt Wasting
BY JOH X H. K.
ALTHOUGH recent studies of patients
with cerebral and pulmonary salt wasting have implicated "inappropriate"' antidiuretic hormone secretion as the basic defect,
the norinality of aldosterone responsiveness
has not been firmly established.'-'
This paper reports a patient with cerebral
salt wasting and hyponatremia in whom bal
VOGEL,
M.D.
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
eific gravity of 1.016, pH 5.5, negative for sugar,
protein, and on microscopic. The white blood-cell
(ouMt was 6,100 per mm.3, with a normal differential. The hematocrit value was 41 per cent.
Fasting blood sugar was 77 mg. per 100 ml., nonproteiin nitrogen 27, and cholesterol 235. Serumn
sodium wqs 127 mEq. per L.. potassium 5.1,
chloride 81.6, and carbon dioxide content 24. The
serum total pr otein was 7.2 Gm. per cent, with
3.9 albumin anid ) 3 globulin. The thvmol turbiditv
was 3.0, cephalin flocculation 0 to 48 hours, and
prothrombin time 72 per cent. A serologic test
and L.E. preparations were negative. Seru-m calcium, phosphorus, and alkaline phosphatase were
niorma.l. Urinary. 17-hydroxvcorticoids were normal,
varying from 6.3 to 19 mg. per 24 hours. The
electroencephalogram was norial and an electrocardiogram was normal except for loIw voltage.
The chest film suggested miinimal pulmonarv
el)hpvsema, spine films were nornmal, and skulll
filmus revealed an old fracture on tlhe left and
burr holes on tbe right. A spirogram wras normal.
The chest pain varied markedly and was un1related to aetivitv, position, or neals with inconsistent responses to medications and placebos. The
weakness of the legs was inconstant, did not inhibit
normal activity, and u-as unrelated to serum sodiuin levels. Neuroloogic consultants found no evidence of residual or active disease. Psyehiatric
evaluation suggested a psvehopatbic personality.
On ad lib. water intake of 1,890 to 3,500 ml.
per day and sodiumL intake of 90 mltlq., hyponatremia with urinary sodium wasting' persisted.
Therefore. ietabolic balance stuidies wrere insti-
anee studies suggested normal aldosterone
response and inappropriate antidiuretie lbor
n.tio-ne activity.
Case Report
A 38-year-old white, single, race-car driver, was
admitted to Vanderbilt Universitv Hospital, Nashville, Tennessee, November 4, 1959, with the chief
comiplaint of chest pain of 6 months' duration.
Four months prior to admission he was involved
in an automlobile accident resulting in a depressed
skull fracture of the left parietal area and a subdural hematoma in the right frontal-parietal area
requiring drainage with burr holes. Recovery was
allegedly unieventful without neurologic deficit.
One monith prior to admission hle was seen at
G(rady Meiemorial Hospital in Atlanta, Georgia,
with chest pain. An electrocardiogram and chest
filmn were normal. Hyponatremia with urinary salt
wasting was demonstrated, however, whieh subsequently responded to water restriction but not
to salt loading. An intravenous pyelogram, blood
nonprotein nitrogen? and urinary phenolsulfonphthaleirn exeretion were normal. Urinary 17hydroxvcorticoids were normnal both resting and
after stimulation with ACTH.
He addmitted to moderate alcoholic intake and
Wave a histor-v of acute pvelonephritis involving
the riiht ki-dnev 5 y ears prior to admiission.
On physical exaamination the blood pressure was
108/98 nmm. Hg, the pulse was 84, and respirations were 16 per m-inute. The skin was of good
tu-rger and color with normal hair distribution
and no abnormal pigmentation. Skull defects were
palpated in the areas of the old fracture and
burr holes. Except for slight weakness in the
le,s. tl-he phyvsical ex.aiminition w:ns otherwise within
tuted.
Methods
A weighed diet with a basic content of 250 rnl.
of water and 8.6 mEq. of sodium-l witlh constant
calorie, carbohydrate, fat, and protein comuposition was given daily. This permitted sodium and
water intake to be varied without altering the
basic diet. Body weight was determinied dail-v
under standard conditions. Urine u-as collected in
24-hour lots from 8:00 a.m. to 8:00 a.m., and
hlood was drawn at 8 :00 a.m. daily. Serum and
urine were analyzed for sodium and potassium
by flame photometer. Osmolality (mOsml Kg.) of
serum and urine was determined in duplicate froim.
freezing-point depression with a Fiske osinometer.
Urinary aldosterone was deter-mined in triplicate
by the double-isotope derivative assay of Kliman
and Peterson.9 Normal exeretion by this technic
normal1st I limits.
Laboratory results: Urinalysis revealed a speFrom the Departmeiit of Medlicine, Vanderbilt
Selool of AMedicine, Nashville, Tennessee.
litiiersity
44
Cireculotion, 'Voluzme rXXVII, Ja!tarur/ 196;
ALDOSTERONE IN CEREBRAI SALT WASTING
200
Na
INTAKE
Meq/DAY
100
-
100- I I I
2
3
4
1
9
5
10
II
-l
12
13
14
15
16
14
15
16
14
I--
16
DAYS
3000
WATER
INTAKE
cc/DAY
1000
0
140
SERUM
Na
-
120 -
Meq/L
L
.--
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
200
1
-3
2
4
T
5
6,
8
DAYS
-r
9
I
12
13 1
~~~~t-I -**-*I
~~~~~~~I
I
9g
0
1
II
-
URINE
No
100
1-1
Meq/DAY
-F
°2I
URINE
ALDOSTERONE
,Ag/DAY
0
1
1
4
3
04 1
403020
o
01
a
DAYS
6
3
~
12 1 13
10 V
15
F
2
8 1 91
DAYS
61
2
II
13114 I1
is
MOSM
URINE
-@
o {3
4
6
5
8
4 e
9
0
9
10
o t---~-------11
I
13
1
14
15 1
DAYS
66 BODY
WEIGHT
Kg
64-
-_
52
2
3 I
41
5
6
1
I
8
I
I
IP 12
13 ' 14 1
15 !
I
DAYS
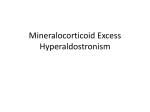
Figure 1
Effects of various sodium and water intakes.
10 ,ug. per 24 hours and ranges from
5 to 19. No aldosterone values were determined
on days 4, 6, 8, 9, 15, and 16.
averages
Results
Effects of high sodium and high water intake: (Days 1-3, table 1 and fig. 1) Prior to
the balance study while on ad lib. water and
Circulation, Volume XXVII, January 1963
sodium intake, the serum sodium varied from
117 to 127 mEq. per L. and the 24-hour urinie
sodium excretion from 47 to 239 mEq. On the
first and third days of the study the findings
were similar. However, on the second day
only, the patient failed to take the full water
allowance with a subsequent rise in aldoster-
VOGEL
46
oiie and serum sodium and a decreased uri
(- ,o N
cl
z
cq
CA
O
z
CA
QO)
N
rl
1C-"C1
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
a).
t-9
.
,
0) 0) 0) 0)
1't- L&
a) t- 0) 1>. 01 )] @1t
.3
.C
-3
C.3
3 O
.
.
.
U)
e)
rl
co
C)
C)
01CA
?0o
C1i
r-l
C:)
1c10A C)
"r
Ct
) 01
.
.
r-
--
*
) 0) 0)
) 0)
=
1-
"
0
O]
CJ
.
.
a)0)
I.-1
.~ .~ . .~ .-1 .~ .l
.e
alm C1 CA v m <w It It m
r1r-.
E-4
i
.
.
.
.
*
L
J
C)t 'A
CJ C3CC 0C lCI
a)
CA
CA
--
-
II
Ii
i
1.
c
c1
CO
clz0C0
7 "
^]0C 011
z
]C]t
1C
]Nm
]C]C1C
0
I1
nary sodium.
Effects of high sodiunm and low water intake: (Days 4-7, table 1 and fig. 1) There was
a conspicuous rise in serum sodium and osnmo-
-
4=-
c)
C)-
-l
x
"
-*
)-
C
01-rCi
r-
.
"I
-~
.
.
-
t
-,
.
m =
r.4
r-
vC
c
<
C)
-Q
0c,
r
'-4
-4
r
I
IC: tc0
t:'- 00)
V00
x v
C01 (, 01
t- 't : lfC
C-It;CG10?Ia
'
fcy 'CC'O CA
c
CQI 0)C.
v
.
cl
0
If:
a'A
tn. X
C
-
1
-w 1 =-or,
rH i
r
ri
.1
'-
kr
17.
i
-Z
.-
-z !V
.- 1 : i
7-.
- '-.
17*
r-'
1H.
)C
00>
>
CC
4
C0
)C
l.
c t
z
o4
In.o
C)o
0I
-f
o.'
m
A-tID~
01
to
C)D
)c
c>
)c
.C
lalitv associated with a decrease in body
weight. Urinary sodium exeretion continued
as in the previous period with nio change in
aldosterone excretion.
Effects of low sodiumv and low water intake:
(Days 8-12, table I and fig. 1) There was a
norm-ial rise in aldosterone excretion to 35 t,g.
In addition, there was a progressive fall in
urinary sodiumn exeretioni and a further increase in serunl sodiuit and osmnolalitv.
Effects of low sodiutm and high uwater intak(e: (Days 13-16. table 1 and fig. 1". The
rapid fall in serumji sodium osmolality and
uriniarv aldosterone in association with inereasing urinary sodium excretion and body
weight is clearly shown.
The n-onprotein: nlitrog,eni an-id serumy creatinine were normual throughout the study. Of
note is the urinary osiolality, which was ii-i
excess of serum osnmolality throughout the
entire study.
Effects of ivatcr avd alcohol loads: (Table
*. and fig 2). Ilaviing been on normal sodiun
and water intake, the patient and the normal
ontrol were fasted for 6 hours. Subsequently
I-hour eontrol urinie anid serumll specimens
were collectedl anid anialyzed for sodium., creatiiiinei aind osmalality. The subjects remainied
supine throughout the study except when providing specimens. Urine volume was recorde(d
and free water clearance calculated. The subjects theni received water loads by mouth of
20 ml. per KIg. over a 5- to 1.0-minute period
and urine and seruma specimnenis were collected
at hourly intervals.
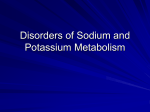
The conitrol (fig. 2. top) clearlv reveals a
i1ornoal response wvitli a moderate increase in
urinie flow and free water clearanee and a
decrease in urine osmolality, becomning maximnal 1 hour after the water load.'0 By contrast.,
the patielnt revealed a markedly abnormal response with miinimal increase in urine flow
and free water clearance with failure to lower
urine osmolality below 121. No significant
Circulation. Volume XXVii, January 1963
47
ALDOSTERONE IN CEREBRAL SALT WASTING
Table 2
Free Water Clearance (ml./mnin.)
Time Hr.
Control
Patient
- .4
-1.0
1
H20 Load
2
3
4
MOS/L
1.5
6.4
4.6
.8
1.2
2.5
5.8
.1
SERUMG --.---
URINE
Alcohol Load
5
6
7
8
.2
4001
-1 ---20 e-
.8
URINE
cc/M1in.5
1490cc
FLOW
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
change in creatinine clearance occurred in
either subject.
Three hours after the water load each subject received 50 ml. of 95 per cent ethyl alcohol by mouth over a 5- to 10-minute period.
In the control subject there was a significant increase in urine flow and free water
clearance 1 hour after the alcohol load, resulting in a negative water balance of 168 ml.
during the 7-hour period (excluding insensible
water loss). In the patient, no significant
change occurred in urine flow or free water
clearance, resulting in a positive water balance of 445 ml. during the 7-hour period. No
significant change in creatinine clearance occurred in either subject.
Discussion
Cerebral disease with hyponatremia and
excessive urinary sodium wasting has been
reported by Peters et al.,8 MeCrory and Macauly,5 Epstein and Levitin,4 Goldberg and
Handler,1 and Carter et al.6
In McCrory and Macauly's patient,5 a 51½2month-old girl with diffuse cerebral disease,
restriction of water in relation to sodium resulted in normal serum sodium levels. The
response to a water load was abnormal as
manifested by a failure of urine osmolality
to fall below 150. A bioassay for antidiuretic
hormone while the patient was hyponatremic
was markedly positive, but a control was essentially negative. With exogenous salt-retaining steroids there was an increase in body
weight, but not of serum sodium.
Epstein and Levitin's patient,4 a 19-yearCirculation, Volume XXVII, January 1963
0- I1
2
6
5
4
3
6
7
HOURS
N
P
H20POI
600-
MOSM/
50cc PO
95% C215°
11320 ce
+
.1370 cc
INTAKE
IT
400-
SERUM a.0
URINE
-*e
-----
200-
-
0-I
URINE
FLOW
cc/Milt_
* 92S cc
o_
0-Il
OUTPUT
2
3
4
O
is
HIOURS
Figure 2
and
Effect of water
alcohol loads. Top, normal
subject; bottom, patient.
old girl with epilepsy, was similar to the above
patient. There was a definite inverse relation between water intake and serum sodium,
positive bioassay for antidiuretic hormone
after water loading, and failure to decrease
urine osmolality normally following an alcohol
load. With combined sodium and water restriction, however, the urinary sodium excretion decreased to 2 mEq. per day.
The four patients studied by Goldberg and
Handler' were strikingly similar to the patients noted above. Their serum sodiums were
\rOGEL
48
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
iinverselv proportional to water in-take, aiid
large sodium loads were ineffective in raising
the serum levels unless combined with water
restriction. One patient failed to ehange urine
osmolality with alcohol.
As with our patient, one of Carter et al 's.6
patients developed hyponatremia followving a
skull fracture, and although the fracture
healed eompletely he remained persistently
hvponatremic when allowed free access to
water. With either restriction of sodiuim to
17 mEq. per dav or 9-alpha-fluorohvdroeortisone a positive sodium balanee wvas attained.
The basic defect in these cases of cerebral
salt wasting would appear to be the inappropriate secretion of antidiuretic hormone.
However, the positive responses to salt restriction or exogenous salt-retaining steroids sugest a normal aldosterone mechanism.
A similar syndrome of salt wasting associated with bronehogenic carcinoma has been
reported by Schwartz et al..2, 3 and careful
studies in three patients revealed hyponatremia, urine osmolality consistently higher than
serum osmlolality, and excessive urinary salt
wasting, which was attribuited to inappropriate antidiuretic hormone secretion. The serum
sodium was closely related to and inversely
proportional to fluid intake, with no significant response to high-sodium intake except
during water restrietion. All patients developed a positive sodium balanee on exogenous
salt-retaining steroids and after ACTH. Aldosterone determinations were low normal in
the presencee of hyponatremia during both
low- and high-sodium intake. These results
sug,gested normal aldosterone responsiveness.
Dossetor et al.]" recently reported another
patient with bronehogenic carcinoma complieated by hyponatremia in whom an inverse
relationship between serum sodium and water
intake was noted, and thought to be a consequence of inappropriate antidiuretic hormone.
As with our patient, aldosteron-e excretion was
normal during balance periods of low sodium
with excess water intake and high sodium
with -restrieted water intake. The effect of
comnbined low sodium and water intake was
not studied, biut presumablY would havre re
sulted in an in-icreased aldosterone exeretio'-i,
as oeeurred in our patient. Dashe and Hern
kin12 have also reported a case of inappropriate antidiureticlhormone secretion follow-
ing yttrium90 hypophysectomy.
The role of extracellular fluid volume in teli
regulation of aldosterone seeretion has beeni
well documented by Bartter et al.13 They produced the control findings in our patietnt by
the simultaneous admlinistration of Pitressin
and a water load to a salt-depleted subject.
This resulted in a decreased aldosterone exere
tion, serum sodium, and osmolality but ati
increase in urinary sodium excretion and body
weight. Similar results have beeni noted- bV
Cox, Leonard, and Singer,14 anid Leaf et al.l'
in human subjects. ani by Leaf and Mamb01l
in dogs. Thus, it is clear that inappropriate
secretion of antidiuretic hormone may be the
basic abnorimalitv in this type of excessive
urinary sodiunm wasting with hIyponatremia.
The second study period in our patient of
water restriction with normal sodium initake.
during which urinary sodium excretion re
mained high and aldosterone low, has also
been produced by Bartter et al.'3 They dem
onstrated that bv maintenance of a normal
extracellular fluid volume with a reduced
fluid intake of hvpertonic coneentration and
subsequent contraction of the intracellular
space, aldosteromie and sodium excretion continued unchanged.
WVith combined sodium and water restriction, the extracellular fluid volume will decrease and aldosterone secretion will increase
in aii effort to re-expand the extracellular
fluid volum-ie by the conservationi of sodium, if
the aldosterone mechanism is normal, and, as
shown (days 8-12), this occurred in our pa-
tient.
The last phase of the study fdays 13-16)<
stresses further the regulatory importance of
the extracellular fluiid volume. With a normal
water intake and low sodiumB intake, the
extracellular fluid volume increased rapidlv
b)v virtue of the abnormal level of antidiuretie
lhorm-none with a prompt decrease in aldosteronie excretion and an increase in urinary
sodiuni exeretion.
Circulation Volume XXVII, Jan-uary 1f963
ALDOSTERONE IN CEREBRAL SALT WASTING
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
The response in the control subject to water
and alcohol loads, characterized by maximum
diuresis 1 hour after the respective loads is
in agreement with other reports in normal
subjects."6 The failure of our patient to decrease urine osmolality below 100, or to sustain any significant change in free water
clearance after water and alcohol loads in
the face of a normal creatinine clearance, is
highly suggestive of inappropriate antidiuretic hormone secretion.3
The studies of Rubini et al.,17 suggest that
the effect of ethyl alcohol is on the release or
production of antidiuretic hormone in that
normally a 60- to 90-minute lag period occurs
before a response to the alcohol load is noted.
This represents the time necessary for circulating antidiuretic hormone to be cleared.
Thus, the failure of our patient and othersl-4
to respond to alcohol loads suggests inappropriate secretion of antidiuretic hormone.
Of interest is a recent report by Grumer
et al."8 on a patient with episodic inappropriate secretion of antidiuretic hormone, but
no apparent underlying disease. In their patient and in our patient, the mechanism of
the inappropriate secretion of antidiuretic
hormone is not clear. Whether there has been
a resetting of the "osmostat," or persistence
of an abnormal stimulus to antidiuretic hormone secretion is not apparent.
The results in our patient suggest a normal responsiveness in aldosterone stimulation,
secretion, and end-organ effectiveness in association with inappropriate antidiuretic hormone secretion.
The maintenance of a normal aldosterone
mechanism suggests that the receptors regulating aldosterone-stimulating hormone may
be independent of the hypothalamus. In support of this are recent studies suggesting
that these receptors may be located in the
kidney.19' 20
Summary
A metabolic balance study in a patient
with cerebral salt wasting is reported. The
results suggest that a normal aldosterone
mechanism was present in association with
inappropriate antidiuretic hormone secretion.
Circulation, Volume XXVII, January: 1963
Acknowledgment
The author wishes to thank Donald Island, B.S.,
for the aldosterone determinations, Dr. Grant W.
Liddle, for his advice and criticism, and Dr. Elbert
P. Tuttle, Jr., for referring the patient.
References
1. GOLDBERG, M., AND HANDLER, J. S., Hyponatremia and renal wasting of sodium in patients
with malfunction of the central nervous system. New England J. Med. 263: 1037, 1960.
2. SCHWARTZ, W. B., BENNETT, W., CURELOP, S.,
AND BARTTER, F. C.: Syndrome of renal sodium
loss and hyponatremia probably resulting from
inappropriate secretion of antidiuretic hormone.
Am. J. Med. 23: 529, 1957.
3. SCHWARTZ, W. B., TASSEL, D., AND BARTTER,
F. C.: Further observations on hyponatremia
and renal sodium loss probably resulting fromn
inappropriate secretion of antidiuretic hormone.
New England J. Med. 262: 743, 1960.
4. EPSTEIN, F. H., AND LEvInN, H.: "Cerebral
salt wasting": An example of sustained inappropriate release of antidiuretic hormone. J.
Clin. Invest. 38: 1001, 1959.
5. MCnROY., W. W., AND MACAULAY, D.: Idiopathic
hypoinatreinia in ani infaint with diffuse cerebral
damage. Pediatrics 20: 23, 1957.
6. CARTER, N. W., RECTOR, F. C., JR., AND SELDIN,
D. W.: Hyponatremia in cerebral disease resulting from the inappropriate secretion of antidiuretic hormone. Newv England J. Med. 264:
67, 1961.
7. ROBERTS, H. J.: Syndrome of hyponatremia and
renal sodium loss probably resulting from
inappropriate secretion of antidiuretic hormone.
Ann. Int. Med. 51: 1420, 1959.
8. PETERS, J. P., WELT, L. G., SIMs, E. A. H.,
ORLOFF, J., AND NEEDHAM, J.: A salt-wasting
syndrome associated with cerebral disease. Tr.
A. Am. Physicians 63: 57, 1950.
9. KLIMAN, B., AND PETERSON, R. E.: Double isotope
derivative assay of aldosterone in biological
extracts. J. Biol. Chem. 235: 1639, 1960.
10. ROBINSON, F. J., POWER, M. H., AND KEPLER,
E. J.: Two new procedures to assist in the
recognition and exclusion of Addison's disease.
Proc. Staff Meet., Mayo Clin. 16: 577, 1941.
11. DOSSETOR, J. B., VENNING, E. H., AND BECK,
J. C.: Hyponatremia associated with superior
vena cava obstruetion. Metabolism 10: 149,
1961.
12. DASHE, A. M., AND HENKIN, R.: Water intoxication after hypophysectomy: an unusual case.
Am. J. M. Sc. 241: 752, 1961.
13. BARTTER, F. C., LIDDLE, G. W., DUNCAN, L. E.,
JR., BARBER, J. K., AND DELEA, C.: The regulation of aldosterone secretion in man: the role
of fluid volume. J. Clin. Invest. 35: 1306, 1956.
VOGEL
-ao
14. Cox, J. R., LEONARD, P. J., AND SINGER, B.:
Effect of vasopressin on the volume of body
fluid compartments and its relation to aldos
terone excretion. Clin. Sc. 21: 205, 1961.
15. LEAF, A., BARTTER, F. C., SANTOS, R. F., AND
WRONG, 0.: Evidence in man that urinary
electrolyte loss induced by pitressin is a function of water retention. J. Clin. Invest. 32:
868, 1953.
16. LEAF, A., AND MAMBY, A. R.: An antidiuretic
mechanism not regulated by extracellular fluid
tonicity. J. Clin. Invest. 31: 60, 1952.
17. RUBINI, M. E., KLEEMAN, C. R., AND LAMDIN,
E.: Studies on alcohol diuresis. I. The effect
of ethyl alcohol ingestioil on water, electrolyte,
and acid-base metabolism. J. Clin. Invest. 34:
439, 1955.
18. GRUMER, H. A.,. DERRYBERRY, V., DUBIN, A., AND
WALDSTEIN, S. S.: Idiopathic, episodic inappropriate secretion of antidiuretic hormone. Am.
J. Med. 32: 954, 1962.
19. DAVIS, J. 0.: A critical evaluation of the role
of receptors in the control of aldosterone
secretion and sodium excretion. Progr. Cardiovas. Dis. 4: 27, 1961.
2O. MULROW, P. J., AND GANONG, W. F.: Role of the
kidney and the renin-angiotensin system in the
response of aldosterone secretion to hemorrhage. Circulation 25: 213, 1962.
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
Richard Bright
He could not have been called a brilliant man. He miade at first no great impressioni
on those about him. But brillianey is often ephemeral; very often brilliancy spells instability. Bright showed a steadfastness of purpose and an equanimity that are rarer
and more precious than mnere brilliancy. He was a simple, straightforward, kindly man,
who met life with charity and tolerance and serenity; a conscientious, painstaking physician; a patient, careful, modest, scrupulous time-taking observer. He became a wise
and learned man, and the fruits of his labours assure him a well-nmerited and honourable
immortality.
Bright was buried in Bethnal Green. There is a tablet dedieated to his memory in
St. James' Church in Piccadilly. The inscription ends with these words:
"He contributed to medical science many discoveries and works of
great value,
And died while in the full practice of his profession after a life
of warm affection
unsullied purity and great usefulness."-W. S. THAYER (B.M.J., 1927). The
Quiet A rt: A Doctor's Anthology. Compiled by DR. ROBERT COOPE. Edinburgh &
London, E. & S. Livingstone Ltd.. 1952, p. 66.
Circulation, Volume XXVII, January 196S
Aldosterone in Cerebral Salt Wasting
JOHN H. K. VOGEL
Downloaded from http://circ.ahajournals.org/ by guest on June 14, 2017
Circulation. 1963;27:44-50
doi: 10.1161/01.CIR.27.1.44
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1963 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://circ.ahajournals.org/content/27/1/44
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles
originally published in Circulation can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column of
the Web page under Services. Further information about this process is available in the Permissions
and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/