Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
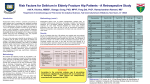
28 February 2014 No.07 POSTOPERATIVE DELIRIUM ’’Grannies gone wild” ZN Moyce Moderator: Kim de Vasconcellos School of Clinical Medicine Discipline of Anaesthesiology and Critical Care CONTENTS INTRODUCTION ................................................................................................... 3 DEFINITION .......................................................................................................... 3 CLASSIFICATION ................................................................................................ 5 INCIDENCE .......................................................................................................... 5 PATHOPHYSIOLOGY .......................................................................................... 5 RISK FACTORS ................................................................................................... 6 DIAGNOSIS .......................................................................................................... 8 OUTCOME/SEQUELAE ..................................................................................... 11 PREVENTION ..................................................................................................... 11 META-ANALYSIS FINDINGS ............................................................................. 12 TREATMENT ...................................................................................................... 18 RECOMMENDATIONS ....................................................................................... 19 WHAT’S ON THE HORIZON .............................................................................. 19 CONCLUSION .................................................................................................... 20 REFERENCES.................................................................................................... 21 Page 2 of 24 POSTOPERATIVE DELIRIUM ’’GRANNIES GONE WILD” INTRODUCTION As the global population ages, so the number of elderly patients with more comorbidities requiring surgical interventions and procedures is increasing[1-3] These patients represent a significant proportion of the estimated annual 200 million surgeries conducted globally[4]. Cognitive decline is one of the common causes of functional impairment worldwide and central nervous system dysfunction is a recognised complication that can occur following both cardiac and non-cardiac surgery[1,3]. The word ‘delirium’ is derived from the Latin term meaning “off the track” and was described by Hippocrates more than 2500 years ago[5]. Postoperative delirium (POD) is one of the most frequently encountered perioperative complications. It is an acute impairment of cognition and or perception, which can be diagnosed at the bedside with specific diagnostic tools. It is a complex disease and often multifactorial, therefore POD continues to be underdiagnosed and poorly managed[6]. POD has a classic fluctuating course, most commonly days 1 to 3 postoperatively with symptoms worse at night [7, 8]. If not systematically tested for POD can be easily overlooked and early diagnosis and resolution is likely to produce the most favorable outcomes [7, 9]. DEFINITION There are two standard definitions used for delirium (DSM IV-TR/ DSM V) : an acute and fluctuating disturbance of consciousness with signs of inattention, accompanied by a change in cognition and perception (Table 1) [10, 11]; or (ICD 10) an aetiologically non-specific organic cerebral syndrome characterized by concurrent disturbances of consciousness and attention, perception, thinking and memory, including disturbances of emotion, psychomotor and the sleep–wake cycle (Table 2) [12]. Page 3 of 24 Table 1: Diagnostic criteria of the DSM-V for postoperative delirium[11] The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) diagnostic criteria for delirium A: Disturbance in attention (ie, reduced ability to direct, focus, sustain, and shift attention) and awareness. B: Change in cognition (eg, memory deficit, disorientation, language disturbance, perceptual disturbance) that is not better accounted for by a preexisting, established, or evolving dementia. C: The disturbance develops over a short period (usually hours to days) and tends to fluctuate during the course of the day. D: There is evidence from the history, physical examination, or laboratory findings that the disturbance is caused by a direct physiologic consequence of a general medical condition, an intoxicating substance, medication use, or more than one cause Table 2: ICD-10 definition for postoperative delirium[12] ICD-10 definition of postoperative delirium An aetiologically non-specific organic cerebral syndrome characterized by concurrent disturbances of consciousness and attention, perception, thinking, memory, psychomotor behavior, emotion and the sleep-wake schedule. The duration is variable and the degree of severity ranges from mild to very severe Includes: Brain syndrome, Confusional state (non-alcoholic), Infective psychosis, Organic reaction, Psycho-organic syndrome Excludes: Delirium tremens, alcohol induced or unspecified Page 4 of 24 CLASSIFICATION [1,5-7,13-19] Delirium can be classified into three subtypes: Hyperactive: most frequently recognized form as it is characterized by agitation, aggression acute disorientation, restlessness, hallucinations and emotional liability. It has been associated with increased use of benzodiazepines, oversedation and physical restraints. Hypoactive: occurs more commonly, but is often unrecognized as the patient usually presents with a flat affect and is withdrawn, lethargic, and quiet, but disoriented and confused. This is however associated with prolonged hospitalization and secondary complications. Mixed: a combination of hyperactive and hypoactive types in which the patient’s behaviors fluctuate from agitated to calm moods commonly associated with daytime sedation and nighttime agitation. Sub-syndromal delirium: patient displays one or more symptoms of delirium but do not meet the defined criteria INCIDENCE There is a wide variation in the reported incidence of delirium ranging from 0-73% depending on patient population and the type of surgery [6, 8, 9]. The incidence of POD following major orthopaedic surgery can range from 16-62% [8]. The incidence is higher in patients with terminal illnesses like cancer or AIDS/HIV related illness and extensive surgical stress [6, 8]. PATHOPHYSIOLOGY[1, 3, 5, 13, 16-18] The pathophysiological mechanisms of POD are not fully understood, however it is probably multifactorial and includes some or all of the various hypotheses given below. Neurotransmittor theory: decrease in oxidative metabolism of the brain causes a decrease in neurotransmittors which causes neuronal dysfunction. Neurotransmittors implicated are acetylcholine, dopamine, gamma-aminobutyric acid (GABA), tryptophan, melatonin and serotonin. Increased levels of dopamine and decreased production of acetylcholine can lead to neuronal excitability which can precipitate delirium. Medication theory: perioperative drugs and associated neurotoxicity. Age related changes to the blood brain barrier (BBB) could affect the permeability of the BBB and alter the entry of drugs into the CNS. Page 5 of 24 Surgical theory: inflammation from both anesthetics and surgical interventions as the aetiology of neuronal changes. Stress responses, release of inflammatory cytokines, increased circulation of cortisol, and sleep deprivation are believed to cause changes in neuronal pathways triggering delirium. Impaired anti-inflammatory feedback of the aged brain can cause exaggerated or prolonged production of cytokines.In animal studies they found increased expression of interleukin 1β was associated with cognitive decline. The inflammatory process can also lead to a prothrombotic state which can lead to decreased cerebral blood flow. Patient theory: factors such as frailty and any preoperative cognitive deficits. Environmental theory: disorientation and unfamiliar surroundings as the contributory factor in POD RISK FACTORS Although the mechanism of POD is not completely understood, there are significant details in literature describing associated perioperative risk factors. A list of the most common conditions/stressors is given below. Specific attention should be paid to identifying and correcting these risk factors if possible (Table 36) [6,7 9,13]. Table 3: A list of preoperative risk factors for postoperative delirium [6, 7, 9, 13] Demographic related: Age >70 years Male sex Low education level Malnutrition Alcohol and drug use Comorbidities related: Preoperative cognitive and physical status Renal or hepatic disease HPT, DM, PVD, CCF, OSA, CVA Hb <10 Smoking, COPD Low albumin Abnormal electrolytes, glucose Hearing or visually impaired Surgery related: Anaesthetic related: Aortic aneurysm, cardiac, Fasting time > 6hrs thoracic, abdominal, Use of premedication: cataract and hip benzodiazepines replacement surgery Use of anticholinergic agents ASA III –IV Page 6 of 24 Table 4: A list of intraoperative risk factors for postoperative delirium [6 7,9,13] Surgery related: Anaesthetic related: Prolonged surgery Hypotension Blood loss >1L Hypoxia, hypocarbia, hypercarbia Hypothermia Use of ketamine, benzodiazepines, propofol Long acting opioids Embolism Table 5: A list of postoperative risk factors for postoperative delirium Pain Sepsis Hypotension requiring vasopressors Hypoxia requiring ventilation Electrolyte or metabolic abnormalities Sensory deprivation or overload Sleep deprivation Anxiety Restraints and catheters Page 7 of 24 [6, 7, 9, 13] Table 6: A list of drugs associated with postoperative delirium[5] Memory aid for delirium precipitants – think DELIRIUM Drugs (withdrawal/toxicity, anticholinergics)/Dehydration Electrolyte imbalance Level of pain Infection/Inflammation (post surgery) Respiratory failure (hypoxia, hypercapnia) Impaction of faeces Urinary retention Metabolic disorder (liver/renal failure, hypoglycaemia) Myocardial infarction DIAGNOSIS To assess the patient’s degree of cognitive impairment, it is vital to have established a baseline for comparison. Therefore, a good preoperative evaluation should include a formal cognitive assessment in patients at risk of developing delirium. DSM IV and ICD 10 are the gold standards but they require expertise and are time consuming[5, 7]. Delirium may be identified with the help of delirium assessment tools like the mini mental state exam (MMSE) (Table 7), the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) and Intensive Care Delirium Screening Checklist (ICDSC)[5, 7, 13]. The MMSE is one of the most widely used tools to test cognition. Although it was not specifically designed for delirium it can be used to assess changes in cognitive function. It is therefore essential to do baseline MMSE testing with repeat testing to assess for changes. A drop of > 2 points from baseline is suggestive of delirium[6, 15]. CAM-ICU is the most commonly used tool. It has high sensitivity and specificity, a rapid assessment tool <5 minutes and its easy to use. Page 8 of 24 When used in ICU it is utilized in conjunction with the Richmond Agitation and Sedation score (RASS) and should be performed daily on patients at risk of POD (Figure 1) [6,7,9,13,15] Table 7: Criteria of the mini mental state exam[17] Points Orientation Name: season/date/day/month/year 5 (1 for each) Name: hospital/floor/town/province/country 5 (1 for each) Registration Identify 3 objects by name and ask patient to repeat it 3 (1 for each) Attention and calculation Serial 7s (subtract from 100-5 subtractions) 5 (1 for each) Recall Recall the 3 objects presented earlier 3 (1 for each) Language Name pencil and watch 2 (1 for each) Repeat “No ifs, ands or buts” 1 Follow 3 step command (take this paper, fold it in half and place it on the table) 3 (1 for each) Write “close your eyes” and ask patient to obey written command 1 Ask patient to write a sentence 1 Ask patient to copy a design (intersecting pentagons) 1 TOTAL 30 Memory aid mnemonic for CAM - think CA2MS: Delirium diagnosis requires CA2 and either M or S Changeable course Acute onset + Attention poor Muddled thinking Shifting consciousness Page 9 of 24 Figure 1: Chart for the stepwise approach to diagnosing delirium[13] Page 10 of 24 OUTCOME/SEQUELAE Postoperative delirium (POD) is associated with serious postoperative complications, which decrease functional capacity, prolong recovery and discharge, and directly increase healthcare costs. Patients suffering delirium have increased numbers of surgical complications, including fractures (due to falls), urinary and respiratory tract infections, and vascular events. Delirium also increases long-term morbidity through delayed functional and cognitive recovery, subsequent institutionalisation and postoperative depression [3, 5, 9, 13, 15, 16] Radtke et al found that delirium was associated with a higher incidence of postoperative cognitive dysfunction at 7 days and 3 months postoperative [20]. PREVENTION Due to the multifactorial nature of POD the approach to prevention of POD needs to be multi-interventional. Preoperative prevention [6, 7, 17, 21] Detailed preoperative history Detailed drug history Detection of any sensory or perceptual deficits Identifying patients at risk is essential and a comprehensive preoperative assessment is vital to provide possible causes that could increase the risk of POD. It’s important to note any pre-operative cognitive impairments and a patient with pre-exising sensory or perceptual deficits is likely to have an increased chance of POD developing. By identifying these high risk patients we should then ensure that all intraoperative and postoperative strategies are adhered to. Preoperative prediction scores assist in identifying these high risk patients but can’t be used to exclude the possiblilty of delirium developing postoperatively (Table 8) [17, 21]. Table 8: Preoperative prediction scores for delirium for both cardiac and noncardiac surgery Intraoperative prevention [6, 9, 17, 19, 21]: Ensure adequate oxygenation and perfusion Correct any electrolyte imbalances Adjust drug doses accordingly Avoid anticholinergic agents Postoperative prevention [6, 7, 13, 21]: Provide visual and hearing aids when appropriate Early mobilisation Orientation Family visits Sleep hygiene Adequate pain management Aviod volume depletion and electrolyte abnormalities In ICU: sedation hold Daily delirium monitoring META-ANALYSIS FINDINGS [22] Despite advances in both perioperative care and surgical interventions, geriatric patients still experience POD. POD is associated with an increase in both morbidity and mortality and had a direct burden on health care costs and resources[1,8,14,23]. Page 12 of 24 Outcomes of POD could be improved by systematic identification of important risk factors for delirium and identification of preventative measures that decrease the incidence of delirium and the subsequent associated morbidity [24]. It is still not clear which are the most effective interventions to decrease POD so we planned to look at perioperative interventions to decrease delirium in noncardiac surgery. The purpose of our systematic review and meta-analysis was to determine the efficacy of both pharmacological and non-pharmacological perioperative interventions to decrease delirium. Method We posed the following research question: ‘Which peri-operative interventions during non-cardiac surgery have been independently associated with a reduction in delirium within the first seven postoperative days?’ Trials were considered eligible if they tested a peri-operative intervention aimed at reducing delirium after non-cardiac surgery in a randomised controlled manner. The primary outcome was the incidence of delirium within seven days of surgery. An electronic search of four databases was conducted. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were adhered to[25]. We included randomised controlled trials of non-cardiac surgery with a peri-operative intervention and that reported postoperative delirium, and identified 29 trials. A manual search of the reference lists of all included papers was also conducted for further eligible studies. Concordance of article extraction was determined using a kappa statistic.Using a standardised data extraction sheet, we extracted data on: the outcome of delirium following a peri-operative intervention; the specific intervention tested; patient age; type of surgery; and the use of premedication. The quality of each study was assessed using the Jadad score[26] Meta-analysis was conducted using Review Manager Version 5.1 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark, 2011). Heterogeneity between studies was assessed using univariate chi-squared analysis. Random or fixed effects models were used based on the presence or absence of significant heterogeneity between studies, respectively. Pooled dichotomous outcomes were reported as odds ratios (OR) with 95% CI. Where an intervention was associated with benefit, a funnel plot was constructed to determine if the outcomes reported were affected by publication bias. For interventions that were not significantly associated with a decrease in delirium, a power analysis was conducted to determine if the sample size was adequately powered for the outcome. The power analysis was based on the incidence in the control group, with an expected 25% relative risk reduction for an efficacious intervention. Page 13 of 24 Results We identified 1376 studies from our literature search, of which 56 studies were selected for full paper analysis; the kappa statistic was 83%. From these studies, 29 were finally included in our meta-analysis (Fig.1). Nineteen of the studies were of a high quality with a Jadad score of 4 or 5 [16– 34], and 10 were low-quality studies with a Jadad score < 4. The following interventions to decrease delirium were tested in more than one trial and a meta-analysis was therefore possible: geriatric (or multicomponent) consultation vs standard care, where peri-operative geriatric consultation constituted a proactive, comprehensive geriatric assessment along with management and rehabilitation to decrease the outcome of delirium[27-29]; deep vs light anaesthesia[30-32]; intravenous vs inhalational anaesthesia [33, 34]; general vs regional anaesthesia[35-37]; haloperidol vs placebo[38-40]; donepezil (a cholinesterase inhibitor) vs placebo[41-43]; gabapentin vs placebo [44, 45]; and bright light therapy vs standard care [46, 47]. Bright light therapy was instituted after extubation of the trachea and study patients received two hours of bright light therapy daily. Only two interventions were associated with significantly decreased delirium: peri-operative geriatric consultation and light as opposed to deep anaesthesia. There was no significant heterogeneity for these two interventions. Figure 2: Flow chart of identification of randomized controlled trials included in the meta-analysis. Potentially relevant studies identified by electronic database search and manual searching (n=1376) Potential studies retrieved for more detailed evaluation (n=56) Selected trials included in meta-analysis (n=29) Letter, editorial, review (n=178) Cardiac (n=375) Non-human (n=1) Non-adult (n=65) No delirium outcome/intervention (n=649) Foreign language (n=52) Duplicates (n=3) No surgical control group/ not RCT (n=6) Same cohort (n=4) Abstract/unable to obtain specific data (n=9) Protocol/ meta-analysis (n=5) Page 14 of 24 Figure 3: Meta-analysis of the efficacy of peri-operative geriatric consultation vs standard care on outcome of postoperative delirium. M-H, Mantel-Haenszel Figure 4: Meta-analysis of the efficacy of depth of anaesthesia vs standard care on outcome of postoperative delirium. M-H, Mantel-Haenszel. For the other interventions, the point estimate suggested possible protection with the use of prophylactic haloperidol, bright light therapy and general as opposed to regional anaesthesia. The power analyses showed that the sample size was inadequate for all the interventions included in the meta-analysis, with the exception of the peri-operative geriatric consultation. Discussion The main findings of this meta-analysis are that perioperative geriatric consultations, which included multicomponent interventions, and lighter as opposed to deeper anaesthesia were effective in decreasing postoperative delirium. The point estimate for perioperative geriatric consultation was robust without heterogeneity, yet these clinical trials are at a high risk of bias due to inadequate randomisation and/or blinding. The point estimate for deep vs light anaesthesia showed significant heterogeneity, and there may be publication bias associated with this intervention. Delirium is a common complication following hip fracture surgery and the three trials of perioperative geriatric consultations were conducted in this population. Page 15 of 24 Multi-component and systemic assessment addressed urinary tract infections, hypoxia, anaemia, constipation, sleep disorders and nutritional deficiencies, which may all have a role in the aetiology and duration of delirium[28]. This meta-analysis lends support to multidisciplinary peri-operative medicine interventions to decrease delirium. Delirium is multifactorial, and anaesthetic technique is another potentially modifiable risk factor. Intra-operative monitoring of depth of anaesthesia using bispectral index (BIS) or auditory evoked potentials has shown to facilitate titration of anaesthetic drugs. Bispectral index values between 40 and 60 during anaesthesia have been associated with decreased awareness, earlier recovery profiles and faster emergence[30]. Chan et al. demonstrated that titrating anaesthetic agents to maintain BIS between 40 and 60 and avoiding episodes of deep anaesthesia (BIS < 40) reduced the risk of delirium (p = 0.01)[30]. Sieber et al. found that light sedation (BIS > 80) during spinal anaesthesia for orthopaedic surgery decreased the occurrence of delirium by 50% when compared with deep sedation (BIS ~ 50) (p = 0.02)[48]. Depth of anaesthesia guided by auditory evoked potentials demonstrated that patients with lighter anaesthesia sustained fewer intraoperative events, had higher blood pressure, required less fluids or vasopressors, and were at a lower risk of developing early postoperative decline [31]. Regarding the intra-operative measures that were identified, neither intravenous vs inhalational anaesthesia, nor regional vs general anaesthesia, showed any effect on postoperative delirium. Although both of these analyses were underpowered, the point estimates favoured inhalational and general anaesthesia. In contrast, another meta-analysis of the efficacy of general and regional anaesthesia failed to show a significant difference (five studies), and suggested that general anaesthesia may increase the risk of developing postoperative cognitive dysfunction [49]. Our meta-analysis has found a trend to protection with the use of haloperidol. The dose of haloperidol varied between the studies. Wang et al. used 0.5 mg haloperidol as an intravenous bolus postoperatively, followed by an infusion at 0.1 mg.hr for 12 h; Kaneko et al. administered 5 mg haloperidol intravenously per day for five days, and Kalisvaart et al. used oral haloperidol 1.5 mg pre-operatively and for three days postoperatively[38-40]. A recent meta-analysis conducted by Teslyar et al. looked at antipsychotics as a group (haloperidol, olanzapine and risperidone) and they also showed a trend to a reduction in delirium with the perioperative use of antipsychotics[50] LImitations There are a number of limitations to this meta-analysis. Firstly, of all the possible interventions investigated to decrease delirium, only peri-operative geriatric consultation and light vs deep anaesthesia were adequately powered. It is therefore possible that certain of the other interventions are efficacious; however, further research would be required to confirm this. Page 16 of 24 Secondly, peri-operative geriatric consultation consultation studies were limited to orthopaedic surgery. This research needs to be extended to other non-cardiac surgeries.Furthermore, the nature of multi-component consultations makes it difficult to exclude a strong bias due to poor randomisation and blinding, which is evident in this meta-analysis. In the pharmacological intervention studies, there was no standardisation of the anaesthetic technique. This is an important limitation, as this meta-analysis suggested that depth of anaesthesia may be an important determinant of delirium.Furthermore, there was no standardisation of the dosage of the pharmacological intervention between the trials analysed and this may be an important confounder in some studies. We also excluded foreign language studies, which could have impacted on the results of the meta-analysis. Finally, few studies assessed pre-operative risk for delirium, with no standardization in timing of postoperative testing either. A standardised protocol for pre-operative risk assessment and outcome determination would be desirable in future studies. In conclusion, the main findings of this meta-analysis are that peri-operative geriatric consultations that involve multi-component interventions, and lighter anaesthesia, are potentially effective in decreasing the outcome of delirium. Zhang et al did a systematic review and meta-analysis of randomised controlled trials of strategies to prevent POD. Their review entailed randomised controlled trials for both cardiac and noncardiac surgery[51]. They found that dexmedetomidine sedation; multicomponent interventions and antipsychotics are useful in preventing postoperative delirium[51]. Dexmedetomidine sedation was used postoperatively in cardiac surgery therefore was not included in our analysis. Both studies found huge heterogeneity of the interventions among the trials and that multicomponent (geriatric) interventions were potentially effective in decreasing the outcome of POD [22, 51] Our study only included RCT, which looked at haloperidol in decreasing the outcome, which only indicated a trend to protection whereas Zhang et al found protection with antipsychotics looking at both typical and atypical antipsychotics [22, 51] .Our point estimates favoured inhalational anaesthesia compared to intravenous and general anaesthesia compared to regional anaesthesia [22]. Zhang et al found that type of anaesthesia had no effect on the outcome of delirium[51]. Page 17 of 24 TREATMENT Due to the multifactorial nature of POD, a multicomponent strategy needs to be implemented for adequate treatment. Once the diagnosis of delirium is made, it is vital to exclude any identifiable causes and treat appropriately Non-pharmacological [5-7, 9, 15, 16, 18, 19, 21] Need to optimise the preventive measures orientation sleep hygiene early mobilisation vision and hearing devices adequate pain management remove any lines or catheters do not use unnecessary physical restraints stop any deliriogenic drugs Pharmacological Antipsychotics: Haloperidol is a dopamine receptor antagonist and acts centrally to decrease hallucinations and delirium[18]. Side effects include prolonged QT, extrapyramidal side effects and neuroleptic malignant syndrome. Although the evidence is inconclusive, current recommendation is haloperidol as the agent of choice for the treatment of delirium[5, 7, 15] Studies have shown a decrease in the incidence of POD and a reduction in the severity POD with the use of haloperidol. The dose of haloperidol is determined by route of administration, the age of the patient and the severity of the agitation[5]. High doses of >4.5mg per day are associated with increases in the incidence of adverse effects[6] Haloperidol dosage[15]: ICU: haloperidol 1-2mgIVI repeated every 20min until resolution of agitation. Taper dose over several days. Ward: haloperidol 1mg po/IM/IV stat ; maintenance 0.25-0.5mg 4 hrly. Taper over several days Atypical antipsychotics eg olanzapine/ risperidone are alternative agents. They have however not been shown to be superior to haploperidol in the treatment of delirium[15]. Benzodiazepines The use of benzodiazepines is discouraged perioperatively in patients at risk of delirium. They have a dose dependent association with the incidence of POD. They however have a role in POD associated with withdrawal syndrome due to chronic alcohol or sedative use[5-7, 15] Page 18 of 24 Alpha-2 agonists Perioperative use of dexmedetomidine has been shown to reduce the prevalence of POD in ICU. Zhang et al found that although the studies used in the metaanalysis were poor quality and had inconsistent definitions it still supported the effectiveness of dexmedetomidine sedation in preventing delirium in ICU[51]. Opioids Opioids have an important role in palliation of terminal illnesses where severe pain might be the aggravating factor for the delirium[5] RECOMMENDATIONS Due to the multifactorial nature of delirium, we are most likely to realise benefit when multiple interventions are instituted. Our meta-analysis supports this approach where peri-operative geriatric consultations have been shown to be a potentially very powerful intervention to decrease delirium. We recommend that future interventional trials for delirium should consider a multi-component approach to preventing delirium. WHAT’S ON THE HORIZON Serum biomarkers generated by the various pathological processes of delirium may be helpful in identifying patients at risk of delirium, diagnosing delrium and assessing the severity of delirium[52-54]. Inflammatory biomarkers interleukin 1,2,6,8, natural killer cell activity and C-reactive protein (CRP) have been implicated in being predictive markers of delirium[52-56]. Zhang et al found that a change in the CRP from admission to ICU was associated with an increased risk of developing delirium[54]. S100 calcium binding protein B (S100 β) which is a protein present in astrocytes and oligodendrocytes, indicates blood brain barrier disruption and has been implicated in the duration of delirium[53]. Fast track surgery has also been associated with a reduction in the incidence of POD. Krenk et al found that in elderly patients, fast track orthopaedic surgery with multimodal opioid-sparing analgesia will decrease the incidence of delirium[57]. So specific identification of biomarkers in patients at risk and multimodal optimisation of perioperative care may be effective in identifying patients at risk and improving the outcome of POD. Page 19 of 24 CONCLUSION Currently research regarding geriatric anaesthesia and postoperative cognitive complications is on the rise. POD is a common complication seen in our geriatric population that has implications on both morbidity and mortality. Early diagnosis and prompt implentation of pharmacological and non-pharmacological interventions to prevent or minimise POD is required to decrease these adverse outcomes. Page 20 of 24 REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. Bekker, A.Y. and E.J. Weeks, Cognitive function after anaesthesia in the elderly. Best Pract Res Clin Anaesthesiol, 2003. 17(2): p. 259-72. Robinson, T.N.R., C. D.; Tran, Z. V.; Brenner, L. A.; Moss, M., Motor subtypes of postoperative delirium in older adults. Archives of Surgery, 2011. 146(3): p. 295-300. Terrando, N., et al., Perioperative cognitive decline in the aging population. Mayo Clin Proc, 2011. 86(9): p. 885-93. Weiser, T.G., et al., An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet, 2008. 372(9633): p. 139-44. A. Rudra, S.C., J. Kirtania, S. Sengupta, G. Moitra, S. Sirohia, R. Wankhade, S. Banerjee, Postoperative delirium. Indian J Crit Care Med Oct-Dec 2006 2006. 10(4): p. 235-240. Wass, S., P.J. Webster, and B.R. Nair, Delirium in the elderly: a review. Oman Med J, 2008. 23(3): p. 150-7. Bilotta, F., et al., Postoperative delirium: risk factors, diagnosis and perioperative care. Minerva Anestesiol, 2013. 79(9): p. 1066-76. Deiner, S. and J.H. Silverstein, Postoperative delirium and cognitive dysfunction. Br J Anaesth, 2009. 103 Suppl 1: p. i41-46. Brooks, P.B., Postoperative delirium in elderly patients. Am J Nurs, 2012. 112(9): p. 38-49; quiz 51, 50. American Psychiatric Association. Diagnostic and statistic manual of mental disorders. revised, DSM-IV-TR. 4th ed. Washington, DC: . 2000. Association, A.P., Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. 5th ed. Washington, DC: American Psychiatric Association. 2013. World Health Organisation. The international classification of diseases, 10th revision: ICD-10. In: Mental and behavioral disorders (F00-F99). Geneva: World Health Organisation. 1992. Flynn Makic, M.B., Preventing delirium in postoperative patients. J Perianesth Nurs, 2013. 28(6): p. 404-8. Rudolph, J.L., et al., Delirium is associated with early postoperative cognitive dysfunction. Anaesthesia, 2008. 63(9): p. 941-7. Robinson, T.N. and B. Eiseman, Postoperative delirium in the elderly: diagnosis and management. Clin Interv Aging, 2008. 3(2): p. 351-5. Strom, C., L.S. Rasmussen, and F.E. Sieber, Should general anaesthesia be avoided in the elderly? Anaesthesia, 2014. 69 Suppl 1: p. 35-44. Parikh, S.S. and F. Chung, Postoperative delirium in the elderly. Anesth Analg, 1995. 80(6): p. 1223-32. Dr David Connor, R., Anaesthesia and C. Dr William English, Intensive Care Medicine, DELIRIUM IN CRITICAL CARE AESTHESIA TUTORIAL OF THE WEEK 232. 18TH JULY 2011. Gregory L. Fricchione, M.D., et al., Postoperative Delirium. Am J Psychiatry 2008. 165(7): p. 803-812. Radtke, F.M., et al., Monitoring depth of anaesthesia in a randomized trial decreases the rate of postoperative delirium but not postoperative cognitive dysfunction. Br J Anaesth, 2013. 110 Suppl 1: p. i98-105. Postoperative Management: general principles, in The Medicine Consult Handbook. 2011. Moyce, Z., R.N. Rodseth, and B.M. Biccard, The efficacy of peri-operative interventions to decrease postoperative delirium in non-cardiac surgery: a systematic review and metaanalysis. Anaesthesia, 2014. Bilotta, F.D., A.; Stazi, E.; Titi, L.; Zeppa, I. O.; Cianchi, A.; Rosa, G.; Paoloni, F. P.; Bergese, S.; Asouhidou, I.; Ioannou, P.; Abramowicz, A. E.; Spinelli, A.; Delphin, E.; Ayrian, E.; Zelman, V.; Lumb, P., Early postoperative cognitive dysfunction and postoperative delirium after anaesthesia with various hypnotics: study protocol for a randomised controlled trial--the PINOCCHIO trial. Trials, 2011. 12: p. 170. Page 21 of 24 24. Patti, R., et al., Risk factors for postoperative delirium after colorectal surgery for carcinoma. Eur J Oncol Nurs, 2011. 15(5): p. 519-23. 25. Moher, D., et al., Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ, 2009. 339: p. b2535. 26. Jadad, A.R., et al., Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials, 1996. 17(1): p. 1-12. 27. Deschodt, M.B., T.; Flamaing, J.; Detroyer, E.; Broos, P.; Haentjens, P.; Boonen, S.; Milisen, K., Preventing delirium in older adults with recent hip fracture through multidisciplinary geriatric consultation. Journal of the American Geriatrics Society, 2012. 60(4): p. 733-9. 28. Lundström, M.O., B.; Stenvall, M.; Karlsson, S.; Nyberg, L.; Englund, U.; Borssén, B.; Svensson, O.; Gustafson, Y. Postoperative delirium in old patients with femoral neck fracture: a randomized intervention study. Aging clinical and experimental research, 2007. 178-86. 29. Marcantonio, E.R.F., J. M.; Wright, R. J.; Resnick, N. M. Reducing delirium after hip fracture: a randomized trial. Journal of the American Geriatrics Society, 2001. 516-22. 30. Chan, M.T.V.C., B.; Gin, T.; Lee, T.; Koo, E. Cognitive dysfunction after anesthesia: a randomized controlled trial. Journal of Neurosurgical Anesthesiology, 2010. 408-9. 31. Jildenstål, P.K.H., J. L.; Rawal, N.; Gupta, A.; Berggren, L. Effect of auditory evoked potential-guided anaesthesia on consumption of anaesthetics and early postoperative cognitive dysfunction: a randomised controlled trial. European journal of anaesthesiology, 2011. 213-9. 32. Sieber, F.E.Z., K. J.; Gottschalk, A.; Blute, M. R.; Lee, H. B.; Rosenberg, P. B.; Mears, S. C. Sedation depth during spinal anesthesia and the development of postoperative delirium in elderly patients undergoing hip fracture repair. Mayo Clinic proceedings. Mayo Clinic, 2010. 18-26. 33. Cai, Y.H., H.; Xue, R.; Liu, P.; Feng, G.; Dong, W.; Yu, B.; Zhao, M. Cognitive function correlations with apolipoprotein E 4 single nucleotide polymorphism in 1000 elderly patients folowing general anesthesia: a randomized controlled study. Neural Regeneration Research, 2009. 316-20. 34. Nishikawa, K.N., M.; Omote, K.; Namiki, A., Recovery characteristics and post-operative delirium after long-duration laparoscope-assisted surgery in elderly patients: propofolbased vs. sevoflurane-based anesthesia. Acta Anaesthesiologica Scandinavica, 2004. 48(2): p. 162-8. 35. Papaioannou, A.F., O.; Michaloudis, D.; Balalis, C.; Askitopoulou, H., The impact of the type of anaesthesia on cognitive status and delirium during the first postoperative days in elderly patients. European Journal of Anaesthesiology, 2005. 22(7): p. 492-9. 36. Slor, C.J.d.J., J. F.; Vreeswijk, R.; Groot, E.; Ploeg, T. V.; van Gool, W. A.; Eikelenboom, P.; Snoeck, M.; Schmand, B.; Kalisvaart, K. J., Anesthesia and postoperative delirium in older adults undergoing hip surgery. Journal of the American Geriatrics Society, 1313. 59(7): p. 1313-9. 37. Berggren, D., et al., Postoperative confusion after anesthesia in elderly patients with femoral neck fractures. Anesth Analg, 1987. 66(6): p. 497-504. 38. Kalisvaart, K.J.d.J., J. F.; Bogaards, M. J.; Vreeswijk, R.; Egberts, T. C.; Burger, B. J.; Eikelenboom, P.; van Gool, W. A., Haloperidol prophylaxis for elderly hip-surgery patients at risk for delirium: a randomized placebo-controlled study. Journal of the American Geriatrics Society, 1658. 53(10): p. 1658-66. 39. Wang, W.L., H. L.; Wang, D. X.; Zhu, X.; Li, S. L.; Yao, G. Q.; Chen, K. S.; Gu, X. E.; Zhu, S. N., Haloperidol prophylaxis decreases delirium incidence in elderly patients after noncardiac surgery: a randomized controlled trial*. Critical Care Medicine, 2012. 40(3): p. 731-9. 40. Kaneko, T.C., J.; Ishikura, T.; Kobayashi, M.; Naka, T.; Kaibara, N. Prophylactic consecutive administration of haloperidol can reduce the occurrence of postoperative delirium in gastrointestinal surgery. Yonago Acta Medica, 1999. 179-184. Page 22 of 24 41. Liptzin, B.L., A.; Garb, J. L.; Fingeroth, R.; Krushell, R., Donepezil in the prevention and treatment of post-surgical delirium. American Journal of Geriatric Psychiatry, 1100. 13(12): p. 1100-6. 42. Marcantonio, E.R.P., K.; Appleton, P.; Davis, R. B., Pilot randomized trial of donepezil hydrochloride for delirium after hip fracture. Journal of the American Geriatrics Society, 2011. 59(2). 43. Sampson, E.L.R., P. R.; Ndhlovu, P. N.; Vallance, A.; Garlick, N.; Watts, J.; Blanchard, M. R.; Bruce, A.; Blizard, R.; Ritchie, C. W., A randomized, double-blind, placebo-controlled trial of donepezil hydrochloride (Aricept) for reducing the incidence of postoperative delirium after elective total hip replacement. International Journal of Geriatric Psychiatry, 2007. 22(4): p. 343-9. 44. Akarsu, T.T., H.; Bolat, C.; Ozkaynak, I., Comparison of pre-emptive pregabalin with placebo and diclofenac combination for postoperative analgesia and cognitive functions after laparoscopic cholecystectomy. Turkiye Klinikleri Journal of Medical Sciences, 2012. 32 (4): p. 963-970. 45. Leung, J.M.S., L. P.; Rico, M.; Petersen, K. L.; Rowbotham, M. C.; Dahl, J. B.; Ames, C.; Chou, D.; Weinstein, P. Pilot clinical trial of gabapentin to decrease postoperative delirium in older patients. Neurology, 2006. 1251-3. 46. Ono, H.T., T.; Kido, Y.; Fujino, Y.; Doki, Y., The usefulness of bright light therapy for patients after oesophagectomy. Intensive & Critical Care Nursing, 2011. 27(3): p. 158-66. 47. Taguchi, T.Y., M.; Kido, Y., Influence of bright light therapy on postoperative patients: a pilot study. Intensive & Critical Care Nursing, 2007. 23(5): p. 289-97. 48. Sieber, F.E.Z., K. J.; Gottschalk, A.; Blute, M. R.; Lee, H. B.; Rosenberg, P. B.; Mears, S. C., Sedation depth during spinal anesthesia and the development of postoperative delirium in elderly patients undergoing hip fracture repair.[Erratum appears in Mayo Clin Proc. 2010 Apr;85(4):400 Note: Dosage error in article text]. Mayo Clinic Proceedings, 2010. 85(1): p. 18-26. 49. Mason, S.E., A. Noel-Storr, and C.W. Ritchie, The impact of general and regional anesthesia on the incidence of post-operative cognitive dysfunction and post-operative delirium: a systematic review with meta-analysis. J Alzheimers Dis, 2010. 22 Suppl 3: p. 67-79. 50. Teslyar, P., et al., Prophylaxis with antipsychotic medication reduces the risk of postoperative delirium in elderly patients: a meta-analysis. Psychosomatics, 2013. 54(2): p. 124-31. 51. Zhang, H., et al., Strategies for prevention of postoperative delirium: a systematic review and meta-analysis of randomized trials. Crit Care, 2013. 17(2): p. R47. 52. Babar A. Khan, M., MS, Mohammed Zawahiri, MD,Noll L. Campbell, PharmD, and M. and Malaz A. Boustani, MPH, Biomarkers for Delirium—A Review. Am Geriatr Soc., 2011. 59(2): p. 256-261. 53. Khan, B.A., et al., S100 calcium binding protein B as a biomarker of delirium duration in the intensive care unit - an exploratory analysis. Int J Gen Med, 2013. 6: p. 855-61. 54. Zhongheng Zhang, M., Lifei Pan, MB, Hongsheng Deng, MM, Hongying Ni, MM, Xiao Xu, MB, Prediction of delirium in critically ill patients with elevated C-reactive protein. Journal of Critical Care, 29 (2014) 88–92. 29(1): p. 88-92. 55. AndreasBaranyi, M.D., M.A., Hans-Bernd Rothenhäusler, M.D., The impact of soluble interleukin-2 receptor as a biomarker of delirium. Psychosomatics, 2014. 55(1): p. 51-60. 56. Kotaro Hatta a, Yasuhiro Kishi b, Takashi Takeuchi c, KenWada d, Toshinari Odawara e, Chie Usui a, and H.N.g. Yutaka Machida f, for the DELIRIA-J Group, The predictive value of a change in natural killer cell activity for delirium. Progress in NeuroPsychopharmacology & Biological Psychiatry, 2014. 48 (01): p. 26-31. 57. Krenk, L.R., L. S.; Hansen, T. B.; Bogo, S.; Soballe, K.; Kehlet, H., Delirium after fast-track hip and knee arthroplasty. British Journal of Anaesthesia, 2012. 108(4): p. 607-11. Page 23 of 24 NOTES Page 24 of 24