Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
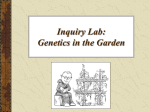
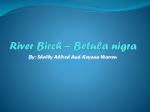
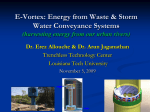
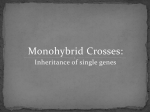
Am J Physiol Regul Integr Comp Physiol 309: R1172–R1177, 2015. First published August 19, 2015; doi:10.1152/ajpregu.00524.2014. Body height and arterial pressure in seated and supine young males during ⫹2 G centrifugation Sine K. Arvedsen,1 Ola Eiken,2 Roger Kölegård,2 Lonnie G. Petersen,1 Peter Norsk,1,3 and Morten Damgaard1,4 1 Department of Biomedical Sciences, Faculty of Health Sciences, University of Copenhagen, Copenhagen, Denmark; Department of Environmental Physiology, Swedish Aerospace Physiology Centre, Royal Institute of Technology, Stockholm, Sweden; and 3Division of Space Life Sciences, Universities Space Research Association and Biomedical Research and Environmental Sciences Division, NASA Johnson Space Center, Houston, Texas; and 4Department of Clinical Physiology and Nuclear Medicine, Centre for Functional Imaging and Research, Hvidovre Hospital, Hvidovre, Denmark 2 Submitted 22 December 2014; accepted in final form 17 August 2015 cardiovascular system; hydrostatic pressure; body height; human centrifuge supine to upright, gravity causes a redistribution of blood from the upper to the lower parts of the body. This induces an abrupt fall in central venous pressure that through the Frank-Starling mechanism decreases cardiac stroke volume (SV) and subsequently arterial pulse pressure (APP). To ensure a sufficient venous return and maintenance of adequate mean arterial pressure (MAP), baroreflexes originating from sensors in the carotid sinuses, aorta, and cardiac chambers induce contraction of the veins and the arterial resistance vessels, as well as an increase in heart rate UPON A CHANGE IN POSTURE FROM Address for reprint requests and other correspondence: S. K. Arvedsen, Dept. of Biomedical Sciences, Faculty of Health Sciences, Univ. of Copenhagen, Blegdamsvej 3b, DK-2200 Copenhagen, Denmark (e-mail: [email protected]). R1172 (HR) and cardiac contractility through the autonomic nervous system (3, 27). Hydrostatic pressure gradients in upright individuals reduce venous return and unload the carotid baroreceptors. It is, therefore, possible that the hydrostatic pressure gradient from the heart to the head in upright subjects is a determinant of arterial pressure at heart level. Tall individuals might, therefore, be endowed with a higher arterial pressure than short individuals through inhibition of the carotid baroreceptors. An animal that illustrates this idea is the giraffe. It has a long vertical distance between the heart and the brain and probably, therefore, possesses the highest arterial pressure of all living species, with MAP at heart level exceeding 200 mmHg (4, 13, 14, 18). In a recent study on humans, we found that 24-h ambulatory arterial pressures in young males increased with body height by 2/2 mmHg [systolic (SAP)/diastolic (DAP) arterial pressure] per 15 cm increase in body height (1). Furthermore, we found that the increases in SV and APP and decrease in HR in response to a moderate antiorthostatic posture change were significantly more pronounced in tall than in short individuals. This indicates that body height affects regulation of arterial pressures. In a human-use centrifuge, it is possible to increase the gravito-inertial (G) stress in the head-to-seat direction (⫹Gz) and, thus, augment intravascular hydrostatic pressure gradients. Arterial pressure at heart level typically increases in response to slightly elevated ⫹Gz-stress in seated humans, probably because of hydrostatic inhibition of the carotid baroreceptors. Hence, we tested the hypothesis that during ⫹2 Gz centrifugation, MAP at heart level increases more in tall than in short males because of the larger hydrostatic pressure difference between heart and head. METHODS Subjects. Nine short (168 –171 cm) and 10 tall (194 –203 cm) males participated in the study (Table 1). All were nonsmokers, had no history of medical diseases, and were healthy, as indicated by a physical examination, a resting arterial pressure below 140/90 mmHg, and values within the normal range for body mass index, blood hemoglobin concentration, and plasma concentrations of glucose, cholesterol, liver enzymes, and creatinine. None of the subjects took any medication. Ethics. Written consent was obtained after the subjects were informed, orally and in writing, about the study protocol and experimental procedures. The protocol was approved by the Regional Human Ethics Committee in Stockholm (no: 2011/2012-31/1) and was in compliance with the Helsinki-II declaration. 0363-6119/15 Copyright © 2015 the American Physiological Society http://www.ajpregu.org Downloaded from http://ajpregu.physiology.org/ by 10.220.33.2 on June 14, 2017 Arvedsen SK, Eiken O, Kölegård R, Petersen LG, Norsk P, Damgaard M. Body height and arterial pressure in seated and supine young males during ⫹2 G centrifugation. Am J Physiol Regul Integr Comp Physiol 309: R1172–R1177, 2015. First published August 19, 2015; doi:10.1152/ajpregu.00524.2014.—It is known that arterial pressure correlates positively with body height in males, and it has been suggested that this is due to the increasing vertical hydrostatic gradient from the heart to the carotid baroreceptors. Therefore, we tested the hypothesis that a higher gravito-inertial stress induced by the use of a human centrifuge would increase mean arterial pressure (MAP) more in tall than in short males in the seated position. In short (162–171 cm; n ⫽ 8) and tall (194 –203 cm; n ⫽ 10) healthy males (18 – 41 yr), brachial arterial pressure, heart rate (HR), and cardiac output were measured during ⫹2G centrifugation, while they were seated upright with the legs kept horizontal (⫹2Gz). In a separate experiment, the same measurements were done with the subjects supine (⫹2Gx). During ⫹2Gz MAP increased in the short (22 ⫾ 2 mmHg, P ⬍ 0.0001) and tall (23 ⫾ 2 mmHg, P ⬍ 0.0001) males, with no significant difference between the groups. HR increased more (P ⬍ 0.05) in the tall than in the short group (14 ⫾ 2 vs. 7 ⫾ 2 bpm). Stroke volume (SV) decreased in the short group (26 ⫾ 4 ml, P ⫽ 0.001) and more so in the tall group (39 ⫾ 5 ml, P ⬍ 0.0001; short vs. tall, P ⫽ 0.047). During ⫹2Gx, systolic arterial pressure increased (P ⬍ 0.001) and SV (P ⫽ 0.012) decreased in the tall group only. In conclusion, during ⫹2Gz, MAP increased in both short and tall males, with no difference between the groups. However, in the tall group, HR increased more during ⫹2Gz, which could be caused by a larger hydrostatic pressure gradient from heart to head, leading to greater inhibition of the carotid baroreceptors. BODY HEIGHT AND ARTERIAL PRESSURE DURING ⫹2 G Table 1. Baseline data for the eighteen subjects participating in the study Height, cm Weight, kg Age, yr BMI, kg/m2 Short (n ⫽ 8) Tall (n ⫽ 10) 167 (162–171) 69 (58–82) 24 (19–29) 23 (19–25) 198* (194–203) 88* (79–104) 23 (18–41) 25* (22–29) The values are means (range). BMI, body mass index. *Statistically significant difference (P ⬍ 0.05) between the groups by unpaired t-test. Fig. 1. Schematic depiction of the ⫹Gz level along the upper body of a tall subject (upper body 1.00 m) seated in the gondola. The gravito-inertial load was ⫹2 Gz at the pivot point, roughly corresponding to the vertical level of the heart. In the supine position, the G load was adjusted so that ⫹2 Gx level corresponded with vertical level of the heart. Prior to the experiment, the rebreathing maneuver for measurement of cardiac output (CO) was rehearsed thoroughly inside the gondola in both the seated and supine position. Each experiment was performed, with the subject once in the seated and once in the supine position in a randomized balanced order. In the seated position, the legs were kept horizontal. The reason for this was twofold 1) our group has previously used this position extensively and documented that the changes in cardiovascular variables are pronounced and reproducible (19 –22); 2) the local reflexes in the legs (myogenic and/or veno-arteriolar reflex responses, etc.) are not, or to a negligible extent, activated when the lower legs are kept horizontal. In this way, the baroreflex responses (arterial and/or cardiopulmonary) are the dominating causes for the observed changes in central hemodynamic changes (15, 28). In the gondola, the subjects were restrained by a five-point safety belt. At 1 G (without rotation), baseline measurements were collected including CO, brachial arterial pressure, and HR at 8 and 2 min before initiation of centrifugation. Subsequently, the G load was increased by 0.5 G/s to ⫹2 G and maintained at this plateau for 10 min, during which time, measurements of CO, arterial pressure, and HR were recorded after 3 (⫹2 G3min) and 8 min (⫹2 G8min), respectively. After changing posture, the subject rested for ⬃10 min, and the experiment was repeated. Each subject was instructed to keep his head still during acceleration and deceleration to avoid motion sickness. Cardiac output. CO was determined by a foreign gas rebreathing technique, whereby a gas mixture consisting of 0.5% sulfur hexafluoride (SF6), 0.1% nitrous oxide (N2O), and 28% oxygen (O2) in nitrogen (N2) was inhaled from and exhaled to a rubber bag over ⬃15 s at a rate of 20 min⫺1, while the nose was occluded with a clip. The volume of rebreathing gas was determined as 30% of the subject’s vital lung capacity (2) (Table 1). During rebreathing, gas was continuously sampled at the mouthpiece for estimations of end-expiratory concentrations of N2O (blood-soluble) and SF6 (blood-insoluble) with an infrared photoacustic gas analyzer (Innocor, Innovision A/S, Odense, Denmark). From the disappearance rate of N2O, pulmonary blood flow and, thus, CO were calculated (7, 12). SF6 was used to correct for inadequate mixing of air in the lungs with the gas mixture from the bag and for changes in the distribution space of N2O. The equipment was fastened perpendicular to the wall of the gondola and operated by the subjects. The mouthpiece was suspended from the gondola wall by a string so that the subjects only needed to maneuver the mouthpiece. The string length and, thereby, the position of the mouthpiece was adjusted for each subject both in the seated and supine position. Anthropometric measures. Body height was determined with a Leicester height-measuring scale. To estimate arterial pressure at the level of the carotid sinus and at the level of the aortic valves, we used anthropometric data obtained in a recent publication (1) from 75 subjects with a body height varying from 147 to 206 cm. In these subjects, the distance from the carotid sinus to the aortic valves (CS-AV) was determined using an ultrasound technique (1). By simple measurements using a ruler on the subject in a seated position, we, furthermore, determined the distance from the carotid sinus to the top of the head (CS-TH) and the distance from the middle of the brachial arterial pressure cuff to the top of the head. From these values, the distance MidCuff-CS was calculated as the difference of MidCuff-TH ⫺ CS-TH, whereas the distance MidCuff-AV was calculated as MidCuff-CS ⫺ CS-AV. Thereafter, by simple linear regression, we expressed the correlations MidCuff-CS ⫽ 4.9 ⫹ 0.16 ⫻ body height and MidCuff-AV ⫽ 1.2 ⫹ 0.07 ⫻ body height. These equations were used in the present investigation to calculate the distances MidCuff-CS and MidCuff-AV of the subjects and, thereby, estimate the pressure at the level of the aortic valves and the carotid sinus. Heart rate. HR was measured from a precordial ECG lead (AS2, Datex-Engström, Helsinki, Finland). AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00524.2014 • www.ajpregu.org Downloaded from http://ajpregu.physiology.org/ by 10.220.33.2 on June 14, 2017 Equipment and measurements. The experiments were conducted in the human-use centrifuge (ASEA, Stockholm, Sweden) at the Royal Institute of Technology, Stockholm, Sweden. The rotational radius to the center of the centrifuge gondola is 7.25 m. The gondola was tangentially pivoted, so that the gondola floor remained perpendicular to the G-vector at all times. Each subject was tested in seated and supine positions. In the seated position, they leaned against a vertical backrest and kept their legs horizontal, so that the G vector was aligned with the upper body (⫹Gz), whereas in the supine position, the G vector was directed front-to-back (⫹Gx). The gravitational gradient of a seated person in a long-armed centrifuge is very small (Fig. 1). The difference in ⫹Gz at the carotid sinus level between a short and a tall male is, therefore, negligible. In the supine position, the gradient is near zero. Multiple slip rings at the center of rotation allowed for audiovisual monitoring, power supply, and transmission of physiological signals between the gondola and the control room. An electrocardiogram (ECG) was recorded from a precordial lead using a monitoring system (type AS2; Datex, Helsinki, Finland). The G force was determined using an accelerometer positioned at heart level, both when the subject was in the seated and the supine position. Continuous signals were recorded at 20 Hz per channel in a digital data acquisition system (Biopac, Goleta, CA). The operator monitored and instructed the subject continuously via voice communication and video camera. Protocol. All subjects were instructed not to eat for at least 2 h before the experiment, so that they were neither hungry nor full during the experiment. They were, furthermore, instructed to avoid nicotine and caffeine during the 4 h prior to the experiment. R1173 R1174 BODY HEIGHT AND ARTERIAL PRESSURE DURING ⫹2 G RESULTS Ten tall and nine short subjects completed the experiment (Table 1). One short subject was excluded after the experiment, as he reported afterward that he had felt motion sick during the session. Seated. In response to ⫹2 Gz, MAP increased in both short (22 ⫾ 2 mmHg, P ⬍ 0.0001) and tall (23 ⫾ 2 mmHg, P ⬍ 0.0001) individuals (Fig. 2A) with no significant difference between the groups. HR increased in both the short (P ⫽ 0.012) and the tall group (P ⬍ 0.0001, Fig. 2B), with a significant interaction (height·G level), indicating (P ⫽ 0.020) that the increase from ⫹1 Gz to ⫹2 Gz3min was greatest in the tall group (tall: 14 ⫾ 2 vs. short: 7 ⫾ 2 bpm, P ⫽ 0.015). SV (Fig. 2C) decreased in the short group (26 ⫾ 4 ml, P ⫽ 0.001) yet more so in the tall group (39 ⫾ 5 ml, P ⬍ 0.0001; short vs. tall: P ⫽ 0.047) when exposed to ⫹2 Gz. Also CO decreased in both the short (P ⫽ 0.015) and tall group (P ⫽ 0.001) (Table 2). TPR increased in both groups (P ⬍ 0.001, Table 2). APP did not change significantly during centrifugation in either group (short, P ⫽ 0.231; tall, P ⫽ 0.080). Although the test for interaction indicated that the two groups responded differently (P ⫽ 0.027) to the ⫹G exposure, the change from ⫹1 Gz to ⫹2 Gz3min (3 ⫾ 4 vs. ⫺5 ⫾ 2 mmHg, P ⫽ 0.125) and ⫹2 G3min to ⫹2 G8min (1 ⫾ 5 vs. ⫺2 ⫾ 2 mmHg, P ⫽ 0.473) was not significantly different in the two groups (Table 2). Supine. In response to ⫹2 Gx, MAP and SAP increased in the tall group only (P ⫽ 0.005, Fig. 2A and P ⬍ 0.001, Table 2, respectively). HR increased significantly in the short (P ⫽ 0.009) and tall (P ⫽ 0.049, Fig. 2B) group. SV decreased (P ⫽ 0.012, Fig. 2C) in the tall group only. TPR increased in both the short (P ⫽ 0.006) and tall group (P ⬍ 0.001, Table 2). Fig. 2. A: mean arterial pressure (MAP) before the onset of centrifugation (⫹1 G), after 3 min (⫹2 G3min), and after 8 min of centrifugation at ⫹2 G (⫹2 G8min). Short group n ⫽ 8 except at ⫹2 Gz8min and at ⫹2 Gx3min (n ⫽ 7). Tall group n ⫽ 10, except at ⫹2 Gx8min (n ⫽ 9). Œ denotes short group in seated position, while denotes short group in supine position. ⌬ denotes tall group in seated position, while ⵜ denotes tall group in supine position. B: heart rate (HR) before the onset of centrifugation (⫹1 G), after 3 min, (⫹2 G3min), and after 8 min of centrifugation at ⫹2 G (⫹2 G8min). Short group: n ⫽ 8. Tall group: n ⫽ 10. C: stroke volume (SV) before the onset of centrifugation (⫹1 G), after 3 (⫹2 G3min), and after 8 min of centrifugation at ⫹2 G (⫹2 G8min). Short group: n ⫽ 8. Tall group: n ⫽ 10, except at ⫹2 Gz8min and at ⫹2 Gx8min (n ⫽ 9). Values are expressed as means ⫾ SE. *Statistically significant (P ⬍ 0.05) difference from ⫹1 G determined by a post hoc multiple-range test (Scheffé). #Statistically significant difference between the short and tall group in the change from ⫹1 Gz to ⫹2 Gz3min by an unpaired t-test. DISCUSSION The present results show that during ⫹2 Gz centrifugation, MAP at the heart level increases in seated males with no significant difference between short and tall individuals. However, during the initial 3 min of ⫹2 Gz, HR increases significantly more in the tall than in the short group (⫹2 Gz3min), indicating an augmented baroreflex-controlled HR response in the tall subjects. Presumably, the greater G-induced HR response in the tall subjects is attributable to a combination of a larger inhibition of the 1) cardiopulmonary baroreflexes caused by a more pronounced decrease in cardiac preload, and 2) AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00524.2014 • www.ajpregu.org Downloaded from http://ajpregu.physiology.org/ by 10.220.33.2 on June 14, 2017 Arterial pressure. Brachial arterial pressure (SAP, MAP, DAP) was measured in the upper right arm with an oscillometric equipment (Omron M4-I). During all measurements, care was taken to ensure that the midpoint of the arm cuff was located at mid-heart level. Data analysis. Offline data analysis was performed with an Acknowledge 3.90 BioPac digital data handling system (BioPac, Goleta, CA). HR (ECG) was registered over a period of 30 s before each rebreathing maneuver. HR used for calculation of SV was read and manually recorded from the ECG output during the rebreathing maneuver. SV was calculated by dividing CO by HR, and total peripheral resistance (TPR) by dividing MAP by CO. Statistical analyses. For each subject, cardiovascular variables were averaged during the two baseline measurements in each posture. A mixed-model ANOVA for repeated measures with height (tall and short) as between-subject factor and G-level as within subject factor in both the seated position (⫹1 Gz, ⫹2 Gz3min, and ⫹2 Gz8min) and supine position (⫹1 Gx, ⫹2 Gx3min, and ⫹2 Gx8min) was used to test for intragroup changes over time. Differences between mean values at ⫹1 Gx and ⫹2 Gx3min and ⫹2 Gx8min were evaluated by a post hoc multiple-range test (Scheffé). If a different response to changes in G level between the short and tall group was indicated as a significant interaction (height·G level), an unpaired t-test was used to evaluate whether these differences (⫹1 Gz to ⫹2 Gz3min and ⫹2 Gz3min to ⫹2 Gz8min) were significantly different. Baseline data (Table 1) are presented as means and range, whereas all other data are presented as means ⫾ SE. In all tests, P ⬍ 0.05 was chosen as the level of significance. The statistical analyses were performed using SPSS for Windows (IBM SPSS Statistics 19). BODY HEIGHT AND ARTERIAL PRESSURE DURING ⫹2 G R1175 Table 2. Cardiovascular parameters for the short and tall group in the seated position at ⫹1 Gz, ⫹2 Gz3min, and ⫹2 Gz8min and in the supine position at ⫹1 Gx, ⫹Gx3min, and ⫹2 Gx8min ⫹1 G Seated SAP, mmHg DAP, mmHg APP, mmHg CO, l/min TPR, mmHg·min⫺1·l DAP, mmHg APP, mmHg CO, l/min TPR, mmHg·min⫺1·l ⫹2 G8min Short Tall Short Tall Short Tall Short Tall Short Tall 125 ⫾ 3 134 ⫾ 4 80 ⫾ 2 76 ⫾ 3 45 ⫾ 3 58 ⫾ 4 6.4 ⫾ 0.4 7.9 ⫾ 0.2 15.3 ⫾ 0.9 12.2 ⫾ 0.3 144 ⫾ 4 152 ⫾ 6* 97 ⫾ 5* 98 ⫾ 4* 48 ⫾ 5 54 ⫾ 4 5.6 ⫾ 0.3 6.9 ⫾ 0.2* 20.6 ⫾ 1.3* 17.1 ⫾ 0.6* 150 ⫾ 4* (n ⫽ 7) 153 ⫾ 4* 101 ⫾ 2* (n ⫽ 7) 101 ⫾ 4* 49 ⫾ 4 (n ⫽ 7) 52 ⫾ 3 5.2 ⫾ 0.2 6.1 ⫾ 0.3* (n ⫽ 9) 22.4 ⫾ 0.7* (n ⫽ 7) 19.7 ⫾ 0.8*¤ (n ⫽ 9) Short Tall Short Tall Short Tall Short Tall Short Tall 123 ⫾ 5 133 ⫾ 4 71 ⫾ 4 66 ⫾ 3 52 ⫾ 4 67 ⫾ 5 6.5 ⫾ 0.4 9.0 ⫾ 0.6 13.7 ⫾ 0.5 10.1 ⫾ 0.5 128 ⫾ 3 (n ⫽ 7) 143 ⫾ 4* 77 ⫾ 2 (n ⫽ 7) 71 ⫾ 3 51 ⫾ 4 (n ⫽ 7) 72 ⫾ 3 6.2 ⫾ 0.4 8.3 ⫾ 0.5 15.2 ⫾ 0.8 (n ⫽ 7) 11.8 ⫾ 0.6 128 ⫾ 3 142 ⫾ 4* (n ⫽ 9) 75 ⫾ 2 69 ⫾ 2 (n ⫽ 9) 52 ⫾ 3 73 ⫾ 4 (n ⫽ 9) 6.0 ⫾ 0.3 7.7 ⫾ 0.3 (n ⫽ 9) 15.8 ⫾ 0.7 12.5 ⫾ 0.5* (n ⫽ 9) Data are presented as means ⫾ SE for the tall group (n ⫽ 10) and the short group (n ⫽ 8). SAP, systolic arterial pressure; DAP, diastolic arterial pressure; APP, arterial pulse pressure; CO, cardiac output; TPR, total peripheral resistance. Statistically significant (P ⬍ 0.05) difference from ⫹1 G. ¤Statistically significant (P ⬍ 0.05) difference from ⫹2 G3min determined by a post hoc multiple-range-test (Scheffé). carotid baroreflexes because of the larger hydrostatic pressure gradients. This is, however, speculative but could be an explanation for our findings. Seated Centrifugation ⫹Gz-induced MAP increase. The mechanisms for the increase of some 20 mmHg in MAP in both groups of males merit comments. First, this magnitude of increase shows that arterial pressure regulation is sensitive to hydrostatic pressure gradients in the cardiovascular system. Second, the increase in the arterial pressure (Fig. 2A and Table 2) must primarily have been accomplished by systemic peripheral vasoconstriction, because CO was unchanged or fell in both groups during centrifugation. Third, the decrease in SV elicited a reflex increase in HR to protect CO from decreasing; nevertheless, CO decreased during ⫹2 Gz. Fourth, despite the unchanged APP, which reflects an unchanged pulsation in the arterial tree, MAP increased by some 20 mmHg at the midbrachial level in both groups. This indicates that the baroreflexes involved in the increase of TPR and HR, must predominantly be 1) the carotid caused by the decrease in MAP at this hydrostatic level, and 2) the cardiopulmonary caused by the decrease in preload indicated by the decrease in SV. We assume that the baroreceptors in the aorta were not or only modestly affected by ⫹2 Gz, because the mean body height of the short (167 ⫾ 1 cm) and tall group (198 ⫾ 1 cm) correspond to an estimated difference in MAP between midbrachial (cuff) to the level of the aortic valves of 19 and 22 mmHg, respectively. This is very similar to the increase in midbrachial MAP during the ⫹2 Gz that we observed. Thus, with very small changes in APP and MAP, the aortic baroreceptors were probably not inhibited, rendering them less important in initiating systemic arterial vasoconstriction and tachycardia. The increase in HR and TPR were, therefore, most likely initiated primarily by the carotid and/or cardiopulmonary reflexes. HR response. HR increased more and faster in the tall vs. the short subjects during ⫹2 Gz stress (Fig. 2B). The mechanism for this may be a more pronounced inhibition of the carotid baroreflexes caused by the hydrostatically lower arterial pressure in the carotid sinus in the tall subjects. This is in accordance with our previous observation that the HR response during moderate ⫹1 G upper body posture change is more pronounced in the tall compared with short individuals (1). In previous studies from our laboratory, we have demonstrated that sudden pressure changes in the carotid sinus (8 –10) within seconds initiate reflex changes in HR by modulating the vagal input to the heart. Systemic arterial vasoconstriction. During ⫹2 Gz, MAP increased within the same magnitude in the two groups, indicating a minor importance of the hydrostatic gradient from the heart level to the baroreceptors in the regulation of MAP. In contrast, the results confirm our previous suggestion, that the higher ambulatory MAP in tall males is not caused by hydrostatics and carotid baroreflexes, but rather by a larger SV and thus CO (1). Even though the hydrostatic pressure changes must have been augmented in the tall compared with the short subjects, this was apparently not enough to induce a greater systemic arteriolar constriction. From previous data (1), it can be estimated that the difference in body height between the tall and short group corresponds to a 5-cm difference in MidCuffCS. Because we observed the same MAP at heart level in the two groups during centrifugation (Fig. 2A), the arterial pressure in the carotid sinus must have been about 7 mmHg lower at ⫹2 Gz (2 ⫻ 5 cm because of the ⫹2 Gz) in the tall subjects. Apparently, this drop in carotid sinus pressure in the tall subjects did not induce an increase in the systemic arterial AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00524.2014 • www.ajpregu.org Downloaded from http://ajpregu.physiology.org/ by 10.220.33.2 on June 14, 2017 Supine SAP, mmHg ⫹2 G3min BODY HEIGHT AND ARTERIAL PRESSURE DURING ⫹2 G R1176 Despite the abolishment of the hydrostatic pressure gradient, the hemodynamic response differed between short and tall subjects when exposed to ⫹2 Gx. In future studies, sizedependent differences in the compression of the thorax in response to ⫹Gx exposure should be evaluated by esophageal or central venous pressure and/or by estimation of left ventricular diameter. Conclusion. The hypothesis that MAP at midbrachial heart level would increase more in the tall than in the short males was not confirmed. However, HR increased faster in tall than short males during ⫹2 Gz centrifugation, which might be attributed to the greater hydrostatic heart to brain distance and, hence, lower MAP in the carotid sinus. Our findings indicate that body height is a factor for the increase in HR to protect CO from falling due to a decrease in cardiac preload during orthostatic challenges. Peripheral arteriolar constriction seems relatively independent of body height as the increase in TPR was not different between the short and tall group. The differences in arterial pressure and SV between short and tall during the ⫹2 Gx load may reflect a more pronounced compression of the thorax in the front to back direction in the tall males. This needs to be further investigated. Perspectives and Significance REFERENCES The present findings suggest that acute baroreflex setting of systemic vascular resistance is probably independent of body height, whereas the setting of HR is not. It would be of interest to investigate the combined effect of age and body height on HR and arterial pressure regulation to understand the implications of gravity for the development of hypertension and other negative impacts on health. During ⫹2 Gz, MAP (at heart level) increased to approximately similar levels in tall and short males. As the hydrostatic gradient from the heart to the head was greater, MAP was considerably lower at the carotid sinus level in tall individuals. Hence, it is conceivable that the cerebral perfusion pressure could be lower in the tall subjects. Notably, although the cerebral vasculature regulates flow across a wide range of perfusion pressures, the autoregulatory capacity is exceeded once local arterial pressure drops below 60 –70 mmHg (30). It has been shown that the capacity to withstand increasing ⫹Gz load (G level tolerance) is negatively correlated to body height and, in particular, to the distance between the heart and the eye (17). Therefore, it would be interesting to investigate whether the blood flow to the brain is different in tall vs. short males during high-level and/or long-duration ⫹Gz loads, and whether the autoregulatory capacity is related to body height. GRANTS The study was funded by the European Space Agency, ESA (grant/contract no. ESA-CORA-GBF-2010-300). DISCLOSURES No conflicts of interest, financial or otherwise, are declared by the authors. AUTHOR CONTRIBUTIONS Author contributions: S.K.A., O.E., R.K., L.G.P., P.N., and M.D. conception and design of research; S.K.A., O.E., and R.K. performed experiments; S.K.A. analyzed data; S.K.A., P.N., and M.D. interpreted results of experiments; S.K.A. prepared figures; S.K.A. drafted manuscript; S.K.A., O.E., R.K., L.G.P., P.N., and M.D. edited and revised manuscript; S.K.A., O.E., R.K., L.G.P., P.N., and M.D. approved final version of manuscript. 1. Arvedsen SK, Damgaard M, Norsk P. Body height and blood pressure regulation in humans during anti-orthostatic tilting. Am J Physiol Regul Integr Comp Physiol 302: R984 –R989, 2012. 2. Berglund E, Birath G, Bjure J, Grimby G, Kjellmer I, Sandqvist L, Söderholm B. Spirometric studies in normal subjects. I. forced expirograms in subjects between 7 and 70 years of age. Acta Med Scand 173: 185–192, 1963. 3. Blomqvist GC, Stone HL. Cardiovascular adjustments to gravitational stress. In: Handbook of Physiology. The Cardiovascular System. Peripheral Circulation and Organ Blood Flow. Bethesda, MD: Am. Physiol. Soc, 1983, sect. 2, vol. III, pt. 2, chapt. 28, p. 1025–1062. 4. Brøndum E, Hasenkam JM, Secher NH, Bertelsen MF, Grøndahl C, Petersen KK, Buhl R, Aalkjaer C, Baandrup U, Nygaard H, Smerup M, Stegmann F, Sloth E, Ostergaard KH, Nissen P, Runge M, Pitsillides K, Wang T. Jugular venous pooling during lowering of the head affects blood pressure of the anesthetized giraffe. Am J Physiol Regul Integr Comp Physiol 297: R1058 –R1065, 2009. 5. Convertino VA, Previc FH, Ludwig DA, Engelken EJ. Effects of vestibular and oculomotor stimulation on responsiveness of the carotidcardiac baroreflex. Am J Physiol Regul Integr Comp Physiol 273: R615– R622, 1997. 6. Convertino VA. Interaction of semicircular canal stimulation with carotid baroreceptor reflex control of heart rate. J Vestib Res 8: 43–49, 1998. 7. Damgaard M, Norsk P. Effects of ventilation on cardiac output determined by inert gas rebreathing. Clin Physiol Funct Imaging 25: 142–147, 2005. 8. Eckberg DL. Temporal response patterns of the human sinus node to brief carotid baroreceptor stimuli. J Physiol 258: 769 –782, 1976. AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00524.2014 • www.ajpregu.org Downloaded from http://ajpregu.physiology.org/ by 10.220.33.2 on June 14, 2017 constrictor response of sufficient magnitude to substantially affect the arterial pressure response. Supine centrifugation. It is well known that cardiovascular function is affected by increased ⫹Gx load (23, 25). In the present study, the tall group exhibited greater response to ⫹2 Gx despite the fact that longitudinally oriented vessels should be unaffected by this stimulus. We observed an increased SAP (Table 2) and a decreased SV (Fig. 2C) in the tall group only. The mechanism underlying this intergroup difference remains to be settled, but conceivably, a greater compression of the thorax in the front to back (⫹Gx) direction in the tall group may have contributed. Increased intrathoracic pressure decreases transmural pressure in the vena cava, which diminishes cardiac preload (26, 31). A thoracic compression also affects the heart and vessels around the heart, including the aorta, which may increase afterload and, hence, reduce SV and CO. These effects might be greater in the tall subjects, as they probably have a larger depth of their thorax. Limitations. It is possible that vestibular stimulation during centrifugation affected cardiovascular regulation (5, 6, 11, 16, 24, 29). Usually, vestibular stimulation induces nausea and increases vagal tone, which attenuates the increase in MAP during increased G stress. It is unlikely, however, that the vestibular stimulation would be different in short and tall individuals. Although all subjects were familiarized with the procedure from test trials, it could be argued that the increasing HR during centrifugation was caused by mental stress. However, it is unlikely that stress should increase HR more in the tall than in the short group during ⫹2 Gz. We measured arterial pressure by an oscillometric method, which prevented us from detecting temporal differences in MAP between the two groups, in particular, within the initial minutes. It is, however, evident that MAP stabilizes at the same level at the 3rd and 8th min of ⫹2 Gz exposure in both groups. BODY HEIGHT AND ARTERIAL PRESSURE DURING ⫹2 G 20. Pump B, Gabrielsen A, Christensen NJ, Bie P, Bestle M, Norsk P. Mechanisms of inhibition of vasopressin release during moderate antiorthostatic posture change in humans. Am J Physiol Regul Integr Comp Physiol 277: R229 –R235, 1999. 21. Pump B, Kamo T, Gabrielsen A, Bie P, Christensen NJ, Norsk P. Central volume expansion is pivotal for sustained decrease in heart rate during seated to supine posture change. Am J Physiol Heart Circ Physiol 281: H1274 –H1279, 2001. 22. Pump B, Schou M, Gabrielsen A, Norsk P. Contribution of the leg vasculature to hypotensive effects of an antiorthostatic posture change in humans. J Physiol 519: 623–628, 1999. 23. Pump B, Videbaek R, Gabrielsen A, Norsk P. Arterial pressure in humans during weightlessness induced by parabolic flights. J Appl Physiol 87: 928 –932, 1999. 24. Ray CA, Hume KM. Neck afferents and muscle sympathetic activity in humans: implications for the vestibulosympathetic reflex. J Appl Physiol 84: 450 –453, 1998. 25. Rohdin M, Petersson J, Mure M, Glenny RW, Lindahl SGE, Linnarsson D. Protective effect of prone posture against hypergravityinduced arterial hypoxaemia in humans. J Physiol 548: 585–591, 2003. 26. Rohdin M, Petersson J, Sundblad P, Mure M, Glenny RW, Lindahl SGE, Linnarsson D. Effects gravity on lung diffusing capacity and cardiac output in prone and supine humans. J Appl Physiol 95: 3–10, 2003. 27. Rowell LB. Human Cardiovascular Control. New York: Oxford University Press, 1993. 28. Sejrsen P, Henriksen O, Paaske WP. Effect of orthostatic blood pressure changes upon capillary filtration-absorption rate in the human calf. Acta Physiol Scand 111: 287–291, 1981. 29. Tanaka K, Abe C, Awazu C, Morita H. Vestibular system plays a significant role in arterial pressure control during head-up tilt in young subjects. Auton Neurosci 148: 90 –96, 2009. 30. Testart J. [Physiopathology of the cerebral arterial circulation. Application to cerebro arterial surgery]. J Mal Vasc 15: 194 –201, 1990. 31. Videbaek R, Norsk P. Atrial distension in humans during microgravity induced by parabolic flights. J Appl Physiol 83: 1862–6, 1997. AJP-Regul Integr Comp Physiol • doi:10.1152/ajpregu.00524.2014 • www.ajpregu.org Downloaded from http://ajpregu.physiology.org/ by 10.220.33.2 on June 14, 2017 9. Eckberg DL. Baroreflex inhibition of the human sinus node: importance of stimulus intensity, duration, and rate of pressure change. J Physiol 269: 561–577, 1977. 10. Eckberg DL. Adaptation of the human carotid baroreceptor-cardiac reflex. J Physiol 269: 579 –589, 1977. 11. Eiken O, Tipton MJ, Kölegard R, Lindborg B, Mekjavic IB. Motion sickness decreases arterial pressure and therefore acceleration tolerance. Aviat Space Environ Med 76: 541–546, 2005. 12. Gabrielsen A, Videbaek R, Schou M, Damgaard M, Kastrup J, Norsk P. Non-invasive measurement of cardiac output in heart failure patients using a new foreign gas rebreathing technique. Clin Sci (Lond) 102: 247–252, 2002. 13. Goetz RH, Warren JV, Gauer OH, Patterson JL, Doyle JT, Keen EN, McGregor M, Tiller LM, Smith M, Mance E. Circulation of the giraffe. Circ Res 8: 1049 –1058, 1960. 14. Hargens AR, Millard RW, Pettersson K, Johansen K. Gravitational haemodynamics and oedema prevention in the giraffe. Nature 329: 59 –60, 1987. 15. Henriksen O, Sejrsen P. Local reflex in microcirculation in human cutaneous tissue. Acta Physiol Scand 98: 227–231, 1976. 16. Iwata C, Abe C, Tanaka K, Morita H. Role of the vestibular system in the arterial pressure response to parabolic-flight-induced gravitational changes in human subjects. Neurosci Lett 495: 121–125, 2011. 17. Klein KE, Brüner H, Jovy D, Vogt L, Wegmann HM. Influence of stature and physical fitness on tilt-table and acceleration tolerance. Aerospace Med 40: 293–297, 1969. 18. Patterson JL, Goetz RH, Doyle JT, Warren JV, Gauer OH, Detweiler DK, Said SI, Hoernicke H, McGregor M, Keen EN, Smith MH, Hardie EL, Reynolds M, Flatt WP, Waldo DR. Cardiorespiratory dynamics in the ox and giraffe, with comparative observations on man and other mammals. Ann NY Acad Sci 127: 393–413, 1965. 19. Pump B, Christensen NJ, Videbaek R, Warberg J, Henriksen O, Norsk P. Left atrial distension and antiorthostatic decrease in arterial pressure and heart rate in humans. Am J Physiol Heart Circ Physiol 273: H2632–H2638, 1997. R1177