Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
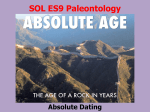
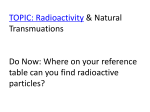
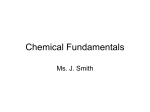
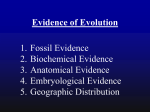
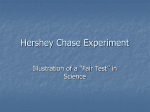
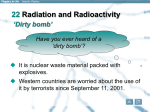
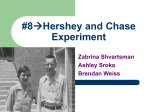
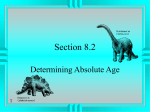
Radioactive Isotopes and Nuclear Radiations in the Treatment of Cancer* JOHN H. LAWRENCE AND CORNELIUS (Donner Laboratory and Donner Pavilion, It is now @20 years since we began to use arti ficially produced radioactive isotopes in cancer re search and in medical research. Actually, our first therapeutic trials were in 1936. In the early days the hope was that at the end of @0 years one could report outstanding examples of selective localiza tion of radioactive compounds in neoplastic tissue, making it possible to give the tumor tissue many times more irradiation than the surrounding, nor mal tissues. Up to the present moment, investigations with only two radioactive isotopes have given us impor tant therapeutic applications in hyperplastic and neoplastic diseases through selective localization. These are radiophosphorus in the treatment of polycythemia vera and radioiodine in the treat ment of the thyroid hyperplasia of Grave's disease and in the palliative treatment of certain thyroid cancers. However, one who has worked in the field from the beginning and who is asked to sum up his experiences can't help saying that the therapeutic achievements have been disappointing; but even in the early days we believed that the greatest contribution of radioactive isotopes in the field of medical and cancer research would lie in tracer applications, and we have devoted most of our energies to the latter. Even though the achievements in prolongation of life and cures in cancer have not been great so far, one should not dismiss too lightly the con tributions of artificial radioactivity and nuclear radiations in cancer therapy. The clinician should not underestimate the importance of relief from pain and extension of comfortable life, and here their value is well established. The importance of the products of nuclear phys ics in cancer therapy is pointed up by the fact that demands for radioactive isotopes in medical and biological research have risen rapidly in the past 10 years. The shipments of radioactive isotopes from Oak Ridge National Laboratory have risen from less than 500 in 1946 to almost 1@,000 in 1954. Seventy per cent of the total dollar value of all * Presented topes and of Cancer presented appeared as part of the Symposium on Radioactive Iso Cancer at the meeting of the American Association Research in San Francisco, April 16, 1955. Papers by David M. Greenberg and by Jacob Furth have in the August, 1955, and the January, 1956, issues of Cancer Research, respectively. University A. T0BIAs of California, Berkeley, Calif.) shipments is for medical use, and one-third of these shipments are for cancer therapy. For in stance, there are 50 medical groups in the United States using radioactive colloidal gold and radio active colloidal chromic phosphate for interstitial infiltration in various types of cancer, such as prostatic, uterine, and bronchogenic. Two hundred fifty groups are using radioactive gold, chromic phosphate, and yttrium colloids in the treatment of cancer metastasized to the pleural and perito neal cavities. There are 400 groups using iodine 181 in the diagnosis and treatment of hyperplastic and neoplastic thyroid disease and 889 groups using @32 for the treatment of polycythemia vera and chronic leukemia. During 1954 there were over 5,000 shipments of radioactive iodine from Oak Ridge to individual users, over @,500ship Inents of radioactive phosphorus, and 6@ ship ments of radioactive gold. At the present time there are 30 cobalt teletherapy units in the United States in use for external irradiation therapy of cancer with high energy gamma rays, and 50 more are being planned (1).' Most of the isotopes which have been used in the therapy of hyperplastic or neoplastic diseases in the form of internal, intracavitary, interstitial, contact, tele, or fission radiation are listed in Chart 1 in the order of increasing atomic number. Early work by Kruger in this laboratory 15 years ago (@5) and by Zahl at al. (59), followed by the uranium fission experiments by Tobias at al. (55), more recently has led to the trial of boron-lO in the treatment of brain tumors, particularly glio blastomas, the radiation being derived from the fission of the boron nuclei after slow neutron cap ture (7). Kruger bathed tumor slices in boric acid solution in vitro and then irradiated them with slow neutrons, causing fission of the boron nuclei into lithium and alpha particles. The ionization ob tained is relatively densely localized, the particles traveling about one cell diameter (55). After borax containing boron-lO was injected intravenously into patients with brain tumors who were then ex posed to soft neutrons from the atomic pile, Farr, Sweet at al. (7, 13) have been able to deliver a few ‘Atthe International Conference @nthe Peaceful Uses of Atomic Energy held in Geneva in August, 1955, the author learned from Professors Modestov and Fateyeva that there are 150 such units now in operation in the Soviet Union. 185 Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. Cancer Research 186 hundred roentgens to the tumor tissue by such fis sion energy, but this is probably insufficient to give real therapeutic effect. Pathological studies of eight of the first ten patients treated at Brookhaven showed changes suggestive of irradiation effects in three patients; however, large areas of viable tu mor were found in all cases (13). More recent in vestigations by Kruger have shown that the con centration of boron in the boundary between nor mal and tumor tissue in glioblastoma multiforme tumors in mice can be increased by injection of palliative treatment of advanced cancer of the bladder, but the survival time is not available for a large series of patients (58). The beta- and gam ma-emitting isotope Na24 has also been tried in the treatment of chronic leukemia, but the method has not found wide usage, since there is no selective localization of sodium. The first example of a successful application of a radioactive isotope in therapy was the treatment of polycythemia vera with @32• Enough experience has been gained over the past @20 years to allow one SOME OF THE THERAPEUTIC USES OF RADIOACTIVE ISOTOPES Glioblastoma multiforme Bladder carcinoma Polycythemia, chronic leukemias, breast cancer Control of oscites and pleural effusion in metastatic Deritoneal and aleural carcinoma .@ carcinoma, cervix carcinoma, bronchogenic carcinoma erkeratosis, basal cell carcinoma, squamous cell carcinoma ‘iancarcinoma carcinoma, naso-pharynx tumor, maxillary tumor, esophaqeal carcinoma, uterine body carcinoma carcinomaDeep-seated carcinoma, cervix carcinoma, bronchogenic 1 1 —@Bladder tumors :...Prostate carcinomaOvarian carcinoma5r90Pterygium, vernal conjunctivitis, vascularization of cornea Hepatomegaly and splenomegaly in advanced leukemia @ I I I — J I Other isotopes I•.' — Thyroid cancer angina pectoris congestive heart failure. hyperthyrodism Hepatomegaly and splenomegaly in advanced leukemia Control of ascites and pleural effusion in metastatic carcinoma Prostate carcinoma, cervix carcinoma, bronchogenic carcinoma 1 I used in therapy: CHART Calcium, Chromium, Gallium, Arsenic, Astatine, Ruthenium 1 .—Some therapeutic applications Evans Blue dye containing boron-lO in the mole cule (@6). Although the localization of the radio isotope achieved by use of the dye is 30 times that obtained after injection of boron-lO as borax solu tion, the localization is greatest at the brain-tumor interface and is not uniformly distributed through out the tumor tissue. Consequently, there is still insufficient localization in tumor cells to provide the needed radiation. However, the use of such boron-containing dyes should be explored. If fis sionable material can be synthesized into com pounds that will give great selective localization in neoplastic tissue, there is little doubt that great therapeutic benefit can result. Sodium-@4 and bromine-8@ have been used in the form of fluid instillation into the bladder for of radioactive Thulium, Lanthanum, Ceseum, isotopes to say that the condition can be satisfactorily con trolled by @82 (@9). The survival of patients with polycythemia treated by @32 is about equal to that in cases of pernicious anemia treated by liver or vitamin B@2and diabetes mellitus treated by in sulin (Chart @),and is superior to any increased survival rate yet achieved in such cancers as breast or prostatic cancer with newer methods of therapy (Chart 3). The median survival in pa tients with polycythemia vera is 14 years, com pared with a survival of approximately @0 years for an age-matched group of the general population. Since 1936, when @32 was first used in the treat ment of chronic leukemia (30), thousands of pa tients have been treated. As shown in Chart 3, approximately 50 per cent of the patients with Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. LAWRENCE AND ToBrJ1s—Radioactive Isotopes chronic lymphatic leukemia treated by P@ will survive over 5 years (@8). This is somewhat better than the 8urvival in 1,600 cases treated by conven tional methods reported in the literature review by Osgood (81). Between 1985 and 1940, in the early days of the radioisotope work, we attempted to treat a group of patients with breast cancer and prostate cancer metastatic to bone by means of intravenous or oral administration of @32 or Sr89 (@7, 80, 40). It had been demonstrated that strontium, like cal cium, localized to a high degree in bony tissue with less uptake than P@ in soft tissue. However, the results were not exciting, and this work was aban doned when it became evident that it would be impossible to deliver sufficient beta radiation to the bony lesions without causing severe marrow depression. Recently, Friedell (11) and others have re-introduced @32 in this form of therapy and found again that there is some relief of pain and occasional evidence of healing. This type of ther apy may have a small place in the palliation of cancer metastatic to bone. in the Treatment of Cancer 187 is pipetted onto it, and the plaque is then applied directly to the lesion. In the case of basal-cell car cinoma, a dose of 34,000—36,000 rep is delivered to the surface, and @0,000—@,500 rep delivered to the first millimeter depth in a period of 48 hours. This method is producing results equal to those of any other of the more conventional methods now in use for the treatment of superficial skin cancer. Radiophosphorus as colloidal chromic phos phate (@1),first used by Jones et at. (fl), as well as YEARS CHART3.—Survival in cancer, leukemia, and polycythemia compared with life expectancy in the general population (thin line). For polycythemia vera the dotted line represents the life expectancy after conventional forms of therapy (56) and the thick black line shows our results after treatmentwith P―(@9). For leukemia, the thick black line shows life expectancy in our patients with chronic lymphatic leukemia treated with P―(Q8) compared with average results in chronic myelogenous and lymphatic leukemia reported in the literature (dotted line) (37). For breast cancer the increased survival achieved with radical mastectomy (thick black line) over that following non radical procedures (dotted line) is shown (49). The survival rate in cancer of the prostate following the Huggins method of orchiectomy and diethylstilbesterol (thick black line) is corn pared with survival prior to Huggins' work (dotted line) (36). (0 z >1 -j z I— LU LU 0@ YEARS CHART L—The @32 compared with survival the in polycythemia survival with insulin and pernicious vitamin B-1Q. in diabetes anemia treated vera treated mellitus with treated with liver and Friedell and associates have also made Sr9°ap plicators for use in the treatment of superficial tumors of the eyelids, conjunctiva, and cornea! ulcers (1@). The treatment of skin cancer and hy perkeratoses by @32 contact therapy (31) has added another successful method for the treatment of such lesions. Since 1943 Low-Beer has treated 350 hyperkeratoses by this method with a 5-year eradi cation rate of 98.8 per cent. Of the 190 basal-ce!! carcinomas treated, 97.6 per cent have been eradi cated for longer than 5 years. Also, 47 hemangio mas have been successfully treated by this meth od. A small plaque of blotting paper is cut to fit the size of the lesion, the desired amount of Na2HP32O4 colloidal radiogold (p2,14, @4)and radioyttrium, is being currently given to patients suffering from pleural and ascitic effusions in metastatic car cinoma. This application of radioisotopes consti tutes an important addition to palliative cancer therapy. Although there is no evidence that such therapy prolongs life, there is little question that it relieves pain in many instances and slows down the accumulation of ascitic and pleural fluids, so that paracentesis is often unnecessary or need be done at less frequent intervals. Colloidal chromic radiophosphate and radio gold are also being used interstitially for the treat ment of carcinoma of the prostate before distant metastases develop (8, 9, 46). The beta radiation from these colloids allows a large tumor dose of radiation to be given without damage to surround ing tissues, as might occur with conventional x-ray Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. 188 Cancer Research therapy. Some workers point out the fact that chromic radiophosphate has an advantage over radiogold in that the former emits only beta rays, and less elaborate radiation protection measures are needed. However, other workers believe that radiogold gives a somewhat better therapeutic ef feet because the greater penetration of the gamma radiation will, with the beta radiation, in effect give a more uniform dose. Radioactive Y@ (@3) and chromic phosphate (45) beads and radon im plants (10) have been used for destruction of the pituitary in certain types of cancer. The tech nics for distributing radioactive materials in tis sue may be improved in the future in some cases by the intra-arterial injection of the radioactive materials. In 1948 we used colloidal chromic radiophos phate in the treatment of a group of patients with chronic leukemia, polycythemia vera, and also a group with marked splenomegaly or hepatomegaly from miscellaneous causes (6, @).We found these results no better than those following P@, as Na@RP@O4, and, because of the chances of getting the radiocolloid outside the vein with resultant radionecrosis, we have more or less abandoned the use of the various radiocolloids for the treatment of this group of diseases. Gofman and associates used many other radiocolloids in the same group of diseases and arrived at the same conclusion (6). Cobalt-60 is being used in intracavitary and in terstitial therapy of nasopharyngeal and maxillary tumors and uterine, prostatic, bladder, and bron chogenic carcinomas. In general, it is too early to evaluate the results in comparison with those achieved by conventional means of therapy. Hin man and co-workers (18, 47) treated 85 patients with bladder tumors by intracavitary irradiation using cobalt-60. They report that in four of nine patients with tumor confined to the mucosa the lesions were destroyed, but most infiltrating le sions were only temporarily arrested. The cobalt bomb teletherapeutic units are of wide interest now and are being used as substitutes for @00kv. x-ray equipment in the treatment of deep-seated tumors. Radiocobalt provides the gamma ray source in these units, but other gamma ray emitters such as cesium are also being used, especially in Great Britain. These teletherapeutic units have certain advantages over x-ray equip ment, such as cost and mobility, but one cannot expect much improvement in end results over con ventional methods which use x-ray or other gam ma ray sources. Since the first therapeutic use of radioactive iodine (15, 16, 17, 80), it has been widely applied in the treatment of hyperplastic thyroid disease or Grave's disease; indeed in many hospitals it is entirely replacing surgery, and remarkably good end results are reported (5, 34). In the case of thyroid cancer, however, it is rare that radioiodine will localize sufficiently in a metastatic lesion to give a good therapeutic result or cure, even after complete thyroidectomy or after a long course of propylthiouracil or thyroid-stimulating hormone (43). The cases in which there is a good uptake of radioiodine, however, give one increas ing confidence that if selectively localizing corn pounds can be found, lasting benefits might be obtained in advanced cancer of other types also. Figure 1 is a gamma ray picture of the localiza tion of I's' in the body of a patient with thyroid rnetastases obtained in the first whole-body scan ner now so widely used. This whole-body scintilla tion scanner, developed by Anger and Tobias (8) for photographing gamma ray-emitting isotopes in the body, is shown in Chart 4. It consists of a series of scintillation counters within lead cylinders. The gamma ray energy from the isotope within the body is converted to light energy and photo graphed with a polaroid camera as the body is scanned. New methods for visualizing the distri bution of radioisotopes in vivo, such as the one de scribed here or the gamma ray pinhole camera (85), are expected to be of indirect use to therapy through more accurate localization of tumors. The patient illustrated in Figure 1 was a 68-year-old male with thyroid metastases in the left upper arm, the chin, the sternum, the hip, the thigh, and the ribs. Interestingly enough, two of these lesions were not discernible by x-ray examination, yet they could be picked up by the scanner. This method of locating tumors would of course have important diagnostic applications if localizing compounds emitting gamma rays could be found for other types of cancer. This particular patient had the largest uptake of radioactive iodine in metastatic lesions that has come to our attention. Comparative counting rates over the tumor and an equal volume of normal tissue showed that the tumor concentration of I's' was as much as @00 times that in an equal volume of normal tissue. During therapy with an oral dose of 100 mc. of J131, as much as 100,000 rep in radiation was deliv ered to the neoplastic lesions. Prior to surgical thyroidectomy there was no uptake in these me tastases. Now, 6 years later, this man is symptom free, and, at the age of 74, he is an example of the good result that can be obtained with isotope ther apy when there is a high selective uptake by neo plastic tissue. Uptake in metastases can be stimu lated by surgical thyroidectomy, and administra tion of propy!thiouracil and thyroid-stimulating hormone are also sometimes helpful in increasing iodine uptake in metastases (48). Another diffi culty encountered in the treatment of metastatic Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. LAWRENCE AND T0BIAS—Radioactive thyroid cancer with radioiodine is that the radia tion dose may not be uniformly distributed in the tumor tissue. Surgery and x-ray continue to be the primary tools for treating thyroid cancer. The high selective localization of iodine in thy roid tissue and also the selective uptake of radio phosphorus by the bone marrow and blood-form ing tissues allow us to deliver relatively high doses of radiation to specific tissues. Perhaps in our present state of relative ignorance regarding the metabolic differences between the cancer cell and normal cell, it is too much to expect that a radio active compound can be found which will localize in cancer cells selectively enough to give V5, 50, or more times the radiation than normal cells will SCHEMATIC Isotopes in the Treatment of Cancer 189 planted melanosarcoma. There was some localiza tion in the melanosarcomatous tissue, but there TYROS/NE HOQI' —C--C—C—OH 4@O ii H NH2 was an appreciable uptake by the adrenal and thyroid glands, since tyrosine is a precursor of the hormones produced by these tissues. The metabolism of stilbamidine containing C14 was studied in multiple myeloma, and, while it did DIAGRAM CHART4.—Diagram of the scintillation receive. If such is to be found, the ideal isotopes to be built into the localizing compound would seem to be hydrogen-S or carbon-14. The latter provide relatively soft beta rays traveling only a few cell diameters in tissue. Many workers have attempted to synthesize compounds containing radioactive carbon and other radioelements for selective localization. Reid and Jones (44) made C'@-labeled tyrosine and in jected some of it into animals carrying a trans scanner (from Anger et at.) localize in the myelomatous tissue, there was an even greater uptake by the liver. These examples are typical of the many coin ST//JAM/DINE Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. Cancer Research 190 pounds that have been synthesized—localization of the radioactive compound is not sufficiently lim ited to the neoplastic cells to permit a good dose of radiation to be given without damage to normal tissue. Some of the most interesting current investiga tions on selective localization are typified by the studies of Pressman and associates (41) . After im munizing animals to various normal tissues and neoplastic tissues and then adsorbing radioactive iodine to the antibodies, they have been able to demonstrate some localization of these antibodies • Chronic lymphatic leukemia (131) Chronic myelogenousleukemia (138) • Breast cancer, radical mastectomy (125, Univ.of Rochester) • Stomach cancer (2772, Mayo Clinic Lung cancer, pneurnonectomy (202, G.A Mason) 0 z > > U) I z w C.) 3 This LU a. YEARS CHART 5.—Survival rates in chronic lymphatic leukemia treated with P@ (@8), in breast cancer treated by radical mastectomy (49), in stomach cancer treated by gastric resec tion (57), and lung cancer treated by pneumonectomy (33). in the various normal and neoplastic tissues. More recently Bale2 has achieved tumor localization of such antibodies 15 times greater than that of any normal tissue, indicating that this approach may be a very hopeful one (4, 50). The therapy of cancer continues to be based primarily on early diagnosis, surgery, and post operative x-ray therapy. Radioactive isotopes and nuclear energy have not yet added importantly to the armamentarium of cancer therapy, but the relatively poor survival in cases of deep-seated cancer impels investigators to make heroic at tempts to relieve these people and extend their lives. As can be seen in Chart 5, the 50 per cent survival in the case of breast cancer, the most com mon type of cancer in women between the ages of 40 and 60, lung cancer, and stomach cancer is approximately 8-5 years. One of the real advances in cancer therapy has been the revelation of the relation of hormones to certain types of cancer, including the effects of oophorectomy, adrenalectomy, and hypophysec tomy on advanced breast cancer (4@). Two ex amples in particular are the work of Huggins in the field of prostate cancer treated by orchiectomy and diethyLstilbesterol (19), and the treatment of met * W. astatic breast cancer by adrenalectomy (@0). Olivecrona and associates were the first to report a remission in metastatic breast cancer following hypophysectomy and have recently reported the results of this form of therapy in a series of 30 pa tients (8@2).Other workers in this field have esti mated that approximately 50 per cent of patients with advanced breast cancer have tumors which are hormone-dependent, and approximately 50 per cent of the patients of this type undergoing sue cessful hypophysectomy will show some evidence of healing (38, 89). Apparently, the response is in dependent of the cellular type of mammary tumor, and whether the effect is always mediated through the ovaries and adrenals or whether there is a pri mary pituitary factor is not yet known. With the hope that hypophysectomy could be achieved by irradiation, for 15 months we have been making such attempts using a somewhat unique form of irradiation from the 184-inch cy F. Bale, personal communication, “Atomsfor Peace Conferences,― Geneva, presented August, 1955. at work is a projection of the animal studies of Tobias et at. (51, 54), who achieved hy pophysectomy in the rat, dog, and monkey with beams of high energy deuterons or protons. One unusual feature of the beam is its pencil-like nature with very little scatter, unlike a similar beam of x-rays or gamma rays. Another unusual feature of these beams is that there is a relatively greater depth dose compared with surface dose. The com parative doses at the surface and depth for @00 kv. x-rays, 16 mev electrons, and 190 mev deuterons are given in Chart 6. The @00kv. x-rays fall off markedly at 10-cm. depth, and the electrons from the betatron or synchrotron also fall ofT consider ably, but the deuteron irradiation rises to a peak at 14 cm., so that the depth dose is approximately 4 times that entering at the surface. Two animals with mammary cancer are shown in Figure @. The one on the left is the control, and the one on the right has been irradiated by passing the beam through the chest of the animal from the opposite side, localizing it on the tumor. In other words, it is possible to deliver energy in the depths of tissues with relatively little skin effect using this form of radiation. Tobias et at. have applied this beam to the pituitaries of rats, monkeys, and dogs and have been able to remove the pituitary by this selective form of external irradiation, producing atrophy of all the target organs, effects paralleling those of surgical hypophysectomy. Four litter mates are shown in Figure 8. The second from the left has had surgical hypophysectomy, and the third from the left irradiation hypophysectomy. The animal on the left has been subjected to hypo thalamic irradiation which produced obesity, and the animal on the right is the control. @Thiswork is supported by the Atomic Energy Commission, the California State Cancer Fund, and the Donner Foundation. Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. LAWRENCE AND ToBJ.@&s—Radioactive During the past year this beam has been applied to the pituitaries of patients with advanced breast cancer and to two patients with leukemia, one hay ing an associated diabetes. This work has been the subject of two previous reports which give much more detail (5@2,53). The patients with cancer have previously had every form of convention al therapy, including radical mastectomy, post operative x-ray, hormone therapy, as well as oöphorectomy and adrenalectomy, and they were no longer responding to these forms of therapy. The aim in this work has been to find out how sue cessfully one can inhibit or destroy the pituitary by this selective form of radiation as compared with surgical hypophysectomy. Figure 4 shows a lateral view of the sella turcica in one of the pa tients with the beam centered on the crosshair. It is possible to cover most of the area occupied by the pituitary within the sella with very little radia tion being delivered to the surrounding tissues, such as the hypothalamus and optic chiasm. Up to the present time, use has not been made of the Bragg curve, and the relatively great pituitary dose is accomplished by continuous head rotation, the beam being centered on the pituitary. There are real problems encountered in avoiding irradia tion of the vital structures surrounding the hy pophysis, such as the optic tracts, the hypothala mus, and the various cranial nerves. It has not been possible to give as much radiation to this area as one would like at the present time because of Isotopes in the Treatment 191 of Cancer the danger of cranial nerve damage. However, al ready in the first fourteen patients treated there is evidence of marked pituitary suppression (Chart 7). Figure 5 shows the patient in position for treat ment. Prior to irradiation the sella is very carefully brought into position by taking x-ray photographs, DEPTH IN CENTIMETERS CHART 6.—Comparative doses at surface to 15 cm. depth for @OO kv. x-rays, 16 mev electrons, and 190 mev deuterons (which are like protons in depth effects). and with the aid of crosshairs the beam is made to fall on the exact center of the sella. During treat ment the head is held tightly in a plastic mask and continuously rotated through a 60°—70° angle, 30°— @‘—I3,85ORAD—j @ (I) I zu) 50 >-o.@@: @ v@::@T:::. . -T T .. •...c.•••••. •. @tI @ k @ 60@ ______________ CHART treatment 7.—Patient M.W. .J,*, Changes in v@!:*;r pituitary I gonadotrophins, I P― uptake, and I protein-bound iodine during and after with 13,850 rads. Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. Cancer Research 19@2 85°to the right and S0°—35° to the left. The first pa tient treated (Chart 7) was given 18,850 rads, one r&d being roughly equivalent to a rep, delivered to the pituitary over a period of about a month in fractionated doses. As far as we know, the findings in this case are the first clear-cut evidence that target organ effects can be brought about by pitui tary irradiation (note decrease of pituitary gon adotrophins and marked decrease in thyroid func tion as shown by fall in I's' thyroid uptake, Chart 7). @ @ Whether or not there will be a real application of irradiation hypophysectomy, or even surgical hypophysectomy, in cancer therapy is not yet known. Another or 8 years must elapse before preliminary impressions regarding clinical benefits in this series can be gained. Also, it will require an other 5 years before it is known whether hypophy sectomy will appreciably lengthen life in advanced cancer of this or other types. While I do not intend to belittle the achieve ments of workers with artificial radioactivity and nuclear energy in cancer therapy, the results re fiected in extension of life so far are not impressive. However, when one must deal with the problem of intractable pain, he learns to appreciate any pal liative procedure which will make the patient more comfortable even if significant extension of life is not demonstrated. Radioisotopes and the new ac celerators and external sources of radiation have given us tremendously important new tools and, from the humane standpoint, have been a real boon to cancer therapy. If a selectively localizing compound or compounds can be found which would emit a soft form of radiation, the really im portant advances that could be realized are ob vious. Much more basic research including that with tracers is needed to learn more of the physiol ogy of cancer. In the search for therapeutic bene fits, our relative ignorance of the nature of neo plastic growth is emphasized, and the solution to the problem will probably not be found without greater understanding of the cancer process at the cellular level. ADDENDUM At the International Conference on Peaceful Uses of Atomic Energy held at Geneva in August, 1955, the author talked at length to numerous Russian investigators and learned that during the past 3—Syears they have been very active in Fio 1.—A scintogram at various times after applying the products of nuclear physics, especially isotopes, to therapy, particularly in the use of 1131in Grave's disease, P― in the treatment of polycythemia vera and leukemia, and the cobalt teletherapeutic units for external irradiation treatment of cancer. REFERENCES 1. AEBERSOLD, P. C. U.S. Atomic Energy Commission.Eight Year Summary of U.S. Isotope Printing Office, 1955. @.ANDREWS, RoOT, S. W.; Knaai@i, Goveimment H. D.; and B1GEWw, R. R. Intracavitary Colloidal Radiogold in the Treatment of Effusion Caused by Malignant Neoplasm. Ann. Surg., 137:375—81, 1953. 3. ANGER, H. 0. A Multiple Scintillation Counter in Vivo@ Scanner. Am. J. Roentgenol. Rad. Therapy & Nuclear Med., 70:605—ig,1953. 4. W. F., and Sp@tn,I. L. In Vivo Localization of Rat Organ Antibodies in Ovaries, Adrenals, and Other Tissues. J. Immunol., 73:125—33, 1954. 5. CHAPMAN, E. M.; M@oop, MARTiN, J. M. Ten Years' F.; M@is@ra@un@A, J.; and Experience with Radioactive Iodide. J. Clan. Endocrinol. & Metabol., 14:45—55, 1954. 6. DOBSON, E.; Knu@y, L. ; JONES, H. ; and Gorst@, J. Radioactive Substances Specifically Localized in Liver, Spleen, or Bone Marrow, pp. @6—@7. XVII Interuat. Physiol. Congress, Oxford, England, July, 1947. 7. F@a, L. E.; Swsmr, W. H.; ROBERTSON, J. S.; FOSTER, C. G.; LOCESLEY,H. B.; Sum@i@n, D. L.; MENDELSON, M. L.; and STICKLEY, E. E. Neutron Capture Therapy with Boron in the Treatment of Glioblastoma Multiforme. Am. J. Roentgenol. Rad. Therapy & Nuclear Med., 71:g79—91, 1954. 8. Fwcxs,R.H.;KmtR,H.D.;EixiNS,H.B.;andCuu',D. Treatment of Carcinoma of the Prostate by Interstitial Radiation with Radioactive Gold (Au198). J. Urol., 68: 51o•-@. 9. . Treatment of Carcinoma of the Prostate by Inter stitialRadiation with Radioactive Gold (Au198): Follow-up Report. Ibid., 71:6@8—SS,1954. 10. FoRREST, A. P. M., and BROWN, D. A. Pituitary Radon Implant for Breast Cancer. Lancet, 268: 1054—55,1955. 11. FRIEDELL,H. L., and STORAASLI,J. P. The Use of Radio active Phosphorus in the Treatment of Carcinoma of the Breast with Wide-spread Metastases to Bone. Am. J. Roentgenol. & Rad Therapy, 46:559—75, 1950. 1@. FRIEDELL, H. L.; THoseas, C. I.; and KnoHirnt, J. S. De scription of an Sr9°Beta-Ray Applicator and Its Use on the Eye. Am. J. Roentgenol. & Rad. Therapy, 65:@3@—44, 1951. 13. GODWIN, J. T.; F@uu1, L. E.; SWEET, W. H.; and ROBERT SON, J. S. Pathological Study of Eight Patients with Glioblastoma Multiforme Treated by Neutron-Capture Therapy Using Boron-lO. Cancer, 8:601—15, 1955. 14. Goura, H., and ILtsIN, P. F. Distribution and Effect of Colloidal Radioactive Gold in Peritoneal Fluid Containing Free Sarcoma 87 Cells. Proc. Soc. Exper. Biol. & Med., 74:634—38, 1950. 15. HAMILTON,J. G., and LAWRENCE,J. H. Recent Clinical Developments in the Therapeutic Application of Radio of a patient injection G. A.; Distribution. with thyroid metastases of a tracer dose of 1131. The scintillation scanner passes back and forth over the body, translating the gamma ray energy from the I's' within the body into light energy, which is then photographed with a Polaroid camera. Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. / I I / I'..' / • - •-- / o@ 0 ••=-=@ ii I % t -@=-@- @ I • ‘I @T@? .1.... I I I i ‘I II I @ j@ 1 ,@ it I I t I HOUR 48 HOURS I I I I I I II I i I I I 96 HOURS I. Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. Fia. g.—A: Control animal with untreated mammary tu mor; B: Healing tumor after bombardment with 190 mev deuterons. The beam of deuterons was directed to the tumor through the opposite side of the animal's body. FIG. 8.—Four radiation, radiation littermates (left to right): producing obesity; surgical hypophysectomy; control. FIG. 4.—Diagnostic hypothalamic hypophysectomy; x-ray of a patient's head in position ir ir for treatment. The crosshairs mark the center of the beam. The outlines of the sella turcica are clearly shown. The black spot on the film on the left shows the shape of the beam, be adjusted to fit each patient. The radioautograph briefly turning on the proton beam prior to developing which can is made by the film. The beam spot is actual size, while the x-ray picture of the sella is enlarged by @0per cent owing to the finite focal distance of the x-ray machine. FIG. 5.—Patient beam. in position for irradiation with the proton Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. rC) Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. LAWRENCE Phosphorus AND TornAs—Radioactive and Radio-Iodine. lsotopes J. Clin. Investigation, 21: 6@4,1942. tion, 21:624, 1942. 18. HzNuaN, F., Ja.; SCHULTE, J. W.; and LOW-BEER, B. V. A. Further Experience with Intracavitary Radiocobalt for Bladder Tumors. J. Urol., 73:285—91,1955. C. Prostatic ment C., and DAO, T. L-Y. of Advanced Carcinoma Adrenalectomy in Treat of the Breast. J.A.M.A., 151:1388—94,1953. 21. JAFFII, H. L. Treatment of Malignant Serous Effusions with Radioactive Colloidal Chromic Phosphate. Am. J. Roentgenol. Rad. Therapy & Nuclear Med., 74:657-66, 1955. @. Joiras, B.; WROBEL, C. G.; and LYONS, W. R. A Meth od of Distributing Beta-Radiation to the Reticulo-endo Tissues. J. Clin. Investiga Useofa Beta-Ray Source forDestruction sis. Siug. Forum, 4:681—86, 1958. of the Hypophy @24. KiNG, E. R.; Spzczia, D. W.; DOWDA,F. W.; BENDrn, M. A.; and NOEL, W. E. The Use of Radioactive Gold (Au1N) in Pleural Effusions and Ascites Associated with Malignancy. Am. J. Roentgenol. Had. Therapy & Nuclear Med., 68:416—20, 1952. 25. KRUGER, P. G. Some Biological Effects of Nuclear Dis integration Products on Neoplastic Tissue. Proc. Nat. Acad. Sc., 26:181—92, 1940. . Boron Uptake in Mouse-Brain Neoplasms. Radia tion Research, 3:1—17,1955. @7.Lawunrwsi, J. H. Observations on the Nature and Treat meat of Leukemia and Allied Diseases. Proc. Inst. Med. Chicago, 14:30-49, @8. Evaluation of Endocrine 1942. . The Treatment of Chronic Leukemia. Med. Clinics N. America, 38:525-40,1954. 29. —. Polycythemia Vera: Physiology, Diagnosis, and Treatment, pp. 69—70.New York: Grune & Stratton, 1955. 80. L&wum@cE, I. H.; IhssiLTON, J G.; Ear, L. A.; and PECHER, C. Recent Advances in Clinical Aid of Artifically Prepared Radioactive Investigation, 20:436, 1941. Therapy for Ad 154:234-39,1954. 46:86—91, 1941. 41. Punseaw@, D. Antibodies as Specific Chemical Reagents. In: J. H. Lawrence and C. A. Tobias (eds.), Advances in Biological and Medical Physics, 3:99—152.New York: Academic Press, 1953. 42. RAWSON,R. W. Hormonal Control of Neoplastic Growth. 43. RAWSON,R. W. ; Rai,L, J. E. ; and ROBBINS,J. Uses and Misuses of Radioactive Iodine in Treatment of Cancer of Thyroid. A.M.A. Arch. Int. Med., 92:299-807, 1958. 44. RaiD, J. C., and JONES,H. B. Radioactivity Distribution in the Tissues of Mice Bearing Melanosarcoma after Ad ministration of DL-Tyrosine Labeled with Radioactive Carbon. J. Biol. Chem., 174:427—37, 1948. 45. ROTBENBERG, S F.; [email protected], H L.; Pum@us,T. J.; and B. Medicine Isotopes. with the J. Cliii. 81. Low-B@a, B. V. A. The Therapeutic Use of Radioactive Hypophysectomy with Radioactive Chromic Phosphate in Treatment of Cancer. A.M.A. Arch. Neurol. & Psychiat., 73:193—99, 1955. 46. RTJSCEE,C., and Jai@t, H. L. The Treatment of Prostatic Carcinoma @23. KENNEDY,T. ; RASMUSSEN, T., and H@uu'zu,P. V. The 26. E. 193 of Cancer 40. PECHER, C. Biological Investigations with Radioactive Calcium and Strontium. Proc. Soc. Exper. Biol. & Med., SIMK.IN, H. thelial System and Adjacent tion, 23:783—88, 1944. @ ‘fREVES, N. Treatment Bull. New York Acad. Med., 29:595—611, 1953. Cancer Treated by Orchiectomy. The Five-Year Results. J.A.M.A., 131:579-81, 1946. @0.Huoan@s, the vanced Breast Cancer. J.A.MA., 16. HAMIIJTON, J. G., and Soi@ziy, M. H. Studies in Iodine Metabolism by the Use of a New Radioactive Isotope of Iodine. Am. J. Physiol., 127:567—72, 1939. 17. Huni'z, S., and ROBERTS, A. Application of Radioactive Iodine in Therapy of Grave's Disease. J. Clin. Investiga 19. lluoonis, in (i@E) with Radioactive Trans. Am. Assoc. Colloidal Chromic Phosphate Genito-urinary Surgeons, pp. 48—56,1953. 47. SCEULTE, J. W.; Hiintair, J., JR.; and LoW-B@, B. V. A. Radiocobalt for Treatment 67:916—24, 1952. of Bladder Tumor. J. Urol., 48. Sumur@r,S. M.; Rossatar', I.; OSERY,E.; and SIEGEL,E. Radioiodine Therapy of Metastases from Carcinoma of the Thyroid: a Six-Year Progress Report. J. Clin. EndocrinoL, 9:1122—37, 1949. 49. Satau@, R. G., and DtrrroN, A. M. Survival of Patients with Cancer of the Breast.J.A.M.A.,157:216—19, 1955. 50. Sp@ii, I. L., and W. F. In Vivo Localization of La beled Rat Adrenal Antibodies. J. Iminunol., 73:134-37, 1954. 51. T0BIAS, C. A.; Airoun, H. 0.; and LAWRENCE, J. H. Radiological Use of High Energy Deuterons and Alpha Particles. Am. J. Roentgenol. Rad. Therapy & Nuclear Med., 67:1—27, 1952. 52. T0BIAS, C. A.; ROBERTS, J. E.; L@wumic@, J. H.; Low Bumi, B. V. A.; ANGER,H. 0.; Bousi,J. L.; McCoums,R.; and Huosin@s, C. Radiation Hypophysectomy with High Energy Proton Beams. Univ. of Calif. Radiation Lab. Report 3035, 1955 58. . Pituitary Irradiation with High-Energy Proton Beams: A Preliminary Report. Cancer (in press). Isotopes, GP, pp. 69—87.1954. 32. Lurr, R., and OL1VECRONA,H. Hypophysectomy in Man. Experiences in Metastatic Cancer of the Breast. Cancer, 8:261—70, 1955. 54. TOBIAS, C. A.; Vaii Dm@, D. C.; SiupsoN, M E.; ANGER, 83. MASON,G. A. Cancer of the Lung: Review of 1,000 Cases. 1954. 55. T0BIAS,C. A.; WEYMOUTU, P. P.; and WAssmuwi, L. R. Lanoet, 2:587—90, 1949. 34. McCuiiaoii, E. P. Radioactive Iodine in the Treatment of Hyperthyroidism. Ann. mt. Med., 37:739—44,1952. 35. Mois'rnsiiu, R. K.; ANGER, H 0.; and T0BIAS, C. A. The Gamma-Ray Pinhole Camera and Image Amplifier. Univ. of Calif. Radiation Lab. Report 2524, 1954. 36. NESBrr, R. M., and BAtm&,W. C. Endocrine Control of Prostatic Carcinoma. J.A.M.A., 143:1317—20,1950. 37. Osooor, E. E., and Snass@&N,A. J. Treatment of Chronic Leukemias. J.A.M.A., 150:1372—79, 1952. 38. PEARSON,0. H.; RAY, B. S.; HAluIou, C. C.; WEST, C. D.; Li, M. C.; MACLEAN, J. P.; and LIPSETr, M. B. Hypophy sectomy in the Treatment of Advanced Cancer. Trans. Am. Assoc.Phys. (inpress). 39. PEARSoN,0. H.; WEST, C. D.; H0LI.ANDER,V. P.; and H. 0.; Hurr, R. L.; and Ko@iw, A. A. Irradiation of the Pituitary of the Rat with High Energy Deuterons. Am J. Roentgunol. Red. Therapy & Nuclear Med., 72:1—fl, Some Biological 107:115-18, Effects Due to Nuclear Fission. Science, 1948. 56. VIDEBARK,A. Polycythemia Vera—Courseand Prognosis. Acta Med. Scandinav., 138:179—87,1950. 57. WALTERS,W.; GEAY,H. K.; and Paizsmzv, J. T. Car cinoma and Other Malignant Lesions of the Stomach. Philadelphia: W. B. Saunders, 1942. 58. WALTON, R. J., and Sz@ci.@uR,W. K. Radioactive Solu. tions (24Na and EBr) in the Treatment of Carcinoma of the Bladder. Brit. Med. Bull., 8:158—65, 1952. 59. ZAHL, P. A.;Coopun, F. S.;and DUNNnW, J.R. Some i* Vivo Effects of Localized Nuclear Disintegration Products on a TransplantableMouse Sarcoma. Proc. Nat. Acad. Sc., 26:589, 1940. Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research. Radioactive Isotopes and Nuclear Radiations in the Treatment of Cancer John H. Lawrence and Cornelius A. Tobias Cancer Res 1956;16:185-193. Updated version E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cancerres.aacrjournals.org/content/16/3/185.citation Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cancerres.aacrjournals.org on June 14, 2017. © 1956 American Association for Cancer Research.