Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
CLIN.CHEM.40/9, 1739-1743 (1994)
#{149}
Molecular
Pathology
Tamm-Horsfall Glycoprotein: Role in Inhibition and Promotion of Renal Calcium
Oxalate Stone Formation Studied with Fourier-Transform Infrared Spectroscopy
Rainer Kn#{246}rle,”5
Peter Schnierle,2 Alexander Koch,1 Niels-Peter Buchholz,3 Franz Hering,4
Theodor Ackermann,’ and Georg Rutishauser3
Tamm-Horsfall glycoprotein (THP) from healthy probands inhibits the precipitation of calcium oxalate,
whereas THP from individuals who repeatedly develop
calcium oxalate stones has no effect or even promotes
precipitation. Using Fourier-transform infrared spectroscopy, we found a structural differentiation between these
functionally different THP5: a decisive difference in sialic
acid content. Quantitative analysis for sialic acid showed
the same results. THP from healthy probands had a high
sialic acid content (51 ± 9 glkg), whereas THP from
recurrent stone formers had a decreased sialic acid content (21 ± 4 g/kg). This explains the dual role of THP in
the precipitation of calcium oxalate and the formation of
renal stones and shows the importance of glycosylationin
the function of this glycoprotein.
Indexing
Terms: glycated proteins/sieiic acid/kidney stones/uiine/
uromodulin
In individuals
who develop renal stones and in
healthy persons, urine is a supersaturated
solution of
calcium oxalate, the most common component of kidney
stones (1). The urinary concentration
of calcium oxalate
is at least four times higher than its solubility
(2),
suggesting that crystal formation occurs in both healthy
persons and stone formers (3). Consequently,
supersaturation cannot be the sole explanation for the formation
of calcium oxalate stones.
The main theories concerning stone formation in the
urinary
tract are the matrix theory and the theory of
inhibitors
(or, better, lack of inhibitors).
Based on results from analyses of many stones, the matrix theory
(4) proposes that urinary macromolecules
promote stone
formation by binding
inorganic ions and acting as a
framework for the deposition of stone salts. Such macromolecules should be present only in the urine of stone
formers or should at least be present in excess in such
persons. The inhibitor theory (5) explains
the fact that
healthy persons do not develop clinically
significant
stones by postulating
the presence of inhibitors in urine
that prevent nucleation,
growth, and aggregation
of
crystals
in the urinary tract. Accordingly
and con‘Department
of Physical
Chemistry,
University
of Freiburg,
Albertstr. 23a, 79104 Freiburg, Germany.
2Iituth
of Inorganic Chemistry, University of Basel, Spitalstr. 51, 4056 Base!, Switzerland.
3Clinic of Urology, Department of Surgery, University
Hospital
Kantonsspital Base!, Spitalstr. 21, 4031 Basel, Switzerland.
Urological Clinic, Kantonsspital
Baden, 5404 Baden, Switzerland.
5Author for correspondence. Fax +41/761/2036189.
Received February 17, 1994; accepted May 31, 1994.
Hans Seiler,2
stone formation
in patients with urolithiasis
would be indicative of a lack or deficiency of these inhibitors.
In the inhibitor
theory, pathogenesis
of stone formation is regarded as the result of an imbalance
between
supersaturation
with calcium oxalate and inhibitory activity (6). Several studies have identified naturally cccurring
inhibitory
substances
(7), of which there are
usually
considered
to be at least two groups (8): (i) the
so-called chelating inhibitors, e.g., magnesium
ions,
which reduce free ion activity and therefore reduce urinary supersaturation,
and (ii) the mostly macromolecular polyanionic inhibitors, which do not influence supersaturation but bind to crystal surfaces, block growing
sites, and modifSr attractive
or repulsive forces between
crystals so that growth and especially
crystal aggregation is inhibited (9).
All renal calcium oxalate stones contain a macromolecular organic matrix (10), and most include TarnmHorsfall glycoprotein
(THP) (11). The most abundant
protein in human urine and present in the kidneys of all
placental
mammals,
THP is -30% carbohydrate
by
weight. The physicochemical
and biological properties
of THP have been studied extensively,
but its physiological function has remained obscure (12). According to
its cDNA sequence, THP exhibits eight possible N-glycosylation
sites, of which five usually are utilized (13).
Proteolytic
digests of THP reveal that every carbohydrate moiety shows a different glycosylation
pattern
(14), and the site heterogeneity
is substantial.
The resulting glycoforms of THP produced (15) have different
physical
and biochemical properties, which may lead to
functional diversity. Early studies on the chemical composition of THP showed -4% (by weight) glycosylation
with sialic acid (16). Under physiological
conditions,
sialic acid is negatively
charged, causing a low p1 value
for the glycoprotein
(17).
Because of its presence in renal stones, THP has been
proposed to play a role in renal stone formation. Some
groups have described a promoting influence of THP on
the precipitation
of calcium oxalate, according to the
matrix theory (18, 19), whereas others have shown that
it has inhibitory
properties and probably acts as an
aggregation
inhibitor (20, 21).
Our earlier studies with the oxalate tolerance test
(22) showed that THP from healthy probands had an
inhibitory
effect on the precipitation
of calcium oxalate,
whereas THP from recurrent
calcium oxalate
stone
formers had no effect or often even a promoting one (23).
In the present study we used Fourier-transform
infrared
(FTIR) spectroscopy
and resolution
enhancement
by
versely,
CLINICAL CHEMISTRY, Vol. 40, No. 9, 1994 1739
Fourier seif-deconvolution
to elucidate possible structural differences between the two functionally
different
THPs revealed by the oxalate tolerance test. The spectroscopic methods were complemented
with biochemical
approaches, e.g., polyelectrolyte
titration or the thiobarbituric acid assay for sialic acids.
MaterIals and Methods
Reagents and Chemicals
Neuraininidase
acetylneuraminic
(from Clostridium
perfringens),
Nacid (sialic
acid), deuterium
oxide,
thiobarbituric acid, and fetuin were purchased from Sigma
Chemie, Deisenhofen,
Germany.
Poly-(1,l,-dimethyl-3,5diinethylene)-piperidinium
chloride, potassium polyvinylsulfate, and Toluidine Blue 0 were supplied from Aldrich
Chemie, Steinheim,
Germany.
All other reagents
were
purchased from Merck1 Darmstadt, Germany.
THP from 12 healthy probands and 13 recurrent stone
formers was isolated by a modified method of Tanun and
Horsfall (24). Urine samples (24-h) were precipitated
three times with 0.58 mol/L NaCl and the precipitates
dialyzed for 72 h. The final products were lyophilized.
Healthy probands were chosen randomly. Of both sexes
and various ages, they had no known stone episode so
far and no other disease at that time. Stone formers
were from the Kantonsspital
Base! and Kantonsspital
Baden, patients classified as recurrent
calcium
oxalate
stone formers; they were sex- and age-mixed and had no
urinary tract infections. We determined the concentration of THP in solution spectrophotometrically
at 277
nm, using an absorptivity
of 10.8 cm’ for 10 gIL (25).
Asialo-THP
was obtained from the healthy probands’
THP by two independent
methods, acid hydrolysis and
enzymatic digestion (26). Acid hydrolysis was carried
out in 50 mmol/L H2S04 at 80#{176}C
for 1 h. After adjusting
the pH of the hydrolysate
to -5.5, we extensively
dialyzed the glycoprotein against water and lyophilized the
product. For enzymatic cleavage, THP was incubated at
37#{176}C
for 24 h with neuraminidase,
50 kUIL, in 50
mmol/L sodium acetate/acetic
acid buffer, pH 5.5, containing 9 g/L NaCl, 1 g/L CaC12, and 0.2 g/L NaN3.
Neuraminidase
from C. perfringens
is specific for the
cleavage
of terminal
a-2,3-, a-2,6-, and a-2,8-linked
sialic acid. After digestion, the glycoprotein
was recovered by extensive dialysis against water and then lyophilized.
FTIR
Investigations
of solutions of proteins in the infrared
region are usually carried out in deuterium oxide (D2O)
because of the strong absorbance of water (H20) in this
spectral region. For H/D exchange we lyophilized the
dialyzed protein, dissolved it three times in deuterium
oxide, and lyophilized
again. The solutions were measured in a 50-pm pathlength
CaF2 cell. Spectra were
recorded with a Bruker IFS-113v FTIR spectrometer
equipped with a mercury-cadmium-telluride
detector
(Bruker
Analytische
Messtechnik,
Karlsruhe,
Germany). The spectrometer
was controlled by a CS-43 computer and OPUS-software
(also from Bruker). The re-
1740 CLINICALCHEMISTRY,Vol.40, No. 9, 1994
sults of 1024 scans were combined to produce a spectrum
of 2 cm’ resolution between wavenumbers
of 1850 and
1300 cm’.
THP Charge
The charge of THP was measured by polyelectrolyte
titration (27). A known amount of protein (50-150 g)
was preincubated
in a solution of poly-(1,1,-dimethyl3,5-dimethylene-piperidinium
chloride). After adding
the indicator Toluidine Blue 0, we titrated the excess
polycation with potassium polyvinylsulfate
at 23#{176}C
with
continuous stirring. The titration was monitored by continuous measurement
of absorbance at 520 nm. To improve the accuracy of determination,
we titrated dilution series of known THP content. The number of
charged residues per protein molecule was calculated
from the differences of the added and retitrated amounts
of polycation preincubated
with the protein sample.
Sialic Acid
Sialic acid was determined
in THP from 10 healthy
probands and recurrent stone formers by the thiobarbituric acid assay. After acid hydrolysis and subsequent
dialysis the diffusate was lyophilized.
The amount of
sialic acid was determined colorimetrically
according to
Aminoff (28), a sensitive method specific for free sialic
acid. In the reaction sequence, periodate oxidation and
coupling of the prechromogen
with thiobarbituric
acid
yields a red chromophore with an absorbance maximum
at 549 nm (29). The amount of sialic acid can easily be
calculated
from the absorptivity
at 549 nm. This assay
was tested with fetuin, a glycoprotein
containing
61
g/kg sialic acid (30). Acid hydrolysis revealed a sialic
acid content of 58 ± 3 g/kg, corresponding
to a relative
error of the determination
of 5%.
Results
Spectra of globular proteins measured as solutions in
D20 usually show two intense broad bands reflecting
vibrations
of the anude group: These are usually described as amide-I’ and amide-Il’ band. The conformationally sensitive amide-I’ band has an absorbance maximum between 1620 and 1660 cm’ and mainly results
from a C=O stretching mode. The amide-Il’ band (15001400 cm1), which is not sensitive to the type of secondary structure, is approximated
to a N-D vibration. In
addition to the ainide group of the peptide backbone,
amino acid side chains absorb in the infrared (31). The
carboxylate
groups of aspartic acid and glutamic acid
result in bands at 1583 and 1564 cm1, tyrosine at 1514
and 1616 cm1. The infrared spectrum of glycoproteins
results from vibrations both of the core protein and the
carbohydrate moiety. Contributions
of the carbohydrate
to the spectrum in the spectral region between 1850 and
1300 cm’ are assigned to vibrations of amide groups (in
N-acetylhexosamines),
carboxylate
groups (in uronic acids), and the C-H and C-O bond (32).
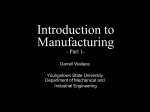
FTIR spectra of THP from healthy probands and recurrent stone formers show two absorbance maxima, at
1638 and 1454 cm
(Fig. 1, top). These bands consist of
C
C
L
1800
1700
1600
1400
1500
Wovenumber,
cm’
C
‘1
C
1800
1700
1600
1500
Wovenumber.
Differences between the spectra of THP from healthy
probands and that from recurrent stone formers are
greatest in the intensity
of the band at 1608 cm’,
which could be assigned to the asymmetric
stretching
vibration of the carboxylate group of sialic acid (32). All
healthy probands showed a clearly distinct band at 1608
cm’, but the band was nearly absent in 12 of 13 spectra
of THP from recurrent stone formers; the remaining
contributions
in this region result from vibrations
of
tyrosine side chains. Spectra of asialo-THP,
whether
obtained after chemical or enzymatic cleavage of sialic
acid, were identical.
Comparison
with the spectra of
untreated THP (Fig. 2) shows the disappearance
of the
carboxylate
vibration at 1608 cm’,
a clear indication
that this band results from vibrations
of sialic acid.
Moreover, the spectra of asialo-THP
resemble those of
THP from recurrent stone formers by having no spectral
feature at 1608 cm’
(Fig. 2). The differences of the
relative intensities
at 1608 cm’ most probably result
from different degrees of glycosylation
with sialic acid.
FTIR spectroscopic
investigations
of fetuin, another
glycoprotein
containing
sialic acid comparable
to the
amount in THP, and its asialo derivative
confirmed
these results (Fig. 3). The deconvoluted
spectra of fetuin
1400
cm’
Fig. 1. Top: Infrared spectra of solutionsof THP in 020; bottom:
deconvolutedspectraof the solutions.
(A) healthy proband; (B) recurrent stone former. Deconvolutionwas carried
out by usinga half-width athalf-height
of20 cm
mentfactor of2.
anda resolution
enhance-
a number of overlapping
components that can be identified by application of Fourier self-deconvolution
(33).
This procedure decreases the width of the bands, leading
to an increased
separation and thus better visualization
of the overlapping
component
bands comprising
the
composite band contour. Deconvolution
by half-width at
half-height
of 20 cm1 and a resolution enhancement
factor of 2 resolved bands at 1676, 1662, 1652, and 1636
cm’ (Fig. 1, bottom), which are assigned to vibrations
of the peptide backbone and correspond to the secondary
structure
of the core protein (34). The bands at 1636 and
1676 cm’
can be assigned to (3-sheets, whereas the
1652 cm’ band arises from both a-helix and random
coils. The band at 1662 cm’
is characteristic
for
13-turns. The spectra of both of the functionally
different
forms of THP are identical in this spectral region, indicating that the secondary
structure of the core protein is
unaffected
in the functional differentiation.
From the
relative areas, the 1636 cm’ band appears to be the
most prominent, indicating a high content of 13-sheets.
1750
1700
1650
Wovenumber.
1600
1550
cm’
-j
1750
1700
1650
Wovenumber,
1600
1550
cm’
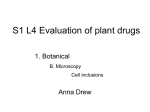
Fig. 2. Deconvolutedspectra of THP (A) and asialo-THP (B) from a
healthyproband (top) and from an oxalate stoneformer (bottom).
CLINICALCHEMISTRY,Vol.40, No.9, 1994 1741
I.,
0
A
1750
1700
1650
Wovenumber.
1600
1550
cm’
Fig. 3. Deconvoluted spectra of fetuin (A) and asialofetuin (B).
show a clearly distinct band at 1607 cm’ that is lacking
in the spectrum of asialofetuin.
The band at 1454 cm1 mainly results from the amide-Il’ band. This region also contains contributions
of
the carbohydrate
moiety. The complex structure of the
sialylated,
sulfated,
and N-acetylgalactosamine-contaming oligosaccharide
chains of THP leads to several
absorbances
between 1700 and 1350 cm’,
making a
complete assignment
of all frequencies
in this spectral
region difficult.
The results obtained by FTIR spectroscopy are supported by biochemical
methods. The sialic acid content
of THP was significantly
higher (P <0.001)
in 10
healthy persons (51 ± 9 g/kg, range 34-64 g/kg) than in
10 recurrent renal stone formers (21 ± 4 g/kg, range
13-29 g/kg). Healthy
probands
reveal a distinctly
greater content of sialic acid in THP than do recurrent
stone formers, in good agreement
with earlier investigations of THP (35). Polyelectrolyte
titration also shows
a loss of titratable
negatively
charged groups at THP
from recurrent stone formers (15 ± 6, range 7-20; in
contrast to THP from healthy persons showing 40 ± 10,
range 34-50; P < 0.05). These result from sialic acids as
well as from sulfated carbohydrates
and the amino acid
side chains.
Discussion
Application of FTIR spectroscopy allowed us to structurally differentiate
between the functionally
different
THPs from healthy probands and from recurrent calcium oxalate
stone formers.
Inhibitory
THP from
healthy
persons
was more highly glycosylated
with
sialic acid than the promoting THP from recurrent stone
formers.
These results confirm the concepts that (a)
glycosylation
is important
for the function of THP (36)
and (b) a lack of sialic acid is the first step in the
conversion of mucosubstances
to mineralizable
matrix
(37), which may lead to renal stone formation.
Our
results show that terminal
sialic acid is essential for the
inhibitory
function of THP from healthy persons.
Knowledge of these structural and functional differences of THP makes it possible to combine inhibitor
1742 CLINICALCHEMISTRY,Vol.40, No.
9, 1994
theory and matrix theory of renal stone formation with
regard to this glycoprotein.
As shown by our study and
earlier results (38), THP from healthy persons is a polyanionic
macromolecule.
According
to the proposed
mechanism
by which urinary
macromolecules
inhibit
crystal growth and aggregation
(9), such a molecule
could bind to the surfaces of growing calcium
oxalate
crystals, block the growing sites, and modifr attractive
or repulsive forces between the crystals, thereby impeding or preventing
aggregation
of the crystals. Consequently (39), no large crystal clusters would be formed
to obstruct the renal tubules and any microcrystals
formed due to supersaturation
could easily be washed
out from the urinary tract.
THP lacking sialic acid (i.e., with fewer negatively
charged groups), as is found in patients with calcium
oxalate urolithiasis,
would no longer be capable of binding effectively to these calcium oxalate crystals. In contrast, THP from stone formers presents an uncharged
surface that might, according to matrix theory, act as an
additional
surface for heterogeneous
nucleation
and
thus provide a framework for the deposition of stoneforming salts. This supports the idea (21) that stone
formers are no longer fully protected against the formation of large crystal aggregates,
which can be deposited
in the urinary
tract.
Although kidney stone formation is a complex multifactorial disease, the loss of this protection mechanism
of THP through an increase in the asialo-THP
glycoforms in urine seems to represent a major factor in renal
stone formation.
One possible explanation
for the lack of sialic acid in
the carbohydrate
moiety of THP from recurrent stone
formers may be the inhibition or a defect of an enzyme
involved in the processing of the oligosaccharide
chains.
Inhibition
of processing
of glycoproteins
has been reported in heavy alcohol consumption,
leading to an increase in asialotransferrin
glycoforms (40). Several inherited
diseases are associated
with abnormalities
in
the genes for glycosidases
or glycosyltransferases
(41).
A deficiency of N-acetylglucosamine
transferase
II gives
rise to congenital dyserythropoietic
anemia type 11(42).
Other examples of genetic diseases involving defective
oligosaccharide
biosynthesis
are I-cell disease and pseudo-Hurler polydystrophy,
in which a deficiency of phospho-N-acetylglucosaminyl
transferase
activity
is the
primary
cause (43). In this regard, investigations
of
THP from one family by circular dichroism showed an
inherited molecular abnormality
of the protein in children of recurrent stone formers (44), suggesting that the
recurrent formation of renal stones may be an inherited
disease caused by a deficiency of glycosidases
or glycosyltransferases.
In conclusion, FTIR spectroscopy allowed a structural
differentiation
between THP from healthy probands and
that from recurrent calcium oxalate stone formers. It
also demonstrated
the importance
of glycosylation
for
the functional activity of this glycoprotein,
showing that
the functional differences between the two THPs result
from different degrees of glycosylation
with sialic acid,
with the secondary structure of the core protein being
unaltered.
Depending on the glycosylation,
THP acts as
an inhibitor or promoter of calcium oxalate precipitation and thus of the renal stone formation process.
Deconvolution
of the infrared spectra was carried out with
RAMOP, a software written by D. J. Moffat, National Research
Council of Canada The technical assistance of Ursula Friedrich is
gratefully acknowledged. This work was supported by the Deutsche
Forschungsgemeinschaft
through SFB 60.
References
1. Coe FL, Parks JH, Asplin JR. The pathogenesis and treatment
of kidney stones [Reviewl. N Engi J Med 1992;16:1141-52.
2. Coe FL, Parks JH. Physical chemistry
of calcium stone disease.
In: Coe FL, Parks JH, eds. Nephrolithiasis: pathogenesis and
treatment, 2nd ed. Chicago: Year Book Medical, 1988:38-58.
3. Goidwasser B, Weinerth JL, Carson CC. Calcium stone disease:
an overview [Review]. J Urol 1986;135:1-9.
4. Boyce WH, King JS Jr. Present concepts concerning
the origin
of matrix and stones. Ann Rev NY Acad Sci 1963;104:563-78.
5. Howard JE, Thomas WC, Smith LH, Barker LM, Wadkuns CL.
A urinary peptide with extraordinary
powers against biological
“calcification” (deposition of hydroxyapatite crystals). Trans Assoc
Am Physicians 1966;79:137-45.
6. Robertson WG, Peacock M, Marshall RW, Marshall DH, Nordin
BEL. Saturation-inhibition
index as a measure of the risk of
calcium oxalate stone formation in the urinary tract. N Engi J Med
1976;294:249-52.
7 Ryall RL, Hannett RM, Marshall VR. The effect of urine,
pyrophosphate, citrate, magnesium and glycosaminoglycans on
the growth and aggregation of calcium oxalate crystals in vitro.
Cliii Chim Acta 1981;112:349-56.
8. Robertson WG, Scurr DS. Modifiers of calcium oxa]ate crystallization found in urine. I. Studies with a continuous crystallizer
using an artificial urine. J Urol 1986;135:1322-6.
9. Robertson WG, Scurr DS. Modifiers of calcium oxalate growth
found in urine. II. Studies on their mode of action in an artificial
urine. J Urol 1986;136:128-31.
10. Khan SR, Hackett RL. Role of organic matrix in urinary stone
formation: an ultrastructural study of crystal matrix interface of
calcium oxalate monohydrate
stones. J Urol 1993;150:239-45.
11. Fraij BM. Separation and identification of urinary proteins
and stone-matrix
proteins by mini-slab sodium dodecyl sulfatepolyacrylamide
gel electrophoresis. Clin Chem 1989;35:658-62.
12. Kumar S, Muchmore S. Tamm-Horsfall
protein-uromodulin
(1950-1990) [Review]. Kidney mt 1990;37:1395-401.
13. Williams J, Marshall RD, van Halbeek H, Vliegenthart JFG.
Structural analysis of the carbohydrate moieties of human Tamm-
Horsfall glycoprotem. Carbohydr Res 1984;134:141-55.
14. Afonso AMM, Charlwood PA, Marshall RD. Isolation
and
from digests of human TammRes 1981;89:309-19.
15. HArdK, van Zadeihoff G, Moonen P, Kamerling JP, Vliegenthart JFG. The Asn-linked carbohydrate
chains of human TammHorsfall glycoprotein of one male. Eur J Biochem 1992;209:895characterisation
of glycopeptides
Horafall glycoprotein. Carbohydr
915.
16. Fletcher
AP, Neuberger
A, Ratcliffe WA. Tamm Horsfall
glycoprotein. The chemical composition. Biochem J 1970;120:41724.
17. Rambausek
M, Dulawa J, Jann K, Ritz E. Tamm Horsfall
glycoprotein in diabetes mellitus: abnormal chemical composition
and colloid stabffity. Eur J Cliii Invest 1988;18:237-42.
18. Yoshioka T, Koide T, Utsunomiya M, It.atani H, Oka T,
Sonoda T. Possible role
oxalate crystallization.
19. Rose GA, Sulainian
calcium oxalate crystal
Urol 1982;127:522-4.
20. Grover PK Ryall
of Tamm-Horsfall
glycoprotein
in calcium
Br J Urol 1989;64:463-7.
S. Tamm-Horsfall
mucoproteins
formation in urine: quantitative
RL, Marshall
promote
studies. J
VR. Does Tamm-Horsfall
mucoprotein inhibit or promote calcium oxalate crystallization in
human urine? Clin Chim Acta 1990;190:223-38.
21. Hess B, Nakagawa Y, Coo FL. Inhibition of calcium oxalate
monohydrate crystal aggregation by urine proteins. Am J Physiol
1989;257:F’99-106.
22. Brielmann T, Hering F, Seiler H, Rutishauser G. The oxalate
tolerance value: a whole urine method to discriminate
between
calcium oxalate stone formers and others. Urol Res 1985;13:291-5.
23. Schnierle P, Sialm F, Seller H, Hering F, Rutishauser G.
Investigations on macromolecular precipitation inhibitors of calcium oxalate. Urol Res 1992;20:7-11.
24. Tamm I, Horsfall FL. Characterization and separation of an
inhibitor of viral hemagglutination
present in urine. Proc Soc Exp
Biol Med 1950;74:108-14.
25. Hamlin LM, Fish WW. Physical properties of Tamm-Horsfall
glycoprotein
and its glycopolypeptide.
mt J Pept Protein Res
1977;10:270-6.
26. Neuberger A, Ratdliffe WA. The acid and enzymic hydrolysis
of 0-acetylated
sialic acid residues from rabbit Tamm-Horsfall
glycoprotein. Biochem J 1972;129:683-93.
27. Horn D, Heuck CC. Charge determination of proteins with
polyelectrolyte titration. J Biol Chem 1983;258:1665-70.
28. Ainunoff D. Methods for the quantitative estimation of
N-acetylneurauninic acid and their application to hydrolysates of
sialomucoids. Biochem J 1961;81:384-92.
29 Schauer R. Chemistry, metabolism and biological functions of
sialic acids [Review]. Adv Carbohydr
Chem Biochem 1982;40:131234.
30. Spiro RG. Studies on fetuin, a glycoprotein of fetal serum. I.
Isolation, chemical composition and physicochemical properties. J
Biol Chem 1960;235:2860-9.
31. Chirgadze YN, Fedorov OV, Trushina NP. Estimation of
amino acid residue side-chain absorption in the infrared spectra of
protein solutions in heavy water. Biopolymers 1975;14:679-94.
32. Tipson RS, Parker FS. Physical methods for structural analysis: infrared spectroscopy. In: Pigman W, Horton D, Wander JD,
eds. The carbohydrates: chemistry and biochemistry. New York:
Academic Press, 1980:1394-436.
33. Kauppinen JK, Moffatt DJ, Mantsch HH, Cameron DG. Fourier self-deconvolution: a method for resolving intrinsically overlapped bands. App! Spectrosc 1981;35:271-6.
34. Byler DM, Susi H. Examination of the secondary structure of
proteins by deconvolved FTIR spectra. Biopolymers 1986;25:46987.
35 Malek RS, Boyce WH. Observations on the ultrastructure
and
genesis of urinary calculi. J Urol 1977;117:336-41.
36. Hession C, Decker JM, Sherblom AP, Kumar S, Yue RJ,
Mattaliano
RJ, et al. Uromodulin
(Taunm-Horsfall glycoprotein): a
renal ligand for lymphokines. Science 1987;237:1479-84.
37. van Aswegen CH, van der Merve CA, du Plessis DJ. Sialic acid
concentration in the urine of men with and without renal stones.
Urol Res 1990;18:29-33.
38. Scurr DS, Robertson WG. Modifiers of calcium oxalate crystallization found in urine. III. Studies on the role of TanimHorsfall mucoprotein and of ionic strength. J Urol 1986;136:505-7.
39. Edyvane KA, Hibberd CM, Harnett RM, Marshall VR, Ryall
RL. Macromolecules
inhibit
calcium oxalate crystal growth and
aggregation in whole human urine. Clin Chim Acta 1987;167:32938.
40. Storey EL, Anderson GJ, Mack U, Powell LW, Halliday JW.
Desialylated transferrin
as a serological marker of chronic excessive alcohol ingestion. Lancet 1987;i:1292-4.
41. Rademacher TW, Parekh RB, Dwek RA. Glycobio!or. Ann
Rev Biochem 1988;57:785-838.
42. Fukuda MN, Dell A, Scartezzin P. Primary defect of congenital dyserythropoietic anemia type II. Failure in glycosylation of
erythrocyte
lactosarnunoglycan
proteins
caused
by
lowered
N-acetylglucosaxninyltransferase
II. J Biol Chem 1987;262:7 195206.
43. Kornfeld S. Trafficking of lysosomal enzymes in normal and
disease states [Review]. J Clin Invest 1986;77:1-6.
44. Hess B, Nakagawa Y, Parks JH, Coo FL. Molecular abnormality of Tamm-Horsfall glycoprotein in calcium oxa]ate nephrolithiasis. Am J Physiol 1991;260:F569-78.
CLINICAL CHEMISTRY, Vol. 40, No. 9, 1994 1743