Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
Human T-cell Leukemia Virus Type I t a x h e x DNA and RNA
in Cutaneous T-cell Lymphoma
By Subrata K. Ghosh, J. Todd Abrams, Hiroshi Terunuma, Eric C. Vonderheid, and Elaine DeFreitas
Peripheral blood mononuclear cells (PBMCs) and T-cell lines
from patients with Sezary syndrome (SS) and skin lesions
from patients with mycosis fungoides(MF) were examined
by polymerase chain reaction (PCR) for DNA sequences homologousto thehuman retroviruses human T-lymphotropic
virus (HTLV)-I and -11. Results obtained using primers and
probes from the taxhex region of HTLV-I indicatethat 72%
(18/25) of SS patients PBMCs, 8OYo (20/25) of T-celllines
established from SS-PBMC, and 30% (3/10) of skin lesions
from MF patients were positive for HTLV-I taxhex region
DNA. Sequence analysis of the 127-bp fragment amplified
by the tax/rexprimers from 4 of these individualswas found
to be identical to that in prototypic HTLV-I. Negative results
were obtained using primers and probes from the HTLV-I
gag region and the HTLV-II gag and tax regions. No PCR
products were obtained using all primers and probes using
DNA from 9 healthy blood donors and 10 cord bloods. Expression of HTLV-I tax/rex mRNA was found in 4 of 8 Sezary
patients, as determined by RNA-PCR, indicating that this
viral regionis being transcribedin vivo. Exposureto Tax/Rex
protein in SS-patients is supported by the fact that serum
antibodies against p27"" and p40"" was observed in 43%
and 29% of these SS patients, respectively. Although the
causal relationship between the HTLV-I taxhex region and
cutaneous T-cell lymphoma (CTCL) remains unclear, these
findings support the presence of atruncated HTLV-I retrovirus in CTCL patients.
0 1994 by The American Society of Hematology.
C
for the expression of t d r e x mRNA inthe PBMCs of several
SS patients.
UTANEOUS T-CELL lymphoma (CTCL) is a lowgrade malignancy thought tobegin in the skin and
then to be involved in the lymphoid tissue, peripheral blood,
and visceral organs.'.' CTCL includes mycosis fungoides
(MF) and the leukemic variant called Sezary syndrome (SS).
SS is characterized by circulating clonal neoplastic T cells
with cerebriform nuclei and a surface phenotype that is typically CD3+, CD4' and CD45 R o + . ~
The etiology of CTCL remains unknown. Because CTCL
has clinical, pathologic, and immunogic similarities with human T-lymphotropic virus-I (HTLV-I)-associated adult Tcell leukemia (ATL), weand other investigators have attempted to determine whether a retroviral agent is involved
with its pathogenesis. In 1987, Manzari et a14 observed budding retroviral-like particles from CTCL cells and designated
them HTLV-V. This virus has not yet beenmolecularly characterized. In 1991, Hall et a
'lsuggested that a partially deleted HTLV-I provirus is associated with MF in non-HTLVI endemic areas. In the same year, Zucker-Franklin et a16.'
reported HTLV-I-like particles in cultured lymphocytes of
18 of 20 consecutive MF patients. Recently, reports from
these investigators indicate the presence of tax gene specific
for both HTLV-I and HTLV-I1in peripheral blood mononuclear cells (PBMCs) from a patient with MF.' A small percentage of patients with classical MF have serum antibodies
directed against HTLV-L9 Serologic studies by enzymelinked immunosorbent assay (ELISA) on more than 200
American patients with CTCL showed that less than 1%
were HTLV seropositive. Subsequently, it was also shown
that 11% of CTCL patients in Europe had low titers of
antibody against HTLV-I antigen."
To establish an in vitro model for CTCL, our laboratory
successfully established interleukin-2 (IL-2)-responsive Tcell lines from blood of 25 American patients with SS3 who
were HTLV-I seronegative by ELISA." To detect the presence of HTLV-I provirus present in these cell lines, we used
semiquantitative polymerase chain reaction (PCR)." We report here the preferential retention of the HTLV-I tax/rex
region but not the gag region in studies with 25 SS patients,
using PBMCs, T-cell lines established from SS PBMCs, and
skin biopsy specimens from 10 HTLV-I-seronegative MF
patients. In addition, we provide evidence for the first report
Blood, Vol 84, No 8 (October 15). 1994: pp 2663-2671
MATERIALS AND METHODS
Cell isolation and culture. Peripheral blood obtained from several patients with SS was fractionated by Ficoll-Hypaque density
centrifugation to recover PBMCs and to establish cell lines as described by Abrams et al."
Oligonucleotide preparationand location of primers and probes.
All the oligonucleotides were synthesized on automated DNA synthesizer (Model 380; Applied Biosystems, Foster City, CA) and
were purified by high performance liquid chromatography for use
as probe; 50 to 100 pmol of an oligonucleotide was end-labeled by
T4 polynucleotide kinase (GIBCO, Grand Island, NY) withhigh
specific activity y (3zP)dATP (NEN, Boston, MA) and separated
on a Sephadex G-50 (Pharmacia, Piscataway, NJ). The amplification
primers were (1) G-1-1 (+) (863-886), (3-1-2 (-) (1353-1379), and
G-1-3 (probe) (1080-1101) corresponding to HTLV-I gag genome
(product size, 535 bp); (2) G-2-2 (+) (813-838). G-2-1 (-) (11871214), and G-2-3 (probe) (1080-1105) corresponding toHTLV-I1
gag genome (product size, 409 bp); (3) T-1-1 (+) (7598-7619). T1-2 (-) (7703-7724), and T-1-3 (probe) (7675-7700) corresponding
toHTLV-I radrex genome (product size, 127 bp); (4) T-2-1 (+)
(7602-7620), T-2-2 (-) (7900-7920), and T-2-3 (probe) (7819-7846)
corresponding to HTLV-I1 tax genome (product size, 319 bp); (5)
T-1,2-1 (+) (7248-7267), T-1,2-2 (-) (7386-7406), andT-1.2-3
(probe) (7337-7376) corresponding to bases of HTLV-I1 tax genome
From the Department of Medicine, University of Miami, School
of Medicine, and Miami Veterans Administration Medical Center,
Miami, FL; and the Department of Medicine, Divisionof Dermatology, Hahnemann University, Philadelphia, PA.
Submitted December 10, 1993; accepted June 8,1994.
Supported by National Institutes of Health Grant No. CA-48484
(E.D.), the American CancerSociety (E.D.), the Eleanor Naylor
Dana Foundation (E.D.),and the Concern Foundation (J.T.A).
Address reprint request to Subrata K . Ghosh, PhD, University of
Miami, School of Medicine,Department of Medicine,PO Box
016960 (M818), Miami, FL 33101.
The publication costsof this article were defrayedin part by page
chargepayment. This article must therefore behereby marked
"advertisement" in accordance with 18 U.S.C. section 1734 solely to
indicate this fact.
0 1994 by The American Society of Hematology.
0006-4971/94/8408-0026$3.00/0
2663
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
2664
(product size, 159 bp), this region is also common to HTLV-I and
-11 tar HTLV-Iand -11 areGenbankaccessionnos.
J02029 and
K02532, respectively.
Isolation of DNA. DNA was extracted from the patient's freshly
isolated PBMCs as well as from cultured T cellsby sodium dodecyl
sulfate (SDS)/proteinaseK digestion followed by phenol-chloroform
extraction using a nucleic acid extractor (Applied Biosystems). Control DNA was prepared from PBMCs obtained from cord bloods as
well as healthyindividuals,MT-2(HTLV-Iinfected),andMOT
(HTLV-I1 infected) cell lines. The DNA was removed from the
filter
( 5 U precipitettecartridge;AppliedBiosystems)bydissolving
in
double distilled water. DNA concentration were estimated by mea260/280. DNA extraction was performed
suring optical density at
with freshly made reagents and equipment that
is physically separated from pre- and post-PCR reagents and equipment.
Amplijcation and analysis of amplijed DNA. PCRwasconductedafter initial optimizationofMgz+concentration
of each
primer set (datanot shown). Two micrograms of DNA was amplified
through 30 repetitive three-step cycles of PCR with incubations for
1 minuteeachat
95°C and 55°C andfor 2 minutesatthe 72°C
extension temperature. All amplifications were performed in a Perkin-Elmer Cetus Thermal Cycler (Perkin-Elmer Cetus, Norwalk, CT)
in wells tested for uniform PCR product generation. The 100 pL of
PCR reaction mixture contained 2 pg of sample DNA; 278 pmol/L
each of dATP, dCTP, dGTP, and TTP; 0.8 pmol/L of each primer:
10 mmol/L Tris/HCI (pH 8.3); 50 mmol/L KCI; 1.5 of mmol/L
MgClz (except for PCR of HTLV-I
?&rex region, in which optimum
MgClzconcentrationis0.75
mmoUL); 0.01% (wt/vol)gelatin
(Sigma, St Louis, MO); and2.5 U of Thermus aquaticus polymerase
(Taq) enzyme" (Perkin-Elmer Cetus). We performed DNA extraction and PCR in separate areas using positive displacement pipettor
toavoidcontamination.AfterPCR,
25 p L of the final amplified
reaction product was analyzed by electrophoresis on 1.2% agarose
gel ( 1 50 V for 2 to 3 hours). The gel was denatured and neutralized
andtheDNAweretransferredtoNytrannylonmembrane
(S&S
Nytran) by blotting. Thefilter was soaked with2X SSC for5 minutes
at room temperature and baked at 80°C for 2 hours under vacuum.
The prehybridization buffer consists of 6X SSC, 0.5% SDS, 50%
formamide, 5 X Denhardt's solution, and 150 pg/mL herring sperm
DNA. The filter was prehybridized overnight at 37°C and then hybridized overnight with 5' end-labeled (12 X IOh cpm) probe (specific for the appropriate region)
in prehybridization buffer. Filters
were then washed with (I)2 X SSC/O.I% SDS (two times for 20
minutes at room temperature),(2) 0.2X SSC/O.I% SDS for 20 minutes at room temperature, (3) 0.1 x SSC/O.I% SDS (30 minutes at
37°C and l hour at 45°C). Autoradiography was performed with two
intensifying screens (Cronex Hi Plans; Dupont, Wilmington, DE) at
-70°C with Kodak X-AR-5 film (Eastman Kodak, Rochester, NY).
The sensitivity of PCR results was determined by extracting DNA
from HTLV-I (13-4) or HTLV-I1 (MO-T) producer serially diluted
(20 ng, 2 ng, 200 pg, and 20 pg) with 2 pg HTLV-I, I1 negative
U937 cellular DNA, and then subjected to PCR analysis.
RNA isolation. Total RNA was isolated from either SS-PBMC or
MT-2 cell line by a modification of the guanidinium isothiocyanate
method of Chomczynski et al.'4
Reversetranscription
and PCR(RNA-PCR).
RNA-PCRwas
performedas d e ~ c r i b e d 'with
~ minormodification.
Briefly, total
RNAs (2 pg) from SS PBMCs was treated with IO U of DNase I
(RNase free; Boehringer Mannheim, Indianapolis, IN)30for
minutes
at 25"C, followed by 5 minutes at 100°C. This treated RNA then
annealed with 2.5 pmol/L of a random hexamer primer and was
reverse transcribed into cDNA in reaction mixture 20 pL (5 mmol/
L MgCI2, 1 mmol/L each of dATP, TTP, dGTP, dCTP, 1 U RNase
inhibitor,2 pL 10 X reactionbuffer) by adding 2.5 U Moloney
murine leukemia virus reverse transcriptase (Perkin-Elmer Cetus) at
GHOSH ET AL
42°C for 45 minutes followed by a denaturation of enzyme at 99°C
for 5 minutes. The resulting cDNA (20 pL) were added to X 0 pL
of PCR cocktail (PCR buffer 11 without MgCI?), S0 pmol of each
5' (T-1-1) and 3' (T-1-2) primer (from
tudr(>x region of HTLV-I
genome), and 2.5 U of taq polymerase (Perkin-Elmer Cetus). PCR
was performed in DNA Thermal Cycler (Perkin-Elmer Cetus) for
of
40 cycles as described before. Because optimum concentration
MgCI2 in PCR usingaboveprimer is 0.75mmol/Lnoadditional
MgCI, is required for PCR step. Analysis of RT-PCR product in gel
was performed exactly as described above for regular PCR.
Cloning and sequencing ofthe umplified fragment. After amplification, the PCR-generated product was directly cloned
into PCR
IIvector (supplied with PCR I1 cloning kit; Invitrogen. San Diego.
CA) transformed into Escherichia coli and, after plating. incubated
overnight at 37°C. The resulting colonies were screened
by a "P
end-labeled oligonucleotide probe (T- 1-3). The cloned DNA were
purified from E coli and sequenced by the dideoxy chain termination
method of Sanger et all" with T7 DNA polymerase (Sequenase; US
Biochemical Corp, Cleveland, OH) and a-(''S)-dATP.
Reversetrunscriptnse L I S S U ~ . To detect potential virus,culture
fluid washarvestedfromthreecycles
of freezing at -80°C and
subsequent thawing and was then centrifuged in a Sorval RC-SB at
2,000 rpm for IO minutes at 4°C to remove intact cells. The supernatant fluid was then recentrifuged at 10.000 rpm for l5 minutesto
sediment cellular debris. Finally, potential viral particles were pelleted at 25,000 rpm for 90 minutes in an SW 28 rotor in a Beckman
ultracentrifuge. The pellet was suspended in 500 p L ( l00X concentration)TNEbuffer
(10 mmol/LTris/HCI, pH 8.0, 100 mmol/L
NaCI, I mmol/L EDTA) and tested immediately. The reverse transcriptase activity was determined i n a reaction mixture of 1 0 0 pL
containing S0 mmol/L Tris/HCI, pH 8.0,40 mmol/L KCI. 30 mmol/
L MgCI,, 5 mmol/L dithiothreitol (DTT), 0.05% TritonX-100, 0.2%
Nonidet P-40 (NP-40), 100 pg/mL bovine serum albumin, 40 pg/mL
template-primer complex poly (I€) oligo (dG) (Pharmacia). After S
minutes on ice, 6.6 pmol/L ('H) dGTP (I1 Ci/mmol); Amersham,
Arlington Heights, IL) was added to the mixture and incubated at
37°C for 60 minutes with repeated shaking. Thereaction was stopped
by the addition of ice-cold 10 mmol/L sodium pyrophosphate and
l S % trichloracetic acid (TCA). After 15 minutes at 0°C. the TCA
precipitable ('H) poly G synthesized in this reaction was collected
on glass microfibre filters (Whatman GF/C; 2.4 cm) presoaked in
5% TCA. Thefilters washed 10 times with ice-cold 5% TCA, dried.
placed in scintillation cocktail, and counted."
Wesrrrn blot analysis. The procedure for Western blot analysis
of retroviral protein has been described by severallaboratories.Ix
Proteins of HTLV-I from MT-2lysates were separated by SDSpolyacrylamide gel electrophoresis andthen transferred to nitrocellulose paper in a transblot electrophoresis cell (BioRad Laboratories,
Richmond, CA) at 250 mA for 4 hours following the manufacturer's
instructions. The nitrocellulose sheets were cut i n strips. To detect
the binding of patient sera to reactive proteins. we used the ProtoBlot
I1 AP system with stabilized substrate for human primary antibodies
(Promega, Madison, WI) following the manufacturer's instructions
for standard protocol. which can detect as little as S O pg protein.
RESULTS
Enzymatic gene amplification with HTLV-I t a d r e x primer
on fresh PBMCs and T cells of SS patients. For the detection of HTLV-I tudrex sequence, DNA was prepared from
fresh PBMCs and cultured T cells and tested for proviral
DNA b y PCR. Amplification was performed using HTLV-I
tudrex specific primer pairs (see Materialsand Methods) and
analyzed by hybridization with a "P-labeled tudrex region
oligonucleotide probe (T- 1-3). In titration experiments with
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
HTLV-I
TAX/R€X
127
-
IN CTCL
2665
I
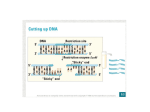
Fig 1. Analysis of PCR-amplified DNA extracted from SS PBMCs. The primers used were specific for HTLV-I tax/rex gene. The HTLV-I tax/
rex-specific oligonucleotide probe used for hybridization was T-1-3 with several concentrations of 13-4 cell line DNA known to be infected
with HTLV-I that served as a positive control. DNA from U937 cell line and MOT cell line (HTLV-II positive) was the negative control. The line
is the location of the expected 127-bp PCR product using these primers.
positive control DNA, we found that the limit of detection
lies between 20 and 200 pg DNA with this primer pair. The
PCR results illustrated in Figs 1 and 2 indicate that I8 (72%)
S S patients' PBMCs of 25 tested were positive for HTLVI radrex DNA, whereas 20 (80%) of 25 T-cell lines from
S S patients were positive for this same region. Only 1 S S
patient's PBMCs (SZ-32) were foundtobe
negative for
HTLV-I radrex gene sequence, whereas the derived T-cell
line was positive. Negative results were obtained with DNA
from the blood of healthy donors (9 PBMCs and I O cord
bloods), confirming the specificity of the amplification (Fig
3).
Enzymatic gene ampl$cation of HTLV-I gag on DNA from
PBMCs and T-cell lines of SSpatienfs. After initial examination with HTLV-I radrex primers, DNA samples derived
frombothPBMCsand
cell lines with S S were amplified
with synthetic oligonucleotides belonging to three different
regions of HTLV-I and HTLV-I1 viral genomes (see Materials and Methods). The primer pairs ((3-1-1 and G-1-2) specific for HTLV-I gag (see Materials and Methods) region
(representing a 535-bp nucleotide base sequence) were used
to amplify DNA from PBMCs and T-cell lines. We could
not detect any significant 535-bp gag product by hybridization with a gag-specific (G-1-3) oligonucleotide probe. However, we can detect between 20 and 200 pg when positive
control DNA was subjected to PCR using these primers. The
primer pairs T- 1,2-1 and T- 1,2-2, which
amplify a conserved
region of tax common to both HTLV-I and -11, were used
to amplify 159 bp. The results were confirmed by repeated
analysis and are summarized in Table I for PBMCs and in
Table 2 for T-cell lines. We found 57% of S S PBMCs (12/
2 1) and 54% of T-cell lines ( 1 3/24) to be positive.In titration
experiments with positive control DNA, we found that the
limit of detection lies between 200 pg and 2 ng. Negative
results obtained using gag and f a x regions of HTLV-I1representing 409- and 3 19-bp nucleotide base sequences, respectively, were screened using specific primer pairs on these
samples. Negative results indicate the absence of HTLV-I1
gag and tar genes. Healthy donors (9 PBMCs and 10 cord
bloods) also tested negatively for HTLV-I rax/rex (observed
Fig 2. Analysis of PCR-amplified DNA extracted from T-cell lines derived from SS PBMCs. The procedures were the same as for Fig 1. N-l,
N-2, and N-4 represent negative controls (DNA from healthy individuals).
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
2666
GHOSH ET AL
-127
Fig 3. Analysis of PCR-amplifiedDNA extracted from control subjects. The primers and probe used were the same as for Fig 1. DNA from
PBMCs of 9 healthy donors (Ph) and l0 cord blood (CB) served ascontrol subject. Different concentrations of DNA from 13-4cell line and MT2 (HTLV-I positive) were used as positive control and MOT (HTLV-II positive) was used as negative control.
in S S patients and lines) as well as for gag I and I1 and tax
I1 (data not shown).
Nucleotide sequence analysis of PCR-amplijied products.
To compare the sequence of tadrex PCR product (DNA
from S S patients' blood andcell lines) with HTLV-Igenome,
we cloned the 127-bp radrex PCR fragment into a plasmid
vector (supplied with the kit, PCR I1 cloning kit; Invitrogen).
EcoRI-digested plasmid was sequenced by dideoxy chain
termination methodsI6 to characterize precisely the type of
retrovirus by nucleotide comparison to the sequences of the
HTLV-I genome. The comparative analysis of the sequence
of tadrex from 4 S S patients (SZ-29 PBMC, SZ-4 cell line,
SZ-28 cell line, and SZ-5 lymph node) to that of prototypic
HTLV-I sequence indicates that the amplified product from
S S patient DNA was identical to the prototype sequence of
HTLV-I (7598 CAA TCA CTC ATA CAA CCC CCA ACA
TTC CAC CCT CCT TCC TCC AGGCCA TGC GCA
AATACTCCC CCTTCC GAA ATG GATACA TGG
AAC CCA CCC TTG GGC AGC ACC TCC CAA CCC
TGT CTT TTC CAG A 7724).
Detection of HTLV-I tadrex mRNA in fresh PBMCs of SS
patients. RNA-PCR was used to examine the expression
of radrex mRNA in fresh PBMCs of S S patients. Total
RNA was extracted from PBMCs and treated with DNase
to eliminate potential DNA contamination. Then RNA (2
pg) was reverse transcribed to cDNA, followed by 40 cycles
of PCR amplification using the HTLV-I radrex-specific
primer pair. To determine the sensitivity of RNA-PCR, RNA
from MT-2 cells were serially diluted (1: IO) and mixed with
carrier totalRNA (2 pg) from normal PBMCs (HTLV-Inegative). A positive signal was detected when as little as
0.2 pg MT-2 mRNA was subjected to PCR, a IO' dilution.
We have detected HTLV-I tadrex RNA in PBMC in 4 of 8
S S patients (Fig 4). PCR was performed without an RT step
using DNase-treated RNA and produced no tadrex-specific
products, confirming that DNA was not contaminating the
RNA preparation (data not shown).
RNA-dependent reverse transcriptase activiv. To detect
retroviral RT activity, we measured the incorporation of ('H)
GTP using synthetic homopolymer templates (Poly IC)and
short oligodeoxy nucleotide primer (oligo dG). T-cellculture
supernatants from 4 S S patients were concentrated by ultracentrifugation and tested for RT activity in presence of Mg2+
along with MT-2 (HTLV-I-positive) culture supernatant as
a positive control. The data presented in Table 3 show that
none of the cultured supernatants has any detectable Mg*+dependent activity, whereas MT-2 supernatants showed a
typical poly IC oligo dG-dependent RT activity of HTLVI.
Western blot analysis of patient serum against HTLVI antigen. Western blotting was performed to determine
whether antibodies reactive with tax (p40)or rex (p27) proteins could be detected in S S serum. UsingMT-2 lysate
proteins separated by SDS-PAGE and transferred to nitrocellulose as described in Materials and Methods, wetested
serum or plasma from the individuals shown in Fig 5 . Sera
from a patient with HAM (13-4) and an HTLV-I ELISApositive patient with cutaneous lymphoma (SZ-37) contained
antibodies reactive with both gag and envproteins of HTLVI as well as with p27"" and p40'". Serum from a healthy
donor served as a negative control (Ph-9). We found that 9
of 21 (43%) and 6 of 21 (29%) of S S patients contained
antibodies reactive withp27"" and p4OIax, respectively, but
not reactive with gag or env proteins. In total, 57% of these
individuals contained antibodies reactive with either of these
proteins.
Detection of taxlrex gene in punch skin biopsies from
patients with MF. To determine whether these observations
could be extended to MF patients, we tested for the HTLVI tadrex gene in DNA extracted directly from skin punch
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
HTLV-I
T A X ~ R E XIN
2667
CTCL
Table 1. Enzymatic Gene Amplification of HTLV-I and -11 DNA
Sequences in PBMCs From SS Patients
gag I
Patients
sz-l
sz-3
sz-5
s z - l0
sz-l2
sz-19
sz-20
sz-22
SZ-23
SZ-24
SZ-25
52-27
SZ-28
SZ-29
SZ-30
SZ-32
sz-33
sz-35
sz-37
SZ-38
sz-39
SZ-40
SZ-41
SZ-42
sz-45
Controls
U937
13-4t (2 pg)
13-4 (20ng)
13-4 (2 ng)
13-4 (200 pg)
13-4 (20 pg)
MOTS 12 pg)
MOT (20ng)
MOT (2 ng)
MOT (200 pg)
gag II
taxl, II*
taxVrexl
+
+
+
+
+
+
+
ND
ND
+
-
-
+
+
-
-
ND
ND
+
+
+
+
+
+
+
+
+
+
+
-
-
+
+
+
+
+
-
-
-
+
-
+
-
+
+
-
-
-
-
ND
+
+
+
+
+
-
-
-
ND
+
~~
ND
ND
ND
ND
ND
ND
~~
taxll
~
Abbreviation: ND, not done.
* Region amplified is conserved between HTLV-I and 4.
t HTLV-l-positive cell line.
HTLV-ll-positive cell line.
*
biopsy specimens from patients with MF. The high molecular weight (genomic) DNA (2 pg) obtained from skin lesion
of 10 MF patients were subjected to PCR amplification with
synthetic oligonucleotide primers specifically chosen to amplify 127-bp HTLV-I t d r e x and 535-bp gag (Materials and
Methods) gene sequences, as described. Positive results were
observed in 3 patients (30%) only when the tdrex-specific
primer pair was used (Fig 6), whereas no 535-bp gag product
was detected (data not shown).
DISCUSSION
We have detected the presence of the HTLV-I t d r e x
gene (but not the gag gene) in DNA from PBMCs and Tcell line(s) from S S patients as well as in skin lesions from
MF patients. The region detected by gene amplification was
found to be identical by double stranded DNA sequencing
to that of prototypic HTLV-I. No evidence of reverse transcriptase activity was found in supernatants from cell lines.
Analysis of serum antibodies to HTLV-I by Western blot
was negative for viral structural proteins, but a proportion
of patients showed reactivity to p27*” and p40’”.
We observed that the t d r e x gene is actively being transcribed by certain S S PBMCs as determined by RNA-PCR.
These data indicate that these genes are being expressed in
vivo, strengthening the possibility that t d r e x expression
plays a role in the etiology of CTCL. However, the level of
expression is less than that necessary for detection by Northem blot analysis. This observation is not surprising because
similar results have been observed inPBMCs of patients
with HTLV-I ATL, showing positive results with RNAPCRI9 without detection by Northern blot.”
Table 2. Enzymatic Gene Amplification of HTLV-I and -11 DNA
Seauences in T-cell Lines Derived From SS PBMCs
Patients
sz-l
sz-2
sz-3
52-4
sz-5
SZ-6
sz-7
SZ-8
sz-10
SZ- 13
sz-20
sz-22
52-23
SZ-24
SZ-25
SZ-26
SZ-27
SZ-28
SZ-29
SZ-30
SZ-31
SZ-32
sz-33
sz-34
sz-35
Controls
Normal 1
Normal 2
Normal 3
Normal 4
Normal 5
U937
13-4t (200 ng)
13-4 (20ng)
13-4 (2 ng)
MOTS (200 ng)
MOT (20 ng)
MOT (2 na)
-
+
+
+
+
+
+
+
+
+
-
+
+
-
+
+
+
+
+
+
+
+
+
-
ND
ND
-
+
+
+
ND
-
Abbreviation: ND, not done.
* Region amplified is conserved between HTLV-I and -11.
t HTLV-l-positive cell line.
S HTLV-ll-positive cell line.
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
GHOSHETAL
2668
1 2 3 4 5 6 7 8 9 10 11
127-
Fig 4. Detection of HTLV-I
taxhex mRNA (DNase treated)
in PBMCs of SS patients by RNAPCR. The primers and probe
used were the same as for Fig
1. Lanes 1 through 8, total RNA
extracted from SS patients SZ-3,
SZ-20. SZ-21, SZ-23, SZ-27. SZ28. SZ-29, SZ-30. respectively;
lanes 9 through 11, MT-2 cell
RNA serially diluted with 2 p g
RNAfrom normal PBMCs (HTLVI negative) and the amount of
MT-2 RNA usedwas 20 pg, 2 pg,
and 0.2 pg, respectively.
--
HTLV-I, the first exogenous human retrovirus,2' was originally isolated from a patient considered to have S S and is
now recognized as the etiological agent of ATL.2'*22The
relationship between CTCL (MF and S S ) and ATL has not
yet been clearly defined, but they share several features, ie,
clonal T-cell transformation, skin involvement, and clinical
similarity of end-stage disease. In contrast, ATL is an aggressive disorder, with rapid progression to death, whereas
CTCL is more indolent. In ATL, HTLV-I provirus is integrated randomly into the abnormal T-cell population and the
vast majority of the patients are seropositive for the structural
proteins of HTLV-L2' In most ATL patients, serologic reactivity with HTLV-I tax protein has also been reported."
The role of HTLV-I in the initiation and clonal expansion
of CTCL is unknown. Manzari et a14 reported the detection
of a new retrovirus, HTLV-V,in Italian MF patients and
Hall et al' found a defective form of HTLV-I proviral DNA
in MF patients. However, at least two reports were unable
Table 3. RNA-Dependent Reverse Transcriptase Activity
Sample
sz-3
sz-3
sz-4
sz-4
SZ-28
SZ-28
sz-35
52-35
MT-2
MT-2
Templateffrimer
(poly rC oligo dG1
+
-
+
-
+
-
+
+
TCA Precipitable
'H-dGTP (cpm)
2,005
1,534
775
624
1,389
1,463
1,045
875
993
11,193
Culture supernatants from SS cell line were concentrated 50x by
ultracentrifugation (25,000 rpm in BeckmanSW28 rotorfor 90 minutes
at 4°C). Reverse transcriptase activity
was quantitated by the incorporation of 13HI-dGTP(specificactivity, 11 Cilmmol;ICNBiomedical)
using a poly(rC)oligo(dG)12-18 (40 pg/mL) template-primer kit (Pharmacia). The reaction mixture contained 45 pmol/L labeled-dGTP as
well as TrisRlCl(50 mmol/L) pH 8.0, MgCll (30 mmol/L), KC1 (40 mmoll
L), Triton x - l 0 0 (0.05%).and dithiothreitol(5 pmol/L). Enzyme activity
Materials and
was assayedat 37°C. during 60 minutes as described in
Methods.
to confirm these observations using DNA from PBMCs and
skin biopsies from patients with CTCL.24.2sNone of these
studies reported testing of T-cell lines established from
CTCL for detection of HTLV-I regions thatcanbeused
to expand the potentially infected malignant cell. We have
observed a stronger PCR signal in certain T-cell lines as
compared with the PBMCs of that patient, suggesting potential expansion of the affected cell.
The proviral genome of HTLV-I contains, in addition to
the structural gene, a unique extra sequence, pX, located
between the env gene and the 3' long terminal repeat
(LTR)?' The pX regionis expressed as doubly spliced
mRNA with tax (p40)and rex (p27) using two overlapping
open reading frames2' thatregulate the replication of HTLVI at the transcriptional and posttranscriptional level, respect i ~ e l y . ~ "Recently,
'~
Pancake and Zucker-Franklin' reported
the presence of r u x gene common to HTLV-I and I1 in DNA
from PBMCs of 6 MF patients, but it was not determined
whether the agent detected was HTLV-I or -11. We have
characterized the tadrex-amplified products by nucleotide
sequence analysis. Results clearly demonstrate 100% homology with prototypic HTLV-Iin at least 4 patients (SZ-29
PBMC, SZ-4 cell line, SZ-28 cell line, and SZ-5 lymph
node). The work presented here demonstrating the association ofa portion of the HTLV-I genome in certain S S patients
blood issimilar to that of Hall et al' and Pancake and ZuckerFranklin' with respect to radrex DNA in CTCL. However,
because of the absence of RT in our experiments, our data
are more consistent the observations of Hall et al? Furthermore, we sent several S S PBMCs DNA samples to an independent laboratory, who confirmed our results (data not
shown). The fact that the observations made here have not
been found universally by all investigators who have performed similar experiments may relate to two important observations. First, titration of the Mgz+is critical for all primer
pairs. In our hands, positive PCR products were best produced with the radrex-specific primers using 0.75 mmol/L
Mgz+. Second, a nonintegrated form of tadrex gene has
been found in the "Hido supernatants" from PBMCs and
cell lines tested here (Ghosh et al, submitted for publication).
The nonintegrated form of radrex gene may represent a
significant portion of the DNA amplified in these individuals.
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
HTLV-I
TMlREX
IN CTCL
2669
30,
p27 -b
21.5
1
2
7
36 5 4
8
9
10 15
14
13
12
11
1624
23
22
21
20
19
18
17
Fig 5. Antibodies to HTLV-I antigen detected in sera from patients with SS by Western blotting. Numbers at left indicate 40- and 27-kD
proteins. Lane1, sera from a patient with TSP (13-4); lane 2, sera from an HTLV-l-positive SS patient (SZ-37); lane 3, sera from healthy donor
(Ph-9); lanes4 through 24, sera from Sezary patients SZ-l, SZ-2, SZ-3. SZ-4. SZ-5. SZ-6, S Z - l . SZ-8, SZ-10. SZ-13, SZ-20. SZ-22, SZ-23, SZ-24,
SZ-25, 52-26. SZ-27. SZ-28, SZ-29, 52-30. SZ-32, and SZ-35, respectively.
Thus, extraction of only high molecular weight DNA rather
than total DNA may reduce of a considerable portion of the
signal we have observed. We believe that these methodologic
points are the key to our consistent results. We suggest that
such episomal radrex DNA are likely to be associated with
a high molecular weight complex such as a retrotransposon."
Why certain patients were found negative for radrex is
unclear. However, the number of atypical cells does not
appear to be the determining factor. For example, patients
SZ-5 and SZ-27 were found to be PCR-positive, but contained less then 30% atypical cells, whereas patient SZ-32
was found to be negative, but contained 70% atypical cells.
Conflicting data between PCR performed with the HTLV-I,
I1 tax, and HTLV-I radrex primers is most likely due to the
fact that we are able to detect lower amounts of viral DNA
with the HTLV-I-specific primers (Table I). Positive results
with SZ-41 PBMCs (Table 1) and SZ-l cell line (Table 2)
for HTLV-I, I1 tax DNA, although negative for HTLV-I t a d
rex DNA, is in contrast to the sensitivity for these primers.
One possibility is that these cells retained the common tax
DNA region while deleting the HTLV-I tadrex-specific region. Positive results for HTLV-I t d r e x andHTLV-I, I1
tax DNA in SZ-32 cell line may be due to expansion of taxcontaining cells from the blood. However, we do not know
why SZ-32 PBMCs were found to be tadrex-negative when
the number of atypical cells should have been sufficient to
provide positive results.
Although Zucker-Franklin et al' observed budding viral
particles in short-term cultures of PBMCs from MF patients,
no RT activity was demonstrated. To our knowledge, the
only example of positive RT activity in CTCL was reported
by Manzari et a1: in which activity was measured by using
poly rA oligo dT and Mg2+and not with poly IC, oligo dG
as template-primer. Because poly rA oligo dT can be used
efficiently by cellular DNA polymerase, whereas poly rC
oligo dG template is used poorly if at all by this enzyme,"2
positive RT results may be due to cellular DNA polymerase
contamination. We are unable to demonstrate the presence
of HTLV-I-specific RT activity (using poly rC oligo dG
as template/primer and Mg2+ as divalent cation) in culture
supernatant of S S cell line, which indicates either absence
of HTLV-I whole virus or a virus with unknown template
specificity or level of enzyme less than the detection limit.
We could not identify any CTCL patient as being HTLVI seropositive by criteria established by the US Department
of Health andHuman Services. However, 57% of CTCL
patients tested were seropositive for the tax or rex regulatory
proteins of HTLV-I. The percentage of antibody-positive
individuals is less than the percentage of tadrex DNA-posi-
control.
but who contained antibodies reactive with the t d r e x gene
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
2670
GHOSH ET A L
Table 4. Summary of PCR and Antibodv Pattern for HTLV-I
~~
taxllrexl
______
Western Blot
Lane
Sample
PBMCs
T-cell Line
P27 rex
P40 tax
1
2
3
4
5
6
7
13-4
sz-37
Ph-9
+
+
+
+
+
+
+
sz-l
+
sz-2
sz-3
sz-4
sz-5
SZ-6
sz-7
SZ-8
sz-l0
SZ-13
sz-20
sz-22
SZ-23
SZ-24
SZ-25
SZ-26
SZ-27
SZ-29
SZ-30
SZ-32
sz-35
NA
a
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
-
+
NA
+
NA
NA
-
MF patients, while not observing gag. Alternatively, these
sequences could be associated with an exogenous retrovirus
different from HTLV-I in the gag region; however. such a
virus should have reverse transcriptase activity. Whether tux/
rex is associated with endogenous or exogenous sequences,
we postulate that the expression of t d r e x maintains the
malignant phenotype in CTCL.
ACKNOWLEDGMENT
+
+
We thank Joyce Stohler and Ryan Vestal for excellent technical
assistance.
NA
NA
NA
+
t
+
NA
+
+
+
NA
+
+
+
-
+
+
+/-
Abbreviation: NA, not available
product (Table 4). Interestingly, we noted that all the CTCL
patients were negative for both HTLV-I gag DNA and antibodies reactive with gag gene-encoded proteins p19 and p24,
an observation confirming that these individuals were not
exposed to HTLV-I gag proteins. Conversely, morethan
halfof these patients have developed antibodies reactive
with t d r e x proteins, suggesting that at some point in time
that these t d r e x containing genes have been expressed as
proteins in vivo.
Both of the pX-encoded products (tax and rex proteins)
have an important role in neoplastic T-cell activation. The
p40tar protein functions as a transcriptional activator for its
own promotor as well as several other genes such as IL-2,
IL-2R, c-fos,
The protein p27 rex is required for
cytoplasmic expression of incompletely spliced viral
mRNAs that encode structural proteins. Rex activity is mediated by cis-acting RNA signal sequence, which is bound
specifically by rex protein.36Rex also stabilizes mRNA of
the IL-2Ra chain.37It has been established that pX ( t d r e x )
gene of HTLV-I is capable and sufficient for immortalization
of primary human CD4+ cord blood lymphocytes in culture
in absence of HTLV-I structural genes.38We suggest that
expression of the t d r e x region may be responsible for the
maintenance of the malignant state in CTCL, as was suggested for patients with ATL.39Whether the origin of the
tadrex genes is from a exogenous or endogenous source is
not clear. If these sequences were introduced via prototypic
HTLV-I infection, then the deletion must have occured before the diagnosis of MF was made, because we detected
HTLV-I t d r e x gene in 30% (3/10) of skin biopsies from
REFERENCES
l . Edelson RL: Cutaneous T-cell lymphomas: Perspectives. Ann
Intern Med 83:548, 1975
2. Kuzel TM, Roenigk HH Jr. Rosen ST: Mycosis fungoides
and the SCzary syndrome: A review of pathogenesis, diagnosis and
therapy. J Clin Oncol 9: 1298, 1991
3 . Abrams JT, Lessin S, Ghosh SK, Ju W, Vonderheid EC, Nowell P, Murphy G, Elfenbein B, DeFreitas E: A clonal CM-positive
T-cell line established from the blood of a patient with Sdzary syndrome. J Invest Dermatol 96:31, 1991
4. Manzari V, Gismondi A, Barillari G, Morrone S, Modesti A,
Albonici L, DeMarchis L, Fazio V, Gradilone A, Zani M, Frati L,
Santoni A: HTLV-V: A new human retrovirus isolated in a tacnegative T-cell lymphomdleukemia. Science 238: 158I , 1987
5. Hall W, Liu CR, Schneewind 0, Takahashi H, Kaplan MH.
Roupe G, Vahlne A: Deleted HTLV-I provirus in blood and cutaneous lesions of patient with mycosis fungoides. Science 253:317,
1991
6. Zucker-Franklin D, Coutavas EE, Rush MG, Zou Zias DC:
Detection of human T-lymphotropic virus-like particles in cultures of
peripheral blood lymphocytes from patients with mycosis fungoides.
Proc Natl Acad Sci USA 88:7630, 1991
7. Zucker-Franklin D, Hooper WC, Evatt BL: Human lymphotropic retroviruses associated with mycosis fungoides: Evidence that
human T-cell lymphotropic virus type I1(HTLV-11) as well as
HTLV-I may play a role in the disease. Blood 80: 1537, 1992
8. Pancake BA, Zucker-Franklin D: HTLV tax and mycosis fungoides. N Engl J Med 329:580, 1993
9. Lange-Wantzin G , Thomsen K, Nissen NI, Saxinger D, Gallo
RC: Occurrance of human T-cell lymphotropic virus (type I) antibodies in cutaneous T cell lymphoma. J AmAcad Dermatol 15598,
1986
10. Saxinger WC, Lange-Wantzin GL, Thomsen K, Hoh M, Gallo
RC: Occurrance of HTLV-I antibodies in Danish patient with cutaneous T-cell lymphoma. Scand J Haematol 34:455, 1985
1 1. Abrams JT, Lessin SR. Ghosh SK, Nowell PC, Ju W, Vonderheid EC, Rook AH, DeFreitas E: Malignant and non malignant T
cell lines from human T cell lymphotropic virus type I-negative
patient with SBzary syndrome. J Immunol 146:1455, 1991
12. Abbott MA, Poiesz BJ, Byrne BC, Kwok S, Sninsky JJ, Ehrlich GD: Enzymatic gene amplification: Qualitative and quantitative
methods for detective proviral DNA amplified in vitro. J Infect Dis
158:1158, 1988
13. Saiki RK, Scharf S, Faloona F, Mullis KB, Horn GT, Erlich
HA, Arnheim N: Enzymatic amplification of beta-globin genomic
sequences on restriction site analysis for diagnosis of sickle cell
anemia. Science 230: 1350, 1985
14. Chomczynski P, Sacchi N: Single step method of RNA isolation by acid guanidium thiocyanate-phenol-chlroformextraction.
Anal Biochem 162:156, 1987
15. Wang AM, Dogle MV, Mark DF: Quantitation of mRNA by
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
HTLV-1
T A X ~ R E XIN
CTCL
the polymerase chain reaction. Proc Natl Acad Sci USA 86:9717,
1989
16. Sanger F, Nicklen S, Coulsen AR: DNA sequencing with
chain-terminating inhibitors. Proc Natl Acad Sci USA 745463, 1977
17. Verma IM: Studies on reverse transcriptase of RNA tumor
viruses. 111. Properties of purified Moloney murine leukemia virus
DNA polymerase and associated RNase H. J Virol 152343, 1975
18. Okayama A, Chen YA, Tachibana N, Shioiri S, Lee T, Tsuda
K, Essex M: High incidence of antibodies to HTLV-I tax in blood
relatives of adult T cell leukemia patients. J Infect Dis 163:47, 1991
19. Kinoshita T, Shimoyama M, Tobinai K, Ito M, Ito S-I, Ikeda
S, Tajima K, Shimotohno K, Sugimura T: Detection of mRNA for
the tax'hex' gene of human T-cell leukemia virustype I in fresh
peripheral blood mononuclear cells of adult T-cell leukemia patients
and viral carrier by using the polymerase chain reaction. Proc Natl
Acad Sci USA 865620, 1989
20. Franchini G, Wong-Staal F, Gallo RC: Human T-cell leukemia virus (HTLV-1) transcripts in fresh and cultured cells of patients
with adult T-cell leukemia. Proc Natl Acad Sci USA 81:6207, 1984
21. Yoshida M, Miyoshi I, Hinuma Y: Isolation and characterization of retrovirus from cell lines of human adult T-cell leukemia and
its implication inthe disease. Proc Natl Acad Sci USA 79:2031,
1982
22. Poiesz BJ, Ruscetti W ,Gazdar AF,Bunn PA, Minna JD,
Gallo RC: Detection and isolation of type C retrovirus particles from
fresh and cultured lymphocytes of a patient with cutaneous T-cell
lymphoma. Proc Natl Acad Sci USA 77:7415, 1980
23. Yoshida M, Seiki M, Yamaguchi Y, Takatsuki K: Monoclonal
integration of HTLV in all primary tumors of adult T-cell leukemia
suggests causative role of HTLV in the disease: Proc Natl Acad Sci
USA 81:2534, 1984
24. Capesius C, Saal F, Macro E, Bazarbachi A, Lasneret J, Laroche L, Gessain A, Hozman F, Penes J: No evidence for HTLV-I
infection in 24 cases of French and Portuguese mycosis fungoides
and SCzary syndrome (as seen in France). Leukemia 5:416, 1991
25. Lisby G, Reitz MS Jr. Vejlsgaard GL: No detection of HTLVI DNA in punch skin biopsies from patient with cutaneous T-cell
lymphoma by the polymerase chain reaction. J Invest Dermatol
98:417, 1992
26. Seiki M, Hattori S, Hirayama Y , Yoshida M:Human adult
T-cell leukemia virus: Complete nucleotide sequence of the previous
genome integrated in leukemia cell DNA, Proc Natl Acad Sci USA
80:3618, 1983
27. Seiki M, Hikikoshi A, Taniguchi T, Yoshida M: Expression
267 1
ofthe pX gene of HTLV-I: General splicing mechanism in the
HTLV family. Science 228:1532, 1985
28. Chen ISY, Cann A J , Shah NP, Gaynor RB: Functional relationship of HTLV-I X and adenovirus EIA proteins in transcriptional
activation. Science 230:570, 1985
29. Inoue J, Yoshida M, Seiki M: Transcriptional (P40x) and
post-transcriptional (P 27x-111) regulation are required for the expression and replication of human T-cell leukemia virus type I genes.
h o c Natl Acad Sci USA 84:3653, 1987
30. Bemhard H: Selective extraction of polyoma DNA from infected mouse cell culture. J Mol Biol 26:365, 1967
31. Baltimore D: Retroviruses and retrotransposons: The role of
reverse transcriptase in shaping the eukaryotic genome. Cell 40:481,
1985
32. Chandra P, Steel L: Purification, biochemical characterization
and serological analysis of cellular deoxyribonucleic acid polymerases and a reverse transcriptase from spleen of a patient with myelofibrotic syndrome. Biochem J 167513, 1977
33. Maruyama M, Shibuya H, Harada H, Hatakeyama M, Seiki
M, Fujita T, Inoue J, Yoshida M, Tanaguchi T: Evidence for aberrant
activation of the interleukin-2 autocrine loop by HTLV-I encoded
p40x and T3Ri complex triggering. Cell 48:343, 1987
34. Cross SL, Feinberg MB, Wolf JB, Holbrook NI, Wong-Staal
F, Leonard WJ: Regulation of the humaninterleukin-2 receptor alpha
chain promoter: Activation of a nonfunctional promoter by the transactivator gene of HTLV-I. Cell 49:41, 1987
35. Nagata K, Ohtani K, Nakamura M, Sagamura K: Activation
of endogeneous c-fos protooncogene expression by human T cell
leukemia virus type-I encoded p40tax protein in the human T cell
line, Jurkat. J Virol 63:3220, 1989
36. Grassman R, Berchtold S, Aepinus C, Ballaun C, Boehnlein
E, Fleckenstein B: In vitro binding of human T-cell leukemia virus
type rex proteins to the rex-response element of viral transcripts. J
Virol 65:3721, 1991
37. Kanamori H, Suzuki N, Siomi H, Nosaka T, Sato A, Sabe H,
Hatanaka M, Honjo T HTLV-I p27rex stabilizes human interleukin2 receptor alpha-chain mRNA. EMBO J 9:4161, 1990
38. Grassman R, Berchtold S, Radant I, Alt M, Fleckenstein B,
Sodroski JG, Haseltine WA, Ramstedt V: Role of human T-cell
leukemia virus type I X region proteins in immortalization of primary
human lymphocytes in culture. J Virol 66:4570, 1992
39. Korber B, Okayama A, Donnelly R, Tachibana N, Essex M:
Polymerase chain reaction analysis of defective human T-cell leukemia virus type I proviral genomes in leukemic cells of patients with
adult T-cell leukemia. J Virol 655471, 1991
From www.bloodjournal.org by guest on June 14, 2017. For personal use only.
1994 84: 2663-2671
Human T-cell leukemia virus type I tax/rex DNA and RNA in
cutaneous T- cell lymphoma
SK Ghosh, JT Abrams, H Terunuma, EC Vonderheid and E DeFreitas
Updated information and services can be found at:
http://www.bloodjournal.org/content/84/8/2663.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.