Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
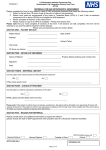
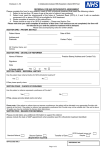
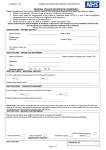
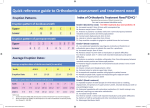
Birmingham Community Healthcare NHS Trust BCHC Orthodontic Services – Referral Form Patient details Practice details Name Referrer’s name and address Address Postcode GDP name and address (if different to above) Telephone no. D.O.B Gender Clinical details (continue on separate sheet if necessary) Relevant medical history Relevant dental history Main reason for referral Decide if a malocclusion has an IOTN above 3.6 and then decide if referral should be to primary care or hospital using the following grid: Feature Primary Care Specialist Services Hospital Services Impacted or ectopic teeth Mild Moderate/severe One tooth missing in More than one tooth missing Missing teeth (not 8s) any quadrant per quadrant Overjet ≤ 10mm > 10 mm Reverse overjet Reverse overjet ≤ 3mm Reverse overjet > 3mm Lateral or anterior open bite ≤ 4mm > 4mm Supernumerary teeth Erupted Unerupted Submerging primary teeth Mild Moderate/severe Craniofacial anomalies Hospital service Cleft lip and palate Hospital service Complicating medical history Hospital service Tooth structure anomalies Hospital service Crossbites ≤ 4mm shift > 4mm shift Crowding Moderate/severe Very severe Are dentally fit and have good OH Please ensure all patients Are the correct age referred for active treatment Understand clearly what treatment involves Are highly motivated to support treatment If recent radiographic films exist (taken in the past year), hard copy images must be enclosed or alternatively send digital radiographs via NHS.net or attach an encrypted DVD or CD. Have radiographs been taken in the last year? Referring Practitioner signature Yes No Radiographs enclosed? Yes No Date Please read the accompanying guidance and select the appropriate orthodontic provider to refer to. Produced by Clinical Photography and Graphic Design Tel: 0121 466 5107 Ref: 43950 16.02.2015 Malocclusion – You must indicate the main feature otherwise the referral may NOT be accepted