Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Special needs dentistry wikipedia , lookup
Medical ethics wikipedia , lookup
Dental emergency wikipedia , lookup
Electronic prescribing wikipedia , lookup
Prenatal testing wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Patient safety wikipedia , lookup
Infection control wikipedia , lookup
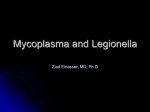
Case Challenge: Dermatology A 13-Year-Old Boy with Pharyngitis, Oral Ulcers, and Dehydration Leanne W. Trapp, MD; Steven J. Schrantz, MD; Monica A. Joseph-Griffin, MD; Joseph R. Hageman, MD; and Shoshana E. Waskow, MD A 13-year-old boy with no significant past medical history was admitted to our institution with pharyngitis, oral ulcers, and dehydration. He was well until 8 days prior to admission when he developed a fever to 103o F and pharyngitis. He was seen by his primary care physician, who orLeanne W. Trapp, MD, is a Resident in Pediat- rics, Comer Children’s Hospital, Pritzker School dered a rapid strep test and throat culture, both of which were negative, so symptomatic care was recommended. Four days prior to admission the patient developed ulcers on the inside of his mouth and lips. He was seen again by his primary care physician and started on antiviral medication and ibuprofen with hydrocodone, and a herpes simplex virus–polymerase chain reaction test was ordered. Mouth pain became so severe that the patient was unable to remain adequately hydrated. He was admitted to the hospital for pain control, intravenous fluids, and further work-up. In the 2 days prior to presentation to the hospital, he developed painful lesions on the glans of his penis. Recent medication use included NyQuil (Vicks), Theraflu (Novartis), Famvir (Novartis) and Vicoprofen (Abbott). The patient denied any history of sexual activity or of Medicine, University of Chicago. Steven J. Schrantz, MD, Department of Medicine, Division of Infectious Diseases NorthShore University HealthSystem; and Clinical Assistant Professor, University of Chicago Pritzker School of Medicine. Monica A. Joseph-Griffin, MD, is Clinical Assistant Professor, Department of Pediatrics, NorthShore University HealthSystem; and Clinical Assistant All images courtesy of Leanne W. Trapp, MD. Professor, Pritzker School of Medicine, University of Chicago. Joseph R. Hageman, MD, is Emeritus Attending Physician, Department of Pediatrics, NorthShore University HealthSystem; and Senior Clinician Educator, Pritzker School of Medicine, University of Chicago. Shoshana E. Waskow, MD, is an independent practitioner, Pediatric Associates of the NorthShore. Figure 1. Cracked, scabbed lips with ulcerations. Address correspondence to: Leanne W. Trapp, MD, Comer Children’s Hospital, 5721 S. Maryland Avenue, Chicago, IL 60637; fax: 773-834-0748; email: [email protected]. Disclosure: The authors have no relevant financial relationships to disclose. doi: 10.3928/00904481-20130326-06 148 | Healio.com/Pediatrics For diagnosis, see page 149 Editor’s note: Each month, this department features a discussion of an unusual diagnosis in genetics, radiology, or dermatology. A description and images are presented, followed by the diagnosis and an explanation of how the diagnosis was determined. As always, your comments are welcome via email at [email protected]. PEDIATRIC ANNALS 42:4 | APRIL 2013 Case Challenge oral sex. Review of systems was positive for a mild, nonproductive cough 1 week prior to admission, but negative for rhinorrhea, vomiting, diarrhea, shortness of breath, chest pain, arthralgia/joint pain, change in vision, headaches, dysuria, or frequency; fevers had resolved 4 days prior to admission. PHYSICAL EXAMINATION On admission, the patient appeared tired and mildly dehydrated. He was afebrile with a pulse of 107 beats per minute, blood pressure of 118/52 mm Hg, and respiratory rate of 20 breaths per minute. His conjunctivae were mildly injected bilaterally. Lips were scabbed with dried blood present (see Figure 1, page 148). Buccal mucosa and gums were erythematous with multiple erosive lesions and white plaques (see Figure 2). Tonsils were enlarged 3+ bilaterally, and erythematous with exudates present. The cardiac examination revealed normal rate and rhythm with no murmur. The lungs were clear to auscultation bilaterally with no wheezing or crackles present. Head of penis was erythematous with vesicles present and scab formation at the urethral meatus (see Figure 3). No other rashes were noted on his skin. HOSPITAL COURSE The patient was given an intravenous (IV) normal saline bolus in the emergency department and 1 dose of dexamethasone IV (0.6 mg/kg). He was admitted to the general pediatrics floor and started on maintenance IV fluids and IV pain medication. The herpes simplex virus–polymerase chain reaction (HSV-PCR) test of an oral lesion done at his pediatrician’s office was negative for HSV 1 and 2, and the antiviral medication was discontinued. He was continued on IV solumedrol for 2 days but it was discontinued after no improvement in symptoms was noted. Initial laboratory work-up included PEDIATRIC ANNALS 42:4 | APRIL 2013 Figure 2. Cracked, scabbed lips with ulcerations and erythematous tongue with ulcerations. serum electrolytes, blood urea nitrogen, creatinine, liver function tests, complete blood count with differential, mono-spot test, urinalysis, and urine culture, all of which were normal. C-reactive protein was elevated at 64.2 mg/L and erythrocyte sedimentation rate was 35 mm/ hour. On day 2 of hospitalization, the patient developed lesions in his nares bilaterally and crusting of lower eyelids bilaterally with continued conjunctival injection. He was also noted to have scattered vesicular lesions on his scrotum but no rash anywhere else. Further work-up included Epstein-Barr virus and cytomegalovirus titers, HLA-B27, and HIV antibody, all of which were negative. Cold agglutinin test was performed on hospital day 2 and was negative. He was started on a 5-day course of azithromycin for possible Mycoplasma pneumoniae infection while awaiting the results of Mycoplasma antibody tests. Ophthalmology was consulted due to lesions in the eye and work-up was negative for corneal or lens involvement. Mucositis slowly began to improve over course of hospitalization. On hospital day 4, Mycoplasma immunoglobulin M (IgM) was reported to be positive and the patient was diagnosed with Mycoplasma pneumoniae-associated mucositis. Figure 3. Erythematous head of penis with crusting. Diagnosis: Mycoplasma pneumoniaeAssociated Mucositis DISCUSSION Mycoplasma pneumoniae is a freeliving organism that lacks a cell wall. It most commonly causes communityacquired atypical pneumonia in children. The most common symptoms are nonproductive cough, myalgias, sore throat, headache, and dyspnea. Though less common, Mycoplasma pneumoniae infection has been associated with several extrapulmonary manifestations including neurologic complications such as aseptic meningitis or encephalitis, cardiac complications such as pericarditis or myocarditis, renal complications such as glomerulonephritis or acute renal failure, and hematologic complications such as hemolysis.1 Mycoplasma pneumoniae is also a rare but well-known cause of Stevens– Johnson syndrome (SJS). SJS occurs in 1% to 5% of cases of Mycoplasma pneumoniae infection.1 According to the classification by Bastuji-Garin and colleagues,2 SJS is characterized by extensive erosion of the skin with poorly defined circular lesions and often with Healio.com/Pediatrics | 149 Case Challenge at least one mucosal surface involved.2 Less than 10% of the body surface area is involved in epidermal detachment. Other classifications suggest that at least two mucous membrane surfaces should be involved.3 There have been several case reports in which Mycoplasma infection is localized to the mucous membranes with very little to no skin involvement.4-6 Patients will often have ocular, oral, and genital involvement as in our patient. This was previously known as atypical SJS but it has been suggested that the term Mycoplasma pneumoniaeassociated mucositis would be a more appropriate definition.1 This is because patients with only mucous membrane involvement recover faster than those patients with SJS, and they do not have the higher risk of mortality seen in SJS.1 Skin involvement is also a key criterion in the diagnosis of SJS. The etiology of Mycoplasma pneumoniae-associated mucositis is unknown but it has been suggested that an antibody may be directed against a specific mucous membrane antigen, causing the clinical sequelae that are seen.4 The diagnosis is often made by detection of Mycoplasma pneumoniae IgM and patients are often treated with macrolide antibiotics. In all the case reports reviewed, the mucositis was severe enough to require hospitalization. The use of corticosteroids is controversial, as it is in the treatment of SJS due to the concern of predisposing the patient to further infection. Most of the patients recovered with the use of antibiotics alone, without the use of corti- 150 | Healio.com/Pediatrics costeroids and without any major lasting sequelae. In the few cases that were refractory to antibiotic treatment and supportive care, intravenous immunoglobulin provided rapid improvement in the mucositis.7-9 CONCLUSIONS The case presented represents a rare but clinically significant manifestation of Mycoplasma pneumoniae infection. In children, Mycoplasma pneumoniae is one of the most common causes of SJS, but it is important to consider this organism in mucous membrane-limited disease as well. It is also important to distinguish between Mycoplasma pneumoniae-associated mucositis and SJS, as the long-term sequelae and mortality rate differ greatly. Patients who present with mucous membranelimited disease, however, should be monitored closely for the progression to skin involvement and SJS. Our patient was discharged home on hospital day 5 with resolving mucositis. He was able to tolerate oral fluids and was to complete a 5-day course of azithromycin. This patient’s recovery proceeded slowly. After discharge, he continued to require significant pain medication for both oral and penile pain and local care for the penile lesions. Given his slow improvement, he received a second 5-day course of azithromycin (initiated 10 days after the first course). He returned to school approximately 3 weeks after his initial presentation to the pediatrician’s office (about 12 days after hospital discharge). At that point, he had minimal remnants of the oral and penile ulcerations and required no pain medications. He experienced a total weight loss of 20 pounds (15% of pre-illness body weight) that he slowly regained over the month after his return to full activity. REFERENCES 1. Schalock PC, Dinulos JG. Mycoplasma pneumoniae-induced cutaneous disease. Int J Dermatol. 2009;48(7):673-680. 2. Bastuji-Garin S, Rzany B, Stern RS, Shear NH, Naldi L, Roujeau JC. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme. Arch Dermatol. 1993;129(1):9296. 3. Huff JC, Weston WL, Tonnesen MG. Erythema multiforme: a critical review of characteristics, diagnostic criteria and causes. J Am Acad Dermatol. 1983;8(6):763-775. 4. Schalock PA, Dinulos JGD, Pace N, Schwarzenberger K, Wenger JK. Erythema multiforme due to Mycoplasma pneumoniae infection in two children. Pediatr Dermatol. 2006;23(60:546-555. 5. Figueira-Coelho J, Lourenco S, Pires AC, Mendcona P, Malhado JA. Mycoplasma pneumoniae- associated mucositis with minimal skin manifestations. Am J Clin Dermatol. 2008;9(6):399-403. 6. Ravin KA, Rappaport LD, Zuckerbraun NS, Wadowsky RM, Wald ER, Michaels MM. Mycoplasma pneumoniae and atypical Stevens-Johnson Syndrome: a case series. Pediatrics. 2007;119(4):e1002-1005. 7. Bressan S, Mion T, Andreola B, Bisogna G, Da Dalt L. Mycoplasma pneumonia-associated mucositis treated with immunoglobulins. Acta Paediatrica. 2011;100(11):e238-240. 8. Zipitis CS, Thalange N. Intravenous immunoglobulins for the management of StevensJohnson syndrome with minimal skin manifestations. Eur J Pediatr. 2007;166(6):585-588. 9. Birch J, Chamlin S, Duerst R, Jacobsohn D. Mycoplasma pneumonia and atypical Stevens-Johnson Syndrome in a hematopoietic stem cell transplant recipient. Pediatr Blood Cancer. 2008;50(6):1278-1279. PEDIATRIC ANNALS 42:4 | APRIL 2013