Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
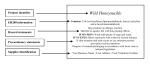
Emerg Med Clin N Am 25 (2007) 333–346 Emergency Department Management of the Salicylate-Poisoned Patient Gerald F. O’Malley, DOa,b,c,d,* a Division of Toxicology, Albert Einstein Medical Center, 5501 Old York Road, Philadelphia, PA 19141, USA b Thomas Jefferson University Hospital, Philadelphia, PA 19141, USA c Children’s Hospital of Philadelphia, Philadelphia, PA 19141, USA d Philadelphia Poison Control Center, Philadelphia, PA 19141, USA The term salicylate refers to any of a group of chemicals that are derived from salicylic acid. The best known is acetylsalicylic acid (aspirin). Acetylsalicylic acid is metabolized to salicylic acid (salicylate) after ingestion. The salicylates originally were derived from salicin, the active ingredient in willow bark, which Hippocrates used 2500 years ago for treating pain and fever [1,2]. Salicylates also occur naturally in many plants such as strawberries, almonds, and tomatoes [3]. Poisoning by aspirin is common and is under-represented in poison center data, because it is often not recognized [4–6]. The in-hospital mortality for unrecognized chronic aspirin poisoning is reportedly three times higher than if the diagnosis is made in the emergency department [7]. Familiarity with the clinical presentation during the various stages of acute and chronic aspirin poisoning is important for the practice of emergency medicine. The most challenging aspect of the clinical evaluation and management of the aspirin-poisoned patient may be recognition of the subtle signs and symptoms of chronic, nonintentional aspirin overdose (Box 1). Epidemiology Salicylate poisoning continues to be an important overdose that frequently presents to emergency departments [8–10]. There were over 21,000 * Department of Emergency Medicine, Albert Einstein Medical Center, 5501 Old York Road, Philadelphia, PA 19141. E-mail address: [email protected] 0733-8627/07/$ - see front matter Ó 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.emc.2007.02.012 emed.theclinics.com 334 O’MALLEY Box 1. Pitfalls in the emergency department management of salicylate–poisoned patients Failure to recognize the presence of salicylate toxicity Failure to appreciate the presence of continued absorption of salicylate Misinterpreting clinical significance of serum salicylate levels, because units of measure were unclear Reliance on one or two serum levels of salicylate that may not describe a trend of decreasing total body burden of aspirin clearly Misinterpretation of low serum salicylate levels as nontoxic and failure to comprehend the changing acid–base status of the patient Waiting until serum salicylate levels are determined before beginning urinary alkalinization Accidentally adding bicarbonate to isotonic saline (creating a hypertonic solution) rather than intravenous dextrose/water solutions to alkalinize the urine Forgetting to add potassium to the urinary alkalinization infusion Failure to recognize the emergent need for definitive therapy (hemodialysis) on the basis of impending end organ injury (Box 2). Inappropriately or prematurely initiating intubation and mechanical ventilation without hyperventilation and without simultaneous hemodialysis Prematurely discharging patients without demonstrating metabolic stability, declining salicylate levels, and the absence of an aspirin bezoar aspirin and nonaspirin salicylate exposures reported to the United States poison centers in 2004, with 43 deaths and 12,968 patients requiring hospital treatment [11]. Because poison center data are collected passively, that statistic is certainly an underestimate of the true incidence of salicylate poisoning occur in the United States. One half of the reported exposures (10,786) were categorized as intentional overdoses. The incidence of chronic aspirin poisoning is not known, but it is misdiagnosed frequently [12]. In recent years, packaging strategies such as child-resistant packaging and reducing the amount of medication in each package of over-the-counter analgesics have impacted the incidence of poisoning. It is estimated that the use of child-resistant packaging for salicylate-containing medications has resulted in a 34% reduction in the salicylate-related child mortality rate [13]. In England, Australia, and Ireland, analgesics are packaged and sold in MANAGEMENT OF THE SALICYLATE-POISONED PATIENT 335 small amounts (ie, 4 g of acetaminophen). This has resulted in a 30% decrease in the number of patients requiring liver transplantation for acetaminophen-induced hepatic failure and a 22% reduction in suicidal deaths from acetaminophen and salicylate [14]. Large aspirin overdoses were reduced by 39% on average in the countries in which the limited package formulation is required [14,15]. Pathophysiologic basis for poisoning Salicylate is a metabolic poison. Understanding the pathophysiology of its metabolic effects can help to understand the clinical manifestations of toxicity. The metabolic derangements induced by salicylate poisoning are multifactorial, but the principal pathophysiologic mechanism in salicylate poisoning is interference with aerobic metabolism by means of uncoupling of mitochondrial oxidative phosphorylation [15a,16]. This leads to the interruption of a series of enzyme-mediated mitochondrial functions and increased anaerobic metabolism with cellular conversion of pyruvate to lactate and rapid development of lactic acidosis [17,18]. The inefficiency of anaerobic metabolism results in less energy being used to create ATP and release of the energy created during the metabolism of glucose in the electron transport chain as heat, so salicylate poisoned patients may become febrile [19]. The absence of fever, however, does not rule out salicylate poisoning. The acidosis is caused by anaerobic metabolism and the inability to buffer hydrogen ions, which is reflected by the accumulation of lactate. The presence of acetasalicylic acid or salicylate molecules probably contributes little to the acidotic state [15a,20]. Interference with oxidative phosphorylation by salicylate also will impact glucose homeostasis negatively by causing glycogen depletion, gluconeogenesis, and catabolism of proteins and free fatty acids, the end result being low serum glucose levels and central nervous system (CNS) hypoglycemia relative to serum glucose levels [15a]. Absorption and metabolism of salicylate The pharmacokinetic profile of aspirin is unique and explains the unique characteristics of clinical poisoning. The ionization constant (pKa) of aspirin is 3, which means that at a pH of 3, approximately half of the available chemical is in the ionized state. In an acidic environment like the stomach, more of the drug will be absorbed compared with tissues at a higher pH [21]. The absorption of aspirin from the stomach can be delayed by the presence of food in the stomach and the formulation of the aspirin, (eg, enteric coating of pills may create concretions and bezoars that limit available surface area for absorption) [22]. Aspirin is thought to cause spasm of the pyloric sphincter, increasing gastric transit time and prolonging the time that aspirin is in the acidic environment of the stomach, favoring increased 336 O’MALLEY absorption [21]. Salicylates also are absorbed readily in the unionized form from the small intestine [23,24]. Dermal salicylate formulations typically do not result in tissue penetration much deeper than 3 to 4 mm in animal studies [25,26] and human volunteer experiments [27]. Methyl salicylate has less dermal absorption than either camphor or menthol, with lower mean plasma levels and shorter elimination half-life than either compound in people [28]. Significant amounts of salicylate typically are not absorbed through the skin except in select patients, such as children and patients with compromised skin such as burn patients or patients who have severe psoriasis [29–31]. In therapeutic doses, the major route of salicylate biotransformation is conjugation with glycine in the liver. A small amount of aspirin is excreted unchanged in the urine [15a]. In overdose, the liver’s ability to metabolize the drug is overwhelmed, and unchanged salicylate excretion through the kidney becomes a much more important elimination route. Salicylate–induced acid-base changes Respiratory alkalosis Salicylate toxicity initially will create a pure respiratory alkalosis because of direct stimulatory effects on the respiratory centers of the cerebral medulla. This is characterized in the blood gas by a decrease in the partial pressure of dissolved CO2 accompanied by an elevated pH and normal to slightly lower levels of serum HCO3 [32]. There is some controversy as to whether pediatric aspirin poisoned patients demonstrate this phase of acid–base derangement. Pediatric patients may present later in the course of the poisoning, or the centrally mediated hyperventilatory phase of aspirin poisoning may be so subtle in children that it often is missed [33–36]. Mixed acid–base disturbances As the poisoning progresses and more of the aspirin is absorbed into the serum and is incorporated into the mitochondria, uncoupling oxidative phosphorylation, lactic acid accumulates in the serum, and metabolic compensatory mechanisms are initiated [16]. Hyperventilation becomes a true compensatory mechanism in addition to the byproduct of central medullary stimulation [20]. This phase is characterized metabolically by a continued decrease in the pCO2, marked decline in measured HCO3 and possibly a decrease in serum pH, depending on the ability of the patient to maintain the respiratory demands of the developing acidosis and to retain bicarbonate in the kidney [37]. A common error at this stage of the poisoning is to acknowledge that the serum pH is close to 7.4 or slightly higher than 7.4, and assume that the patient is compensating adequately for the acidosis. Metabolic acidosis As the ability to compensate for the acidosis is overwhelmed, pH drops; lactic acid accumulates, and serum bicarbonate is consumed. Patients who MANAGEMENT OF THE SALICYLATE-POISONED PATIENT 337 reach the stage of aspirin poisoning where pH is less than 7.4 with decreased pCO2 and low serum bicarbonate are dangerously unstable, likely to decompensate hemodynamically and will begin to demonstrate other symptoms of end-organ injury [37]. Clinical presentation Classic salicylism The triad of salicylate poisoning consists of hyperventilation, tinnitus, and gastrointestinal (GI) irritation [38,39]. Physicians should remain aware that patients may hyperventilate with a normal respiratory rate by increasing tidal volume (hyperpnea) and should make it a habit to observe respiratory patterns carefully. Ototoxicity is a well-described phenomenon with salicylism, and it is thought to be secondary to interference with chloride channels in the cochlear hair cells that transmit sound waves [40,41]. The ototoxicity is most noticeable in the range of serum salicylate from 20 to 40 mg/dL [40,42]. Aspirin, especially enteric-coated formulations, are known to develop concretions and bezoars in the stomach and act as a direct GI irritant leading to nausea, vomiting, and abdominal pain [22,43,44]. Early presentation Patients who present early in the course of salicylate poisoning may have modest symptoms, and the hyperventilation may be mistaken for emotional excitation or anxiety. GI irritation may or may not be present, and tinnitus or other symptoms of ototoxicity may be overlooked unless the physician specifically tests for them with direct questioning or confrontational hearing testing. Vital signs may reflect emotional agitation and CNS stimulation with tachycardia, increased work of breathing (increased minute ventilation), and overall autonomic up-regulation. Early in the course of acute poisoning, fever generally will be absent [39]. Clinical symptoms will be variable if the patient ingested more than one drug, or the ingested aspirin formulation contained a CNS depressant, which might blunt the expected hyperventilation and respiratory alkalosis [45]. Laboratory values early in the course of aspirin poisoning will be largely normal or will reflect the direct stimulatory effect of salicylate on the cerebral respiratory center. Serum aspirin levels may be elevated modestly (20 to 40 mg/dL), and blood gas analysis may demonstrate pure respiratory alkalosis with elevated pH and low pCO2 with normal or near-normal HCO3 [39]. The decision to determine serum salicylate concentrations is not difficult. Although serum salicylate levels may not be required to screen every asymptomatic overdose, liberal use of the laboratory to make the diagnosis and follow resuscitative efforts is advisable [46–48]. 338 O’MALLEY Late presentation As salicylate enters the mitochondria, dramatic changes in vital signs and clinical stability occur. Serum salicylate levels alone are not adequate to accurately assess and follow seriously poisoned patients [49]. Serum salicylate levels do not reflect the total body burden of salicylate, and so to evaluate the rapidly changing acid base status of an aspirin poisoned patient, serial salicylate levels should be accompanied by serial blood gas analysis [5]. Patients who present in the late phases of salicylate toxicity often are misdiagnosed as sepsis [50], myocardial infarction [51], or as agitated or otherwise psychiatrically disturbed [43,52,53]. Death from salicylism The progression to death from salicylate poisoning is particularly tumultuous. The toxic effects of the salicylate molecule on mitochondrial function and subsequent basement membrane leakage overwhelm the compensatory capacity of the organism. This leads to marked metabolic acidosis with development of pulmonary and cerebral edema. Myocardial depression and hypotension secondary to the acidosis and volume deficit occur, and CNS depression with seizures secondary to hypoxia, hypoglycemia, and direct CNS toxicity often precedes cardiopulmonary arrest [54]. In one study, nearly half (45%) of the patients who died from salicylate poisoning arrived at the emergency department alert and deteriorated while there [55]. In another study, 39% of the patients who had severe salicylate poisoning requiring ICU management arrived alert with minimal symptoms [56]. Mean postmortem salicylate serum levels on 16 patients who presented dead on arrival after aspirin overdose were 51 mg/dL (range 17 to 101 mg/dL) [55]. Postmortem examination of salicylate-poisoned patients demonstrated several unique findings including myocardial necrosis suggestive of toxic myocarditis [57], pulmonary congestion, hemorrhagic gastritis with unabsorbed salicylate and GI ulceration, cerebral edema, and paratonia (extreme muscle rigidity) [55,56]. Emergency department evaluation of the salicylate-poisoned patient Done nomogram The aspirin nomogram, commonly referred to as the Done nomogram, after its creator Done [58,59], was first published in 1960. Data from pediatric patients who ingested a one-time dose of aspirin were plotted over time to create an instrument to predict toxicity. Several important limitations exist with regards to the development of the Done nomogram that limit its generalizability, including the fact that patients who had polydrug ingestion were included in the analysis, making the clinical correlation difficult to interpret. In addition, the nomogram assumed an elimination MANAGEMENT OF THE SALICYLATE-POISONED PATIENT 339 half-life of 20 hours in all patients and did not allow for the change from first-order to zero-order elimination kinetics that occurs when serum levels exceed the elimination enzyme systems [60]. Although innovative and often accurate for the intended (pediatric) population, the Done nomogram has been demonstrated to have very limited applicability and usefulness for most aspirin-poisoned patients, and its routine use is discouraged [49]. Laboratory evaluation Physicians should make liberal use of blood tests in the evaluation of potentially aspirin-poisoned patients. Different clinical laboratories may report salicylate levels in different units of measure (mg/dL versus mmol/L). Clinicians should maintain consistent use of the respective units of measure to avoid confusion. Seriously aspirin-poisoned patients may display symptoms that allow an astute practitioner to perform comparative serial examinations and assess developing toxicity. Accurate recognition of worsening signs of toxicity, however, is an inexact science with uncertain sensitivity and specificity, especially in the event of polypharmaceutical ingestion or pediatric patients [45,61–63]. Serum salicylate levels frequently do not reflect the severity of the poisoning. Depending on the time since ingestion, presence of food in the stomach, coingestants, and presence of concretions, among other variables, symptoms may or may not correlate with serum salicylate levels. Symptomatic patients suspected of aspirin ingestion or salicylate poisoning should have serial aspirin levels and blood gas analysis performed until a clear trend toward decreasing (not plateau or modestly increasing) levels and metabolic stability as described by the blood gas is present. Radiographic evaluation of the aspirin poisoned patient is rarely helpful, except for seriously ill patients who may have pulmonary edema or patients who have altered mental status that might require CT scanning of the head to eliminate the possibility of an alternative cause for a changed level of consciousness. Large bezoars of ingested enteric-coated aspirin tablets may or may not be visible on a radiograph, and the absence of opacity on an abdominal radiograph is not adequate to rule out the presence of a large amount of salicylate in the gut [64]. Treatment of the salicylate-poisoned patient Resuscitation Depending on the acuity of the poisoning and the presence of end-organ injury and hemodynamic instability, patients may require early, aggressive resuscitation and treatment. Most patients who have consequential aspirin overdose will be somewhat volume deficient because of fluid losses caused by increased respiration, fever, and metabolic activity [15a]. Volume resuscitation with alkalinized intravenous fluids is reasonable and advisable and 340 O’MALLEY should be initiated early in the course of the patient’s treatment so that valuable time is not lost waiting for laboratory confirmation of elevated salicylate levels [65]. Begin by placing a sufficient volume of sodium bicarbonate (three ampules NaHCO3 with 44 mEq Naþ/ampule) into a liter of a glucose-containing hypotonic solution, such as 5% dextrose and water and infusing at 2 to 3 mL/kg per hour to promote brisk urine output. A total of 40 mEq of KCl per liter should be added to prevent hypokalemia. Salicylate-poisoned patients who require advanced airway management are particularly challenging. Salicylate-intoxicated patients who have depressed mental status from the salicylate-induced cerebral hypoglycemia or acidosis or coingestants who require endotracheal intubation and mechanical ventilation pose a clinical no-win situation for emergency physicians, because positive pressure ventilation simply cannot maintain the respiratory rate and metabolic demands of seriously salicylate-poisoned patients. Hemodynamic instability and worsening of acid–base status will almost definitely be the consequence [66]. Patients who require endotracheal intubation for airway protection and maintenance almost always should be hemodialyzed simultaneously to remove salicylate and the accumulated organic acids. Careful attention to maintaining a favorable acid–base status through the judicious manipulation of ventilator settings should occur so as not to allow hypoventilation and the accumulation of CO2. Gastric decontamination The unique characteristics of aspirin in the stomach make gastric decontamination particularly problematic. Gastric irritation, induction of nausea, and decreased mental alertness all combine to put the salicylate-poisoned patient at substantial risk for vomiting and aspiration from any attempt at GI decontamination. Clinicians must weigh the very real risk of aspiration versus the possible benefits from any method of gastric decontamination. Activated charcoal has been demonstrated to be effective in decreasing the area under the curve for absorbed aspirin, and it is the most widely used method of gastric decontamination for salicylate-poisoned patients [67,68]. Multidose activated charcoal similarly has been shown to reduce absorption of aspirin and results in decreased serum levels, but this has not translated into an improved morbidity or mortality rate [69]. Given that multiple doses of activated charcoal are quite safe and generally well tolerated and seem to result in lower total body burden of aspirin, it is reasonable to recommend 25 g of activated charcoal without sorbitol given orally every 3 hours while the patient is being monitored with serial aspirin and blood gas measurements. Before each 25 g dose of activated charcoal, bowel sounds should be checked, and if absent, the activated charcoal should not be withheld. Whole-bowel irrigation is not recommended in aspirin-poisoned patients, because there are very little data to support its use in salicylate poisoning. MANAGEMENT OF THE SALICYLATE-POISONED PATIENT 341 What data do exist do not demonstrate an improved outcome [70,71]. Whole-bowel irrigation with balanced electrolyte solutions decreases gut transit time but may increase total surface area available for absorption and possibly lead to increased serum levels of aspirin. It is universally poorly tolerated and difficult to perform [70,71]. Gastric lavage largely has been abandoned in the management of poisoned patients with the possible exception of overdose with a life-threatening drug and early presentation of the patient in the course of the poisoning [72–74]. Serious aspirin poisoning is certainly a life threat and given the unique potential of enteric-coated aspirin to form concretions and remain in the stomach due to pylorospasm [22], it is reasonable to consider gastric lavage with a large-bore endogastric tube (36 French or larger) if substantial salicylate poisoning is suspected, and there is no likelihood of airway compromise [74–76]. Enhanced elimination Restoring intravascular volume and alkalinization of the serum and urine is an important first-line treatment for acetasalicylic acid toxicity. Bicarbonate diuresis is the mainstay and first-line treatment for aspirin toxicity, and it should be initiated early in every case of moderate salicylate poisoning [65]. The (pKa) is a logarithmic function, so a small change in urine pH will have a disproportionately larger effect on salicylate clearance, so theoretically elimination of salicylic acid is increased substantially in alkaline urine [77]. The most practical method of creating an isotonic alkaline solution in the emergency department is to add sodium bicarbonate to 5% dextrose in water. In general, one 50 mL ampule of 40% sodium bicarbonate should contain 43 mEq of sodium. By putting three ampules (150 mL total volume) of sodium bicarbonate into one liter of D5W, the resulting solution should have 132 mEq of sodium, which is essentially 0.9% (normal) saline [15a]. A total of 40 mEq of KCl per liter should be added to prevent hypokalemia. This solution should be infused rapidly at a rate of at least 2 to 3 mL/kg/hour to maintain a brisk urine output of 1 to 2 mL/kg/hr. The enhanced excretion of salicylate requires not just raising the pH of the urine, but also increasing the glomerular filtration rate [65]. The development of cerebral or pulmonary edema following salicylate poisoning is an important consideration, but a concern for possibly causing these complications should not lead to inadequate or inefficient urinary alkalinization or intravascular volume restoration. Patients who develop worsening respiratory function with increased work of breathing and hypoxia consistent with pulmonary edema or who develop altered or decreased mental status consistent with cerebral edema should have their hydration and urinary alkalinization interrupted and be evaluated immediately for definitive treatment (hemodialysis). 342 O’MALLEY Box 2. Indications for hemodialysis in salicylatedpoisoned patients Severe acidosis or hypotension refractory to optimal supportive care (regardless of absolute serum aspirin concentration) Evidence of end-organ injury (ie, seizures, rhabdomyolysis, pulmonary edema) Renal failure High serum aspirin concentration (>100 mg/dL) despite relatively stable metabolic picture Consider for patients who require endotracheal intubation unless that indication for mechanical ventilation is respiratory depression secondary to a coingestant. Potassium replacement long has been an important aspect of urinary alkalinization despite a paucity of clinical evidence to support the routine practice [15a]. Chronic potassium depletion causes increased reabsorption of bicarbonate in the proximal renal tubules and difficulty achieving an alkaline urine. The effects of acute potassium depletion on urinary excretion of bicarbonate are uncertain [78]. It seems reasonable to infuse potassium and NaHCO3 simultaneously, especially in patients who are already hypokalemic. Urinary alkalinization should be delayed while attempts are made to replace the serum potassium [15a]. Hemodialysis is the definitive treatment to prevent and treat salicylateinduced end-organ injury [79]. Indications for dialysis are listed in Box 2. Hemodialysis will remove aspirin in the serum and lactate efficiently [80]. Patients may have metabolized their aspirin and have a low measured serum concentration of salicylate, but they still may benefit from hemodialysis to remove the byproducts of mitochondrial poisoning. Charcoal hemoperfusion is not practical in most circumstances [81], and hemodialysis has become the preferred method of enhanced elimination of excess serum salicylate. Summary Aspirin carries both significant adverse effects in therapeutic doses and a substantial risk in overdose, for which there is no antidote. Its risk-benefit profile is probably the poorest of all analgesics currently available over the counter; this is reflected in current trends in analgesic use and overdose figures [8] Emergency physicians must have a healthy respect for the erratic and unpredictable absorption and elimination kinetics of aspirin, the devastating physiologic effects of aspirin overdose and the subtle manifestations, MANAGEMENT OF THE SALICYLATE-POISONED PATIENT 343 presentation, and increased mortality of chronic aspirin toxicity. Consultation with the regional poison control center is advised to assist with the management and follow-up of all poisoned patients. References [1] Hedner T, Everts B. The early clinical history of salicylates in rheumatology and pain. Clin Rheumatol 1998;17(1):17–25. [2] Mueller RL, Scheidt S. History of drugs for thrombotic disease. Discovery, development, and directions for the future. Circulation 1994;89(1):432–49. [3] Hare LG, Woodside JV, Young IS. Dietary salicylates. Journal of Clinical Pathology 2003; 56:649–50. [4] Fink CW. Acute versus chronic salicylate poisoning. Pediatrics 1983;71(5):862–3. [5] Flomenbaum N. Salicylates. In: Goldfrank LR, Flomenbaum N, Lewin N, editors. Goldfrank’s toxicologic emergencies. 7th edition. New York: McGraw-Hill Medical Publishing Division; 2003. p. 513. [6] Vivian AS, Goldberg IB. Recognizing chronic salicylate intoxication in the elderly. Geriatrics 1982;37(11):91–7. [7] Anderson RJ, Potts DE, Gabow PA, et al. Unrecognized adult salicylate intoxication. Ann Intern Med 1976;85(6):745–8. [8] Jones A. Over-the-counter analgesics: a toxicologic perspective. Am J Ther 2002;9(3): 245–57. [9] Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18,820 patients. BMJ 2004;329(7456):15–9. [10] Wazaify M, Kennedy S, Hughes CM, et al. Prevalence of over-the-counter drug-related overdoses at accident and emergency departments in Northern Irelandda retrospective evaluation. J Clin Pharm Ther 2005;30(1):39–44. [11] Watson WA, Litovitz TL, Rodgers GC Jr, et al. 2004 Annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Am J Emerg Med 2005;23(5):589–666. [12] Gittelman DK. Chronic salicylate intoxication. South Med J 1993;86(6):683–5. [13] Rodgers GB. The effectiveness of child-resistant packaging for aspirin. Arch Pediatr Adolesc Med 2002;156(9):929–33. [14] Hawton K, Simkins S, Decks J, et al. UK legislation on analgesic packs: before-and-after study of long-term effect on poisonings. BMJ 2004;329(7474):1076. [15] Sheen CL, Dillon JF, Bateman DN, et al. Paracetamol pack size restriction: the impact on paracetamol poisoning and the over-the-counter supply of paracetamol, aspirin, and ibuprofen. Pharmacoepidemiol Drug Saf 2002;11(4):329–31. [15a] Yip L, Dart RC, Gabrow PA. Concepts and controversies in salicylate toxicity. Emerg Med Clin N Am 1994;12(2):351–64. [16] Petrescu I, Tarba C. Uncoupling effects of diclofenac and aspirin in the perfused liver and isolated hepatic mitochondria of rat. Biochim Biophys Acta 1997;1318(3):385–94. [17] Krause DS, Wolf BA, Shaw LM. Acute aspirin overdose: mechanisms of toxicity. Ther Drug Monit 1992;14(6):441–51. [18] Temple AR. Pathophysiology of aspirin overdosage toxicity, with implications for management [review]. Pediatrics 1978;62(5 Pt 2 Suppl):873–6. [19] Leatherman JW, Schmitz PG. Fever, hyperdynamic shock, and multiple-system organ failure. A pseudo-sepsis syndrome associated with chronic salicylate intoxication. Chest 1991; 100(5):1391–6. [20] Schwartz R, Landy G. Organic acid excretion in salicylate intoxication. J Pediatr 1965;66: 658–66. 344 O’MALLEY [21] Hill JB. Salicylate intoxication. N Engl J Med 1973;288:1110–3. [22] Rivera W, Kleinschmidt KC, Velez LI, et al. Delayed salicylate toxicity at 35 hours without early manifestations following a single salicylate ingestion. Ann Pharmacother 2004;38(7–8): 1186–8. [23] Myers B, Evans DN, Rhodes J, et al. Metabolism and urinary excretion of 5-amino salicylic acid in healthy volunteers when given intravenously or released for absorption at different sites in the gastrointestinal tract. Gut 1987;28:196–200. [24] Schanker LS, Tocco DJ, Brodie BB, et al. Absorption of drugs from the rat small intestine. J Pharmacol Exp Ther 1958;123(1):81–8. [25] Singh P, Roberts MS. Dermal and underlying tissue pharmacokinetics of salicylic acid after topical application. J Pharmacokinet Biopharm 1993;21(4):368–70. [26] Singh P, Roberts MS. Skin permeability and local tissue concentrations of nonsteroidal antiinflammatory drugs after topical application. J Pharmacol Exp Ther 1994;268(1):144–51. [27] Cross SE, Anderson C, Roberts MS. Topical penetration of commercial salicylate esters and salts using human isolated skin and clinical microdialysis studies. Br J Clin Pharmacol 1998; 46(1):29–35. [28] Martin D, Valdez J, Boren J, et al. Dermal absorption of camphor, menthol, and methyl salicylate in humans. J Clin Pharmacol 2004;44:1151–7. [29] Bell AJ, Duggin G. Acute methyl salicylate toxicity complicating herbal skin treatment for psoriasis. Emerg Med (Fremantle) 2002;14(2):188–90. [30] Lebwohl M. The role of salicylic acid in the treatment of psoriasis. Int J Dermatol 1999;38(1): 20–2. [31] Taylor JR, Halprin KM. Percutaneous absorption of salicylic acid. Arch Dermatol 1975; 111(6):740–3. [32] Martin L. All you really need to interpret arterial blood gases. 2nd edition. Philadelphia: Lippincott, Williams and Wilkins; 1999. [33] Chrichton JU, Elliott GB. Salicylateda dangerous drug in infancy and childhood. Can Med Assoc J 1960;83:1144. [34] Done AK. Treatment of salicylate poisoning: review of personal and published experiences. Clin Toxicol 1968;1:451. [35] Gaudreault P, Temple AR, Lovejoy FH. The relative severity of acute versus chronic salicylate poisoning in children: a clinical comparison. Pediatrics 1982;70:567–8. [36] Jepsen F, Ryan M. Poisoning in children. Current Paediatrics 2005;15(7):563–8. [37] Wrathall G, Sinclair R, Moore A, et al. Three case reports of the use of haemodiafiltration in the treatment of salicylate overdose. Hum Exp Toxicol 2001;20(9):491–5. [38] Grabe DW, Manley HJ, Kim JS, et al. Respiratory distress caused by salicylism confirmed by lung biopsy. Clin Drug Investig 1999;17(1):79–81. [39] Proudfoot AT. Toxicity of salicylates. Am J Med 1983;75(Suppl):100–2. [40] Cazals Y. Auditory sensori-neural alterations induced by salicylate. Prog Neurobiol 2000; 62(6):583–631. [41] Wecker H, Laubert A. Reversible hearing loss in acute salicylate intoxication. HNO 2004; 52(4):347–51. [42] Mongan E, Kelly P, Nies K, et al. Tinnitus as an indication of therapeutic serum salicylate levels. JAMA 1973;226(2):142–5. [43] Taylor JR, Streetman, DS, Castle SS. Medication bezoars: a literature review and report of a case. Ann Pharmacother 1998;32(9):940–6. [44] Stack PE, Thomas E. Pharmacobezoar: an evolving new entity. Dig Dis 1995;13(6):356–64. [45] Gabow PA, Anderson RJ, Potts DE, et al. Acid–base disturbances in the salicylate-intoxicated adult. Arch Intern Med 1978;138:1482–3. [46] Dale C, Aulaqi AA, Baker J, et al. Assessment of a point-of-care test for paracetamol and salicylate in blood. QJM 2005;98(2):113–8. [47] Graham CA, Irons AJ, Munro PT. Paracetamol and salicylate testing: routinely required for all overdose patients? Eur J Emerg Med 2006;13(1):26–8. MANAGEMENT OF THE SALICYLATE-POISONED PATIENT 345 [48] Wood DM, Dargan PI, Jones AL. Measuring plasma salicylate concentrations in all patients with drug overdose or altered consciousness: is it necessary? Emerg Med J 2005;22(6):401–3. [49] Dugandzic RM, Tierney MG, Dickinson GE, et al. Evaluation of the validity of the Done nomogram in the management of acute salicylate intoxication. Ann Emerg Med 1989;18: 1186–90. [50] Chalasani N, Roman J, Jurado RL. Systemic inflammatory response syndrome caused by chronic salicylate intoxication. South Med J 1996;89(5):479–82. [51] Paul BN. Salicylate poisoning in the elderly: diagnostic pitfalls. J Am Geriatr Soc 1972;20: 388–9. [52] Bailey RB, Jones SR. Chronic salicylate intoxication: a common cause of morbidity in the elderly. J Am Geriatr Soc 1989;37:556. [53] Steele TE, Morton WA. Salicylate-induced delirium. Psychosomatics 1986;27:455–6. [54] Dargan PI, Wallace CI, Jones AL. An evidence-based flowchart to guide the management of acute salicylate (aspirin) overdose. Emerg Med J 2002;19:206–9. [55] McGuigan MA. A two-year review of salicylate deaths in Ontario. Arch Intern Med 1987; 147:510–2. [56] Thisted B, Krantz T, Stroom J. Acute salicylate self-poisoning in 177 consecutive patients treated in ICU. Acta Anaesthesiol Scand 1987;31(4):312–6. [57] Pena-Alonso YR, Montoya-Cabrera MA, Bustos-Cordoba E. Aspirin intoxication in a child associated with myocardial necrosis: Is this a drug-related lesion? Pediatr Dev Pathol 2003;3: 342–7. [58] Done AK. Salicylate intoxication: significance of measurements of salicylate in blood in cases of acute ingestion. Pediatrics 1960;26:805–6. [59] Done AK. Aspirin overdosage: incidence, diagnosis, and management. Pediatrics 1978; 62(Suppl):890–7. [60] Kulig K. Salicylate intoxication: is the Done nomogram reliable? [Comment in AACT] Clinical Toxicology UPDATE 1990;3(2):2–3. [61] Chabali R. Diagnostic use of anion and osmolal gaps in pediatric emergency medicine. Pediatr Emerg Care 1997;13(3):204–10. [62] Litovitz T, Manoguerra A. Comparison of pediatric poisoning hazards: an analysis of 3.8 million exposure incidents. A report from the American Association of Poison Control Centers. Pediatrics 1992;89(6 Pt 1):999–1006. [63] Mitchell AA, Lovejoy FH Jr, Slone D, et al. Acetaminophen and aspirin. Prescription, use, and accidental ingestion among children. Am J Dis Child 1982;136(11):976–9. [64] Erzurumlu K, Malagirt Z, Bektas A, et al. Gastrointestinal bezoars: a retrospective analysis of 34 cases. World J Gastroenterol 2005;11(12):1813–7. [65] Proudfoot AT, Krenzelok EP, Vale JA. Position paper on urine alkalinization. J Toxicol Clin Toxicol 2004;42(1):1–26. [66] Greenberg MI, Hendrickson RG, Hofman M. Deleterious effects of endotracheal intubation in salicylate poisoning. Ann Emerg Med 2003;41(4):583–4. [67] Kirshenbaum LA, Mathews SC, Sitar DS, et al. Does multiple-dose charcoal therapy enhance salicylate excretion? Arch Intern Med 1990;150(6):1281–3. [68] Park GD, Spector R, Goldberg MJ, et al. Expanded role of charcoal therapy in the poisoned and overdosed patient. Arch Intern Med 1986;146(5):969–73. [69] Vale JA, Krenzolak E, Barceloux GD. Position statement and practice guidelines on the use of multidose activated charcoal in the treatment of acute poisoning. American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. J Toxicol Clin Toxicol 1999;37(6):731–51. [70] Lheureux P, Tenenbein M. Position paper: whole bowel irrigation. J Toxicol Clin Toxicol 2004;42(6):843–54. [71] Tenenbein M. Position statement: whole bowel irrigation. American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. J Toxicol Clin Toxicol 1997;35(7):753–62. 346 O’MALLEY [72] Daly FF, Little M, Murray L. A risk assessment-based approach to the management of acute poisoning. Emerg Med J 2006;23(5):396–9. [73] Heard K. The changing indications of gastrointestinal decontamination in poisonings. Clin Lab Med 2006;26(1):1–12, vii. [74] Worthley LI. Clinical toxicology: part I. Diagnosis and management of common drug overdosage. Crit Care Resusc 2002;4(3):192–215. [75] Heard K. Gastrointestinal decontamination. Med Clin North Am 2005;89(6):1067–78. [76] Osterhoudt KC, Durbin D, Alpern ER, et al. Risk factors for emesis after therapeutic use of activated charcoal in acutely poisoned children. Pediatrics 2004;113(4):806–10. [77] Proudfoot AT, Krenzelok EP, Brent J, et al. Does urinary alkalinization increase salicylate elimination? If so, why? Toxicol Rev 2003;22(3):129–36. [78] Chang YL, Biagi B, Giebish G. Control mechanism for bicarbonate transport across the rat proximal convoluted tubule. Am J Physiol 1982;242:532–43. [79] Lund B, Seifert SA, Mayersohn M. Efficacy of sustained low-efficiency dialysis in the treatment of salicylate toxicity. Nephrol Dial Transplant 2005;20(7):1483–4. [80] Higgins RM, Connolly JO, Hendry BM. Alkalinization and hemodialysis in severe salicylate poisoning: comparison of elimination techniques in the same patient. Clin Nephrol 1998; 50(3):178–83. [81] Shalkham AS, Kirrane BM, Hoffman RS, et al. The availability and use of charcoal hemoperfusion in the treatment of poisoned patients. Am J Kidney Dis 2006;48(2):239–41.