Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
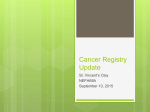
Quality Reporting Now and in the Future Heather Smith, PT, MPH Mandy Frohlich Future of High Quality Patient Care Future of Medicare Part B Quality Reporting DOPTA PQRS FLR Future reporting systems PTPCS SGR PAC Congressional Medicare Payment Reform What is the Sustainable Growth Rate (SGR)? • Created in the Balanced Budget Act of 1997 • Payment formula for all outpatient Medicare services • Intended to ensure that yearly increases match the growth in GDP • Flawed formula results in the need for a yearly “doc fix” Congressional Medicare Payment Reform What will the SGR be replaced with? • 5% annual updates through 2018 • Incentive payments starting in 2018 through Merit- Based Incentive Payment System (MIPS) • Alternative to MIPS is participation in Alternative Payment Models It’s Not Just SGR Functional Limitation Reporting as Part of Therapy Cap Reform • FLR will be reformed and expanded to include additional variable as identified by the Secretary and stakeholders in 2017 (demographic info, diagnosis, severity, affected body structures/functions, limitations with ADLs and participation, functional status, etc) • Data to be submitted via web-portal or other mechanism • Data utilized to report to Congress on new payment system It’s Not Just SGR Post-Acute Care Reform • IMPACT Act Discussion Draft • Requires standardized patient assessment data • Reports to Congress based on comparing patient outcome data to reform payment • Interest in going to bundles, site neutral payment in the future • Protecting Access to Medicare Act of 2014 (H.R. 4302) • Establishment of a new Value Based Purchasing (VBP) program for Skilled Nursing Facilities (SNF) based on performance on hospital readmission measures beginning in 2019. This new program would provide $2 billion in savings. Quality Reporting Today Future Separate and distinct reporting programs (FLR, PQRS, MU, etc.) One quality program under Medicare Part B Varied methods of data reporting Electronic reporting via patient registries High percentage of process measures Focus on outcome measures and patient/family centered measures Multiple measures of patient function One measure of global patient function that crosses the continuum of care Identification of measure gaps by government/ national measurement groups Increasing role of associations in the creation of meaningful quality measures for professionals 10 Physical Therapy Outcome Registry EHR’s EMR’s Billing vendors Components PT Outcome Registry Facility based practices Health systems Private practice clinics 11 Registry: Meeting Compliance Needs PQRS Future Programs FLR 12 Registry 2014 and Beyond Minimum data set • Core data elements • PQRS • FLR Modules • Based on CPGs • Tied to quality measures Future evolutions • Changing policy/ payment • Potential partnerships Current Quality Reporting Programs Under Medicare Healthcare Setting Quality Program(s) Inpatient (Acute Care Hospitals) IQR, Readmissions & VBP Yes Yes P4R & P4P in 2013 Long Term Care Hospitals (LTCH) Beginning in 2014 Yes Yes P4R Penalty 2% Inpatient Rehabilitation Facilities (IRF) Beginning in 2014 Yes Yes P4R Penalty 2% Skilled Nursing Facilities (SNF) MDS 3.0 Yes No Beginning in 2014 Yes Yes P4R Penalty2% OASIS, HH CAHPS Yes Yes P4R Penalty 2% PQRS No, payment adjustments for nonparticipation beginning in 2015 (based on 2013 data) Yes P4R Incentive 0.5% through 2014, 1.5% 2015, -2.0% 2016 and beyond Accountable Care Organizations ACO program (ACO) Yes P4P data performance tied to shared savings Functional Limitation Reporting (FLR) Yes Non-compliance = claims returned unpaid Hospice Home Health Outpatient Therapy services provided under Part B Mandatory Reporting Payment Incentive/ Penalty PQRS vs Functional Limitation Reporting Program Detail PQRS Functional Limitation Reporting Program start date •2007 (incentive program) •2015 (penalty program) •January 1, 2013 •July 1, 2013 (non-payment) Participants (Medicare Part B) •Eligible professionals (including PT, OT, SLP) billing for outpatient physical therapy services in private practice settings •Facility based outpatient practices are not able to participate •All practice settings that provide outpatient therapy services (PT, OT, and SLP) furnished in all outpatient settings including facilities Reporting method •Claims •Registry •Claims Reporting frequency •Determined by CPT codes submitted (Example: 97001, 97002 , 97110, 97140, 97532, several wound care codes) •Determined by visit (evaluation, minimum of every 10th visit, reevaluation, discharge) Tracking of data •NPI (provider) •Beneficiary, NPI/ Tax ID facility, Service provided (PT, OT, SLP) Information reported •Quality Data Code (QDC) G-code •QDC modifier (1P, 8P) •Functional limitation G-code •Therapy modifier •Severity modifier PQRS Reporting and Payment PQRS Program Reporting Year Data Year Utilized to Inform Payment Incentive/ Penalty Payment 2013 2013 +0.5% 2014 2014 +0.5% 2015 2013 -1.5% 2016 2014 -2.0% 2017 2015 -2.0% PQRS Eligible Providers • In 2014, eligible providers who bill under the physician fee schedule (includes PTs in private practice) can receive a bonus payment of 0.5% if they report on quality measures • Rehab agencies, outpatient hospitals, SNFs Part B unable to participate in PQRS; use UB-92 (UB-04) or 837I for billing to intermediary • No place on claim form for individual NPI PQRS • Major changes to the reporting system for 2014 • 2 successful reporting thresholds established: • Eligible for 0.5% 2014 bonus AND avoid -2.0% 2016 penalty • Avoid the -2.0% 2016 penalty ONLY • Can choose not to participate and take the -2.0% 2016 penalty • Major changes to available measures, reporting mechanisms for measures, and measure details Should I participate in PQRS in 2014 ? Yes- I want qualify for the bonus and avoid the penalty Report via claims Report all available individual measures (6 or 7*) Select 9 individual measures (or if less available 1-8) Report via registry Report one measures group Report via claims Yes – I want to avoid the penalty Select 3 individual measures Select 3 individual measures Report via registry No – I will take the 2.0% penalty in 2016 Report one measures group Should I participate in PQRS in 2014 ? Report via claims I want qualify for the bonus 0.5% bonus in 2014 AND avoid the 2.0% penalty in 2016 Report via registry Report all available individual measures (128, 130, 131, 154, 155, 182, and 245*) Select 9 individual measures (or if less available 1-8) Need to confirm with your registry which measures are available Report one measures group (Back pain: 148-151) * Providers will report all applicable measures; however, the chronic wound care measure may not apply to all clinics Should I participate in PQRS in 2014 ? Report via claims I ONLY want to avoid the -2.0% penalty in 2016 Report via registry Select 3 individual measures (may choose from: 128, 130, 131, 154*, 155*, 182, or 245) Select 3 individual measures (select 3 of the individual measures offered by your registry) Report one measures group (Back pain) * Providers who choose to report 154 must also select 155 as these measures are paired; they count as two individual measures but 154 triggers 155 2014 Individual Measures for PTs # Measure Description Claims Registry 126 Diabetes Mellitus: Diabetic Foot and Ankle Care, Peripheral Neuropathy: Neurological Evaluation X 127 Diabetic Mellitus: Diabetic Foot and Ankle Care, Ulcer Prevention Evaluation of Footwear X 128 Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-up X X 130 Documentation and Verification of Current Medications in the Medical X Record X 131 Pain Assessment Prior to Initiation of Patient Treatment X X 154 Falls: Risk Assessment X X 155 Falls: Plan of Care X X 182 Functional Outcome Assessment X X 245 Use of Wound Surface Culture Technique in Patients with Chronic Skin Ulcers (Overuse Measure) X X 2014 Individual Measures for PT’s # Measure Description Claims Registry 217 Change in Risk-Adjusted Functional Status for Patients with Knee Impairments X 218 Change in Risk-Adjusted Functional Status for Patients with Hip Impairments X 219 Change in Risk-Adjusted Functional Status for Patients with Lower Leg, Foot or Ankle Impairments X 220 Change in Risk-Adjusted Functional Status for Patients with Lumbar Spine Impairments X 221 Change in Risk-Adjusted Functional Status for Patients with Shoulder Impairments X 222 Change in Risk-Adjusted Functional Status for Patients with Elbow, Wrist, or Hand Impairments X 223 Change in Risk-Adjusted Functional Status for Patients with a Functional Deficit of the Neck, Cranium, Mandible, Thoracic Spine, Ribs, or other General Orthopedic Impairment X 2014: Measures Group for PTs • Group Back Pain Measure • Must report all 4 measures in the group; may not be reported individually # Measure Description Claims Registry 148 Back Pain: Initial Visit X 149 Back Pain: Physical Exam X 150 Back Pain: Advice for Normal Activities X 151 Back Pain: Advice Against Bed Rest X PQRS Measure Changes for 2014 Measure Number Measure Title Changes Details 126 & 127 Diabetes Measures Registry reporting only in 2014 The diabetes measures (126 & 127) will not be reportable via claimsbased reporting in 2014 130 Current Medications Reporting every visit for 97001, 97002 AND 97110, 97140, 97532 Therapists must now report this measure when billing 97110, 97140, AND 97532 in addition to 97001 and 97002 131 Pain Assessment Reporting every visit for 97001, 97002 AND 97532; measure updated Therapists must now report this measure when billing 97001, 97002, AND 97532 148-151 Back Pain Measures Group Registry reporting only in 2014 The back pain measures group (148-151) will not be reportable via claims-based reporting in 2014 Please review all 2014 measure specifications in detail for your clinic’s selected measures to ensure that you are up to date with the current measures requirements PQRS Measure Changes for 2014 Measure Number Measure Title Changes Details 155 Falls Plan of Care Change in instructions and numerator definitions Consideration of Vitamin D supplementation and balance, strength, and gait training 182 Functional Outcome Assessment Change in numerator definitions AND addition of new numerator code G9227: Functional outcome assessment documented, care plan not documented, documentation the patient is not eligible for a care plan 246 Chronic Wound Care (Wet to Dry Dressing) Removal of 97001 and 97002 from numerator Therapists cannot report this measure in 2014; 97001 and 97002 removed from measure numerator definition 321 Participation in Systematic Clinical Database Registry Measure removed from program This measure will be removed from the PQRS program in 2014 Please review all 2014 measure specifications in detail for your clinic’s selected measures to ensure that you are up to date with the current measures requirements PT Measures and National Quality Strategy Domains Communication an care coordination • Falls plan of care (#155) • Functional assessment (#182) • FOTO measures (#217-223) Community / population health • BMI screening (#128) • Pain assessment (#131) Efficiency and cost reduction Safety Effective clinical care Person- and caregivercentered experience and outcomes • Back pain measures group (#148) • Medication verification (#130) • Falls risk (#154) • Diabetes measures (#126 &127) • Back pain measures group (#149-151) • Chronic wound measure (#245) • N/A PQRS 2014 Challenges Challenges Confusion about the number of measures to submit in 2014 Resources • www.apta.org/pqrs • Reporting Requirements for 2014 • Podcast: PQRS 2014 Summary of Changes Unsure about where to find data collection forms for claims- based submission in 2014 • 2014 Data Collections Sheets Looking for measure updates for 2014 • • • 2014 PQRS Group Measures 2014 PQRS Individual Measures Claims Measures Quick Reference Guide 2014 Podcasts • Unsure of how to handle measure #130 • Podcast: Measure Specifications for Measure 130: Documentation of Current Medications Future Trends PQRS • Move to 9 measures for successful reporting • Elimination of claims-based data submission • Increased use of registry and EHR reporting • Elimination of claims-based reporting 2017? PQRS Resources • APTA: Quality Resources http://www.apta.org/PQRS • CMS- PQRS page https://www.cms.gov/PQRS/ • Quality Net (general questions or feedback reports) https://www.qualitynet.org/ 866 288 8912 (option #1, then #7) Functional Limitation Reporting (FLR) Middle Class Tax Relief Act of 2012 February 2012 Congress mandates CMS to collect functional info on Medicare beneficiaries receiving therapy services under Part B FLR Ongoing February 2014 Medicare continues to work through system modifications; anticipating future evolutions of FLR FLR Implementation January 1, 2013 Testing phase begins for the collection of functional data Final Physician Fee Schedule Rule November 2012 Outlines the regulations around the new claimsbased reporting program for therapy services FLR Payment Adjustment Phase October 1, 2013 Originally slatted for July 1, 2013 this was delayed until October 1; providers began reporting processing issues in mid November From Law to Implementation Legislative Congress MCTRA Regulations/ Guidelines CMS 2012 Final Physician Fee Schedule, FAQs, MLN Matters Implementation Medicare Administrative Contractors NGS CGS Novitas Palmetto Cahaba First Coast APTA resources WPS Noridan FLR: Continuing to Evolve Tracking of FLR Episode • FLR tracking: • per beneficiary, • per therapy discipline, and • per billing provider NPI • (ie, per facility or practice, as identified by National Provider Identification or tax identification). Beneficiary (HIC#) Discipline (PT, OT, SLP) Facility (Tax ID or NPI) Discharge of FLR Episode Formal DC appointment Unanticipated DC Submit Gcodes- DC and goal No codes submitted Medicare DCs episode 60 calendar days from the last recorded date of service Patient returns to therapy within 60 calendar days of last recorded date of service If same issue/ limitation, continue reporting on that limitation If new issue/ limitation DC original primary and report on subsequent (DC original on visit 1 and begin reporting of new primary on visit 2 Return to Therapy within 60 Days • Therapist must decide if • The patient is returning for the same issue/ primary limitation (carry, moving and handling objects) OR • There is a new primary limitation associated with a new diagnosis (changing and maintaining body position)* Determine primary functional limitation Carrying, moving and handling objects (original diagnosis) Changing and maintaining body position (new diagnosis) * If the therapist determines that there is a new primary functional limitation, the he/she would end reporting on primary functional limitation for the previous episode (carry, moving and handling objects) and begin reporting on the new primary limitation on visit 2. Return to Therapy After 45 Day Absence Initial Evaluation Visit 1/6/2014 G8984 CK GP* G8985 CI GP 6th visit (Unanticipated DC) 1/23/2014 No codes submitted; unanticipated 1st Visit (Returns (Returns with with new same DX)DX) 2/12/2104 2nd Visit (Begin reporting subsequent) G8984 CJ GP G8985 CI GP G8986 CI GP G8981 CJ GP* G8982 CI GP *Carrying, moving, and handling objects **Changing and maintaining body position Multiple Diagnoses and POCs • FLR must occur for every beneficiary being seen by each discipline in a given facility/ practice • Two plans of care can exist concurrently for a beneficiary being seen with two different diagnoses by two different referring physicians • Two plans can be combined into a single plan of care if one of the two referring physician is willing to certify the POC Multiple Plans of Care Same Facility or Practice Different Facility or Practice Different discipline Multiple POC Same discipline Multiple POC Same discipline Multiple POC Each therapist identifies primary limitation for their POC Therapists coordinate and identify one primary limitation to be reported under one POC Each therapist identifies a primary limitation for the POC Treatment days for both conditions are counted towards the reporting frequency –each treatment day counts towards the total number of days the beneficiary received services, under both POCs. Note: It counts as one treatment day when services are received on the same date of service under both POCs FLR with Addition of Second Diagnosis to POC New DX for active POC FLR Coding Ongoing reporting Therapist performs evaluative procedure Limitation associated with new DX is different: submit 3 Gcodes (like one time visit) Can submit updated current and goal status on day of evaluative procedure; restart count Can choose to end reporting on primary and begin reporting on new limitation for second DX on the next visit Limitation is same as primary; revise POC and report current and goal codes Ongoing reporting continues; count restarts Addition of Second DX to an Active POC Initial Evaluation Visit Re-evaluation (6th Visit)* G8984 CK GP G8984 CJ GP G8985 CI GP G8985 CI GP 14th Visit (End reporting primary) 15th Visit (Begin reporting subsequent) D/C Visit G8985 CI GP G8986 CI GP G8981 CJ GP G8981 CJ GP G8982 CI GP G8982 CI GP G8983 CJ GP G8982 CI GP G8983 CI GP * Count does not restart when billing only the 3 Gcodes; must submit updated data on primary limitation to restart count PTA and FLR • Special exceptions in which a PTA may report Gcodes as determined by the PT: • Reporting of a new, subsequent functional limitation (PT ended reporting of primary limitation and determined Gcodes for subsequent limitation on previous visit) • Discharge anticipated within 3 treatment days of the progress report (PT determined Gcodes on date of progress report) Unique Clinical Situations Clinical Situation FLR: No FLR: Yes Comment Observation status X Emergency department X Short procedure stay X Typically billed under Medicare part B Re-billing under part B X Re-billing a denied part A acute care stay under part B subject to FLR DME billing X Once pt admitted, typically converted to part A; FLR not required if billing under part A FLR required for all therapy services associated with the always and sometimes therapy code list*. Also includes CPT codes for “Application of Casts and Strapping”, as clinically applicable *http://www.cms.gov/Medicare/Billing/TherapyServices/AnnualTherapyUpdate.html Resources for Ongoing Guidance Challenges Strategies Tracking of FLR episode, including discharge of episodes • Podcast on discharge reporting • Report D/C G-codes in charts even if you do not submit the data Multiple diagnoses and plans of care (POC)** • Case scenarios • Podcast on mult. dx and POC Role of PTA in FLR • Podcast on PTA and FLR Unique clinical situations: observation status patients, re-billing • FAQ documents • Podcast observation status Current status of claims and FLR • • • • FAQ documents Claim form examples Case scenarios PTNow Current Status of Claims and FLR • National implementation delayed until October 1, 2013 • Systems issues • Claims splitting • Delayed/ out of sequence processing • Incorrect visit counts • Required reporting at 10th/20th/etc despite early reporting • Problems with 60 day discharge • Issues with 3Gcode submission with an active POC • New FLR complaint form • Data being shared with Medicare staff weekly 45 Complaints by Month/ Year Month Year Number of Complaints October 2013 3 November 2013 7 December 2013 3 January 2014 15 February 2014 42* March 2014 89** * Standardized data collection implemented ** Data complete thru 3/25/2014 46 FLR: % of Complaints by MAC 1% 8% 8% 6% 14% Cahaba 9% CGS NGS Noridian Novitas Palmetto 19% 35% WPS First Coast 47 FLR: Number of Complaints by Type and 32 MAC 30 24 22 20 15 12 6 3 2 3 2423 1 1 Cahaba 6 NGS 8 Novitas 7 11 8 5 1314 45 5 Palmetto 6 2 4 9 6 2 WPS 4 2 44 1 Noridian 4 1 CGS 2 2 First Coast Count of Count discrepancy Count of October 1 restart Count of Delayed payment Count of Claims Splitting Count of Processing out of order Count of Other Simple FLR Coding Errors • Common issues that may cause claims to be returned unpaid: • Use of $0.00 instead of $0.01 • Leaving off the GP or severity modifiers • Incorrect submission of Gcodes • Changing categories mid episode • Submission of wrong Gcode (discharge vs current) • Claims splitting • Recommend placing FLR codes as line items directly after procedural codes APTA Functional Limitation Resources • http://www.apta.org/FLR • Resources include: • FAQ documents • Case scenarios • Webinar • Discussion forum • Toolkit • CMS links • PTNow (other tests and measure information) http://www.ptnow.org/FLR/Tests Questions [email protected] OR 800-999-2782 ext 8511