Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
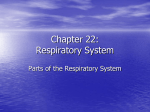
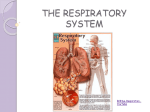
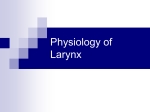
Angela Kempen October Case Study October 29, 2012 3D Conformal Radiation Therapy for Squamous Cell Carcinoma of the Vocal Cords History of Present Illness: RW is a 77 year-old male who presents with a long history of having a very hoarse voice. He has had previous direct laryngoscopy and biopsies which showed dysplasia. He was seen by a physician in May and he was noted to have abnormal vocal cords. He was recommended to have a direct laryngoscopy, but this procedure was postponed as a result of developing bilateral pulmonary emboli. He was seen back by the same physician earlier in the month of October and a direct laryngoscopy was done on 10/5/2012. The results of the procedure revealed bilaterally abnormal vocal cords involving the vocal process to the commissure. The cords have normal mobility. A biopsy revealed squamous cell carcinoma. The patient was referred to Radiation Oncology for the consideration of radiation therapy. Past Medical History: The patient suffers from severe chronic obstructive pulmonary disease (COPD) and hypertension. He has dyslipidemia. In 2001, he experienced a myocardial infarction (MI) and had a stent placed to circumflex the artery. The patient also suffered from a transient ischemic attack (TIA), and was diagnosed with a pulmonary embolism (PE) in June of 2012. In addition, the patient has coronary artery disease. Diagnostic Imaging Studies: The patient underwent a computed tomography (CT) scan of his neck on 10/19/2012. The scan revealed exophytic tissue coming off the mid left true vocal cord all the way through the anterior commissure and extending into the right true vocal cord to midlevel. There is also some extra soft tissue density in the region of the anterior commissure along with some minimal thickening of the adjacent aspects of the right and left true vocal cords. The patient also had a flexible fiberoptic laryngoscopy done. The nasopharynx, oropharynx, hypopharynx and larynx were examined. The findings showed bilaterally abnormal cords with irregular heaped up tissue from the vocal process to the commissure. Mobility was normal. He was staged as clinical stage I (T1b, N0, M0) early stage glottic larynx cancer, by American Joint Committee on Cancer (AJCC). Family History: The patient has a significant family history of cancer. Both his mother and father died of cancer. Both of his brothers died of prostate cancer, one of his sisters died of lung cancer and another sister died of breast cancer. He has a sister who is still alive, but living with mantle cell lymphoma. Social History: The patient is married and resides with his wife. They have three children. The patient is a former pipe smoker of one pack per day for 40 years. He quit in 1987. He has approximately two drinks a day. Medications: The patient uses the following medications: Advair, albuterol, aspirin, Nitrotab, palmetto fruit, senna, simvastatin, tiotropium, and warfarin. Recommendations: The Radiation Oncologist recommended that the patient receive radiation therapy for management of his early stage larynx cancer. This would be localized radiation therapy to the larynx with no coverage of the lymph node region. The physician discussed the rationale for radiation therapy with the patient. Toxicities during treatment were reviewed which include, but are not limited to, fatigue, skin irritation, dysphagia, odynophagia, and hoarseness. In addition, potential for late effects from treatment including thyroid cartilage necrosis and injury to the soft tissues of the neck were discussed. The patient was in agreement to proceed. The Plan (Prescription): The plan is for the patient to receive 6525 centigray (cGy) to the larynx planning treatment volume (PTV) using a 3D-conformal technique. Patient Setup/Immobilization: The patient was simulated in the supine position, with an aquaplast mask used for immobilization of his head, neck and upper shoulder region. Arm pulls were used in an attempt to move his shoulders as far down and away from his neck as possible. A treatment planning computed tomography (TPCT) was completed with 2.5 millimeter (mm) slices through the head and neck region. Anatomical Contouring: The physician drew the gross tumor volume (GTV), clinical tumor volume (CTV) and the larynx PTV. I contoured the spinal cord, right carotid and left carotid. Beam Isocenter/Arrangement: I placed the isocenter in the middle of the larynx PTV. I then added two lateral beams of 6 megavoltage (MV) photon energies. The straight lateral beams were going through the patients shoulders, so I changed the right lateral to a right anterior oblique (RAO) at 285 degrees with a collimator rotation of 340 degrees, and changed the left lateral to a left anterior oblique (LAO) at 75 degrees with a collimator rotation of 20 degrees. The physician then set his field size. Treatment Planning: The physician wanted to the larynx PTV to receive 6525 cGy in 29 fractions at 225 cGy per fraction. The spinal cord was to be kept as low as reasonably achievable. I calculated the beams and added 45 degree wedges with the heels facing anterior to both the LAO and RAO beams to decrease hot spots. I still had a large hot spot superiorly, so I copied the LAO field and added a 30 wedge with the heel facing superior to decrease the hot spot. To cool the plan down even more, I copied the RAO field and closed some of the multicollimator leaves (MLC). I then weighted the beams to even out the prescription dose and make the plan more conformal. The fields, wedge orientation and weighting of each beam can be seen in Figure 1. I struggled to achieve 95% of the larynx PTV receiving full prescription dose, since the fields were drawn so tight with very little margin. The physician was ok with this, but wanted a bit more coverage anteriorly since that was were gross disease was located. A 4x3 centimeter (cm) piece of 0.5 cm bolus was added to increase dose in this area. The physician prescribed to the 100% isodose line and approved the plan. Figure 1: Field size, wedge orientation and beam weighting Figure 2: Axial, sagittal and coronal slices Figure 3: Axial slices showing isodose lines Monitor Unit Check: Monitor unit (MU) calculations were performed to verify that the treatment planning computer was calculating properly. MU check by Oncology Data Systems, version 8.2.0, takes several factors into consideration in order to perform an accurate calculation to determine the monitor units needed for treatment. The MU result is compared to the computer MU calculation. The difference between the two should result in less than 5%, which it did for this plan. Quality Assurance Check: A physicist performed a second check of the treatment plan and monitor unit check. It is critical to have an independent set of eyes look over the plan and additional checks. Conclusion: I chose this case study because it was challenging. The patient had a very short neck and was unable to move his shoulders out of the treatment fields. Therefore, oblique treatment fields were used. The physician drew his fields very tight with little margin around the larynx PTV, which made it difficult to obtain adequate coverage of the larynx PTV. After having a discussion with the physician, it was determined that eliminating hot spots and adding the bolus to ensure the prescription dose adequately covered the gross disease was more important than 95% of the larynx PTV receiving full prescription dose. I learned that a discussion with the physician regarding exactly what he wants is extremely important in treatment planning. Figure 4: Dose Volume Histogram (DVH)