Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
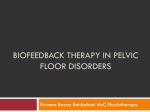
UNJ June 2005-206.ps C O N T I N U I N G E D U C A T I O N 5/18/05 3:52 PM Page 206 Biofeedback Therapy In Pediatric Urology Jacqueline Liberati B iofeedback treatment uses electronic or mechanical instruments to relay visual and/or auditory evidence to assist a person in gaining control over a physiologic process or function. In pediatric urology patients, biofeedback treatment is used to promote retraining of pelvic muscles. Figure 1 depicts the pathophysiology of dysfunctional voiding. In the figure, increased pelvic floor tension or overtraining is part of a vicious cycle that leads to pelvic floor and bladder dysfunction. Biofeedback methods are used to interrupt the cycle and promote pelvic floor relaxation and improve bladder function. With the use of biofeedback methods, the child learns about a unconscious physiologic process through visual, auditory, and/or tactile signals so that the unconscious physiologic process can be recognized and then changed or influenced (Hoebeke et al., 1996). Historical Review Biofeedback techniques to manage external sphincter-detrusor dyssynergia were initially described in the late 1970s. Interest has recently returned for biofeedback utilized as a treatment modality for children with dysfunctional voiding, recurrent Jacqueline Liberati, MSN, BS, RN, CRNP, is a Pediatric Nurse Practitioner, The Children’s Hospital of Philadelphia, Philadelphia, PA. Note: CE Objectives and Evaluation Form appear on page 211. 206 Biofeedback is one of the unique treatment options available in the management of voiding dysfunction in children.The focus of biofeedback in pediatric urology is on pelvic floor muscle retraining. Biofeedback uses monitoring devices and strategically placed electrodes to obtain and relay to the child visual and/or auditory cues on bladder emptying activity. The visual and auditory cues help train the child to sense, interpret, and respond to the body’s messages related to voiding activity. The overall goal is to improve the child’s ability to store urine and empty the bladder more effectively. urinary tract infections, or diurnal enuresis. The concept that pelvic floor musculature affects bladder function is not new. DePaepe and colleagues (2002) assert the pelvic floor is under voluntary control and plays an important role in the pathophysiology of lower urinary tract dysfunctions in children, especially of non-neuropathic bladder sphincter dysfunction. Allen and Bright (1975) reported on the relationship between dysfunctional voiding symptoms and objective pathology using urodynamics in the pediatric urological population. It was their idea that dysfunctional voiding represented a transitional stage between infant reflex voiding and mature voiding with cognitive reflex guarding. Cardozo, Stanton, and Hafner (1978) initially reported the use of biofeedback in a highly selected population of women with detrusor instability. Controversy exists in the literature in regard to the validity of objective versus subjective improvement of symptoms of voiding dysfunction in children (McKenna, Herndon, Connery, & Ferrer, 1999). Some believe that patients with voiding dysfunction should initially be treated with behavioral therapy for its long-term efficacy and biofeedback used only if this therapy fails (Weiner et al., 2000). Others, however, attest that biofeedback achieves perineal synergy, cures symptoms in children with detrusor-sphincter dyssynergia, and that it guarantees long-term clinical and functional recovery (Porena, Costantini, Rociola, & Mearini, 2000). Attainment of daytime dryness is an important milestone for children and has been noted to improve selfesteem dramatically (Hagglof, Andren, & Bergstrom, 1997). The earliest method of biofeedback training for detrusor overactivity focused on patient attempts to inhibit overactive detrusor contraction by concentrating, breathing deeply, clenching the fists, and generally relaxing while watching the cystometric curves or listening to the auditory signal to which the increase in detrusor pressure is converted. Maizels, King, and Firlit (1979) introduced urodynamic biofeedback as a new approach to treat vesical sphinc- UROLOGIC NURSING / June 2005 / Volume 25 Number 3 UNJ June 2005-207.ps 5/18/05 3:37 PM Page 207 Figure 1. Pathophysiology of Dysfunctional Voiding Voiding diaries Pharmacotherapy Bladder dysfunction Overtraining of pelvic floor Pelvic floor dysfunction Pelvic floor relaxation therapy ter dyssynergia in the pediatric population. Since that time, effective bladder retraining programs for children have been developed. VanGool, Vijverberg, Messer, Elzinga-Plomp, & deJong (1992) described an effective treatment program involving a 10day inpatient therapy and biofeedback via uroflowmetry and urine volume diaries. Biofeedback has previously been used successfully to treat various pelvic floor dysfunctions, such as urinary incontinence and pediatric detrusorsphincter dyssynergia (Sugar & Firlit, 1979; Wennergren & Oberg, 1995). Despite the postulated success of biofeedback in pediatric urology, it is apparent that this therapeutic approach is not well studied in the literature. Often patients have daytime and/or nighttime enuresis. For children with urinary incontinence and bladder overactivity, the goal is dryness. For children with vesicoureteral reflux and recurrent urinary tract infections, the goal of biofeedback is to establish low pressure cycling of the bladder. For children with severe voiding dysfunction, significant improvement of symptoms, rather than elimination of symptoms, is the targeted outcome goal (management versus cure). The common goal of biofeedback is to make children aware of their pelvic floor musculature and to teach them functional ways of using these muscles with voiding. Goals of Treatment To grasp the basis of voiding dysfunction and the mechanics of biofeedback, it is important to understand the relationship between the nervous system (brain and spinal cord) and the urinary system. The brain and spinal cord coordinate the functions of the body’s organ systems, including the kidneys and the bladder. The kidneys filter waste from the blood and dispose of this waste in the urine. The The goals of biofeedback vary with the etiology of the problem. Children with bladder sphincter dysfunction (defined as contraction of the pelvic floor muscles during voiding in the absence of obstruction) may present with urgency, frequency, and occasional recurrent urinary tract infections and vesicoureteral reflux (McKenna et al., 1999). Biofeedback Methods UROLOGIC NURSING / June 2005 / Volume 25 Number 3 ureters carry the urine down to the bladder where it is stored until time for emptying or voiding. The bladder stretches and relaxes as it fills and then squeezes or contracts as it empties. When the bladder is full, a signal is sent to the brain. The brain makes us aware of the need to urinate. As the bladder muscle contracts, a band of muscles at the bladder opening, called the external or urethral sphincter, relaxes to let the urine out. This muscular band is also responsible for tightening to keep urine in as the bladder fills. The surrounding muscles (lower pelvic muscles) hold the pelvic organs in place. Tightening of the pelvic muscles also tightens the urinary sphincter. Voiding dysfunction occurs when one or several physiological mechanisms do not work in a coordinated fashion. These include the inability to sense when the bladder is full, relax the sphincter, tighten the sphincter, and determine when the bladder is empty. Teaching children the dynamics of voiding can be challenging. The success of biofeedback therapy depends greatly on patient and parent compliance, motivation to learn, and a willingness to participate. The procedure must be discussed clearly with the patient and family. The child’s session must be individualized and be developmentally appropriate for that child. Each child is taught to identify differences in relaxation, contraction, and straining. Children observe changes in the electromyography tracing on the monitor and wait for cues by the nurse to elicit a contraction or relaxation. Under guidance the child is taught to optimize pelvic floor relaxation with a stool placed beneath the feet or with knees spread which helps to relax the perineum. Biofeedback involves use of electromyography and uroflowmetry. Electromyography patches are placed perianally at the 3 and 9 207 C O N T I N U I N G E D U C A T I O N UNJ June 2005-208.ps C O N T I N U I N G E D U C A T I O N 5/18/05 3:37 PM Page 208 Figure 2. Biofeedback Involves Use of Electromyography and Uroflowmetry Figure 3. The External Unit Is Attached to a Computer, Which Relays the Image to a Monitor Surface EMG electrodes are placed at the 3- and 9-o’clock positions of the the child’s perineum. An additional surface electrode is placed on the rectus abdominus to measure abdominal muscle activity. o’clock positions. A sensor patch is placed on the abdomen to monitor accessory muscle activity (see Figure 2). Leads are connected to an external unit that interprets and analyzes the electrical impulses received from the pelvic floor muscles. The external unit is attached to a computer, which relays the image to a monitor (see Figure 3). At the beginning of all sessions, a provider obtains a voiding history and assesses if the child is a potential candidate for biofeedback. The provider then discusses the accomplishments of the previous treatment session, patient progress at home, incidence of breakthrough infection, compliance with home exercises, and addresses any questions the family has concerning the pelvic floor muscle retraining program. After all questions and/or concerns are addressed, the biofeedback session commences with placement of perianal leads. Patients are completely dressed and reclined in an adjustable chair during the session. The session schedule involves the patient first relaxing and the nurse obtaining a baseline relaxation reading. Patients 208 then perform Kegel exercises and short bursts of pelvic floor contractions, called quick flicks. When patients are not able to isolate the pelvic floor muscles, immediate instruction is given on how to isolate them (focusing on squeezing the leads on the buttocks). The patient is then instructed to perform four, 5-second repetitions of quick flicks, that is, short contractions and relaxations with the nurse and patient watching electromyography-generated activity patterns on the television screen. This is followed by a 30-second relaxation interval. The patient then performs a series of eight, 10-second alternating contractions and relaxations. This interval is then followed by a 30-second rest period. Screening uroflowmetry and bladder scan for post-void residual urine are performed. The child is asked if there is residual urine in the bladder. This sequence is repeated until the bladder is empty or the child is unable to void any more. Over time, the child becomes increasingly aware of the difference between poor bladder emptying and an empty bladder. An initial biofeedback session lasts approximately 90 minutes and a followup session lasts 60 minutes, depending on how well the child grasps the concept and practices at home. Three sessions, 4 to 6 weeks apart, is a usual starting point; however, timing of sessions is not welldocumented in the literature. Other treatment plans include biweekly sessions or biofeedback until detrusor-sphincter dyssynergia is resolved (Porena et al., 2000). Timing between sessions essentially depends on progress and retention of concepts taught previously. It is generally accepted that biofeedback is the treatment of choice for children with dysfunctional voiding in the form of staccato (fail to empty or store urine) or fractionated (further hyperactivity of the pelvic floor which stops flow with voiding occurring in several portions) UROLOGIC NURSING / June 2005 / Volume 25 Number 3 UNJ June 2005-209.ps 5/18/05 3:38 PM Page 209 Pediatric urologic nurses must be aware of the back, have facilitated the diagnosis and management of detrusor-sphincter dyssynerincontinence beyond the typical age of toilet training. gia, which has been identified as a major cause of voiding (Schulman, Von Zuben, dysfunction, establishing and disturbance in children who are Plachter, & Kodman-Jones, 2001). maintaining good bladder habits uro-anatomically and neurologiTo date, however, there has been takes a lot of work. A lot of cally normal (Porena et al., 2000). no agreement as to the optimal “homework” is given outside of The etiology of dysfunctional form of biofeedback. Some clinic. This includes comprehenvoiding is controversial. The clinibiofeedback programs attempt to sive voiding and stooling diaries cal presentation varies and the funnel the attention of children to track voiding habits and acciprecipitating event in autonomic through intensive inpatient prodents. Maintaining the child’s somatic dyssynergia usually regrams (McKenna et al., 1999). At motivation to work vigilantly on mains obscure. Jayanthi, Khoury, The Children’s Hospital of developing healthy voiding skills and McLorie (1997) suggested that Philadelphia (CHOP), the current and to adhere to the treatment there may be a subgroup of chiloutpatient biofeedback program recommendations over time is a dren in whom voiding dysfuncfocuses on what is interpreted as big challenge. For many chiltion is congenital rather than the underlying pathologic condidren, a reward system is needed acquired. This hypothesis is diffition. to help them focus on establishcult to confirm. Some authors The key to successful ing bladder routines. Behavior have suggested that the beneficial biofeedback is both patient and therapy interventions such as results of biofeedback may be due parent participation and motivamodeling healthy urinary habits to intensive one-on-one education tion. Computer games in biofeedare often needed to alter malrather than physiologic changes back serve as a mechanism to adaptive child behaviors that induced by biofeedback (Wein, engage the child and maintain interfere with treatment progress. 1982). Hence, further study is interest in the program. It is a Success can only be achieved if needed. reproducible technique and is the child is an active participant Cost Effectiveness advocated by others (Pfister et al., in treatment and if the child 1999). The games provide visual believes there are benefits to Urinary incontinence and biofeedback as well as positive obtaining proper voiding habits. voiding dysfunction are common reinforcement. Game action is Pediatric urologic nurses problems, estimated to affect 13 controlled by patient pelvic floor must be aware of the significant million adults and children in muscle activity. psychosocial impact of urinary the United States, and to account incontinence beyond the typical for costs exceeding $15 billion Outcomes age of toilet training. School, per year (Fantl et al., 1996). It is peer, and family relationships are In biofeedback therapy, chilassociated with a high burden of often affected, and can result in dren learn during voiding to susillnesses, high costs, and subdamage to the child’s developing tain concentration and maintain stantial negative effect on quality self-esteem. Problems related to a relaxed pelvic floor and volunof life. Many medical and psyself-esteem may require additary urethral sphincter (Porena et chological insurance plans now tional referrals to appropriate al., 2000). The accurate monitorcover biofeedback for various health care providers as needed. ing of this physiological response conditions. Some require co-payPediatric nurses are in key posiby electromyography and the ments. Other plans have annual tions to identify children with immediate recognition by feedcaps. A prescription for the trainvoiding problems. Once the back of the changes provide the ing, along with a diagnosis, may problem has been acknowledged, basis for therapeutic retraining. be required from a provider nurses can assess the problem Outcome variables include under the medical part of the and its impact on the family; improved urinary continence, plan. Intangible benefits from educate parents, children, and fewer urinary tract infections, biofeedback therapy include others regarding causes; discuss and less vesicoureteral reflux. increased patient satisfaction and management options; and refer Improvement with continence better patient compliance. children for medical intervention may lead to improved selfAlthough not stated in the literawhen necessary. esteem for the child as an added ture, one can imagine how outcome. biofeedback therapy can provide Research Implications a number of benefits that can be Nursing Implications Noninvasive urodynamic measured and put into dollar For children with voiding techniques, including biofeedterms. These include reduced significant psychosocial impact of urinary UROLOGIC NURSING / June 2005 / Volume 25 Number 3 209 C O N T I N U I N G E D U C A T I O N UNJ June 2005-210.ps C O N T I N U I N G E D U C A T I O N 5/18/05 3:38 PM Page 210 Table 1. CPT Codes for Reimbursement • • • • Biofeedback therapy – 90911 Complex uroflow – 51741 Pelvic floor EMG – 51784 Bladder scan residual – 51798 incidence of urinary tract infections and vesicoureteral reflux, fewer visits to the physician, fewer hospitalizations, and decreased use of medications. By treating the underlying cause, costs are greatly reduced, patients are less burdened, and families can enjoy a better quality of life. Reimbursement for the evaluation and treatment of patients with voiding dysfunction varies from practice to practice, but most often involves a combination of the different codes (see Table 1). The initial evaluation involves a consultation code, usual detail (99253) or comprehensive (99254) level. If screening radiologic studies are performed, this is usually done through the radiology office and there is usually not a billable service for the urologist involved in that evaluation. If the patient proceeds with further noninvasive urodynamic studies, he or she would receive a simultaneous uroflow study, an EMG, and bladder ultrasound for PVR (codes 51741, 51784, 51798). The patient who proceeds with biofeedback treatment would be coded as 90911 for each session. Most patients are re-evaluated at the end of the biofeedback sessions by repeating the simultaneous urine flow, EMG, and PVR to be certain the treatment did not result in increased hyperactivity of the pelvic floor, and to be certain that the flow pattern and EMG pattern are in line with the patient improvement. Conclusion Biofeedback can be a suc- 210 cessful modality for dysfunctional voiding in children associated with recurrent urinary incontinence, urinary tract infections, and vesicoureteral reflux. Many treatment programs typically utilize formal urodynamic studies to develop an inpatient treatment program. At CHOP, however, the initial evaluation and treatment of children with voiding dysfunction is on an outpatient basis, focusing on correcting pelvic floor voiding immaturity. Although this approach is time consuming and labor intensive for the patient and the nurse practitioner, the advantages are that it is noninvasive and makes the patient more responsible and less passive regarding the condition. It provides positive results in most patients in a short duration of time. Biofeedback can be readily performed using the resources available in most pediatric urology practices on an outpatient basis. Given the excellent results in the CHOP outpatient clinic, this strategy is recommended as adjunctive therapy in pediatric patients recalcitrant to standard behavior modification. • References Allen, T., & Bright, T. (1975). Urodynamic patterns in children with dysfunctional voiding problems. Journal of Urology, 119, 247-257. Cardozo, L., Stanton, S., & Hafner, J. (1978). Biofeedback in the treatment of detrusor instability. British Journal of Urology, 50, 250. DePaepe, H., Renson, C., Hoebeke, P., Raes, A., Van Laecke, E., & Vande Walle, J. (2002). The role of pelvic-floor therapy in the treatment of lower urinary tract dysfunctions in children. Scandinavian Journal of Urology and Nephrology, 36, 260-267. Fantl, J., Newman, D., Colling, J., DeLancey, J., Keeys, C., Loughert, R., et al. (1996). Urinary incontinence in adults: Acute and chronic management. Clinical Practice Guideline No. 2 U.S. Department of Health and Human Services, Public Health Service. Rockville, MD: Agency for Healthcare Policy and Research. Hagglof, B., Andren, O., & Bergstrom, E. (1997). Self-esteem before and after treatment in children with nocturnal enuresis and urinary incontinence. Scandinavian Journal of Urology and Nephrology, 183, 79. Hoebeke, P., Walle, J., Theunis, M., DePaepe, H., Oosterlinck, W., & Renson, C. (1996). Outpatient pelvic floor therapy in girls with daytime incontinence and dysfunctional voiding. Pediatric Urology, 48, 923927. Jayanthi, V., Khoury, A., & McLorie, G. (1997). The nonneurogenic neurogenic bladder of early infancy. Journal of Urology, 158(3), 1281-1285. Maizels, M., King, L., & Firlit, C. (1979). Urodynamic biofeedback: A new approach to treat vesical sphincter dyssynergia. Journal of Urology, 122, 205. McKenna, P.H., Herndon, C.D., Connery, S., & Ferrer, F.A. (1999). Pelvic floor muscle retraining for pediatric voiding dysfunction using interactive computer games. Journal of Urology, 19,162(3 Pt 2),1056-1062; discussion 1062-1063. Pfister, C., Dacher, J., Gaucher, S., LiardZmuda, A., Grise, P., & Mitrofanoff, P. (1999). The usefulness of a minimal urodynamic evaluation and pelvic floor biofeedback in children with chronic voiding dysfunction. British Journal of Urology, 84(9), 1054-1057. Porena, M., Costantini, E., Rociola, W., & Mearini, E. (2000). Biofeedback successfully cures detrusor-sphincter dyssynergia in pediatric patients. Journal of Urology, 162(6), 19271931. Schulman, S.L., Von Zuben, F.C., Plachter, N., & Kodman-Jones C. (2001) Biofeedback methodology: Does it matter how we teach children how to relax the pelvic floor during voiding? Journal of Urology, 166(6), 2423-2426. Sugar, E., & Firlit, C. (1982). Urodynamic biofeedback: A new therapeutic approach for childhood incontinence/infection (vesical voluntary sphincter dyssynergia). Journal of Urology, 128(6), 1253-1258. VanGool, J., Vijverberg, M., Messer, A., Elzinga-Plomp, A., & deJong, T. (1992). Functional daytime incontinence: Nonpharmacological treatment. Scandinavian Journal of Urology & Nephrology, 141, 93. Wein, A. (1982). Editorial. Journal of Urology, 128, 1253. Weiner, J., Scales, M., Hampton, J., King, L., Surwitt, R., & Edwards, C. (2000). Long-term efficacy of simple behavioral therapy for daytime wetting in children. Journal of Urology, 164, 786-790. Wennergren, H., & Oberg, B. (1995). Pelvic floor exercises for children: A method treating dysfunctional voiding. British Journal of Urology, 76, 919. UROLOGIC NURSING / June 2005 / Volume 25 Number 3