Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Circulation Research
JUNE
VOL. 44
1979
NO. 6
An Official Journal of the American Heart Association
SPECIAL ARTICLE
The Cardiac and Vascular Factors That
Determine Systemic Blood Flow
MATTHEW N. LEVY
Downloaded from http://circres.ahajournals.org/ by guest on April 30, 2017
THE CARDIOVASCULAR system is a closed circuit. At any given moment, the rate at which blood
returns to the heart from the venous system (venous
return) may differ considerably from the rate at
which the heart pumps it out into the arterial
system (cardiac output). Under steady state conditions, however, cardiac output (CO) and venous
return (VR) are virtually equal. Therefore, it probably is better not to distinguish between CO and
VR under such conditions, but simply to consider
the total blood flow (OJ around the circuit. There
has been a tendency on the part of some investigators to explain steady state changes in CO in response to certain conditions (e.g., blood loss, exercise, vasoactdve drugs) by invoking changes in VR.
Such an explanation is meaningless, however.
These conditions affect Q. for reasons that merit
analysis, and such changes in Q are, of course,
attended by equal changes in CO and VR at equilibrium. However, to explain the steady state
change in CO on the basis of a change in VR is a
patent example of circular reasoning; it is tantamount to explaining a change in Q on the basis of
a change in Q.
This paper will deal with the cardiac and vascular
factors that determine the rate of blood flow around
the circulatory system, principally under steady
state conditions. The following are some of the
salient questions to be addressed: What are the
factors responsible for the equality of VR and CO
at equilibrium? Is there one group of factors that
influences the heart to pump a certain level of CO,
and are these then the same factors responsible for
the VR? Or is a separate group of factors responsible
for the VR? Specifically, is the right atrial pressure
an important determinant of the VR, by virtue of
its being one of two critical factors in a hypothetical
From the Division of Investigative Medicine, M t Sinai Hospital, and
Case Western Reserve University, Cleveland, Ohio.
Supported by U.S. Public Health Service Grant HL 10961.
Address for reprints: Matthew N. Levy, M.D., Chief, Investigative
Medicine, Mt. Sinai Hospital, 1800 East 105th Street, Cleveland, Ohio
44106.
"gradient for venous return"? Or is the level of the
right atrial pressure simply the result, not the cause,
of a change in VR? Does the level of the right atrial
pressure have opposite effects on CO and VR?
Coupling of the Heart and Circulation
In the early investigations of the control of CO,
such as those of Frank (1895) and of Starling and
his collaborators (Patterson et al., 1914), the heart
was studied after it had been separated from the
vascular system. Such isolated heart preparations
permitted rigorous control of the experimental variables, and many basic mechanisms were elucidated. However, it became increasingly evident that
the vascular system interacts with the heart, and
that the control of CO is influenced substantially
by the characteristics of the blood vessels and of
the blood itself (i.e., its volume and viscosity). Much
of the work on the role of the vascular system in
the control of CO was done by Guyton and his
associates (Guyton, 1955; Guyton et al., 1955, 1957,
1973).
To analyze the functional coupling between the
heart and the blood vessels, a model will be used in
which the cardiovascular system has been reduced
to its simplest components. As shown in Figure 1,
the model consists of a pump, an elastic arterial
system, a peripheral resistance (R), and an elastic
venous system. The advantage of the simplified
model is the relative ease of analysis of the interactions among the components, thereby permitting
the elucidation of certain basic principles. For many
purposes (e.g., when there are substantial blood
volume shifts between the pulmonary and systemic
circuits), the model is much too simple and potentially misleading. For such purposes, more complicated models must be used, such as those developed
by Grodins and his coworkers (Grodins, 1959; Grodins et al., 1960), Sagawa (1972), and Guyton et al.
(1973).
The model of the cardiovascular system shown
in Figure 1 may be subdivided arbitrarily into car-
CIRCULATION RESEARCH
740
VOL. 44, No. 6, JUNE
1979
bottom half of the loop represent the vascular activity. A preliminary version of this block diagram
has been presented previously by Fennoso et al.
(1964), and a more detailed version has been developed by Grodins and his coworkers (Grodins, 1959;
GrodinsetaL, 1960).
Vein
Artery
1 Simplified model of the systemic circulation.
The coupling between the heart and the vascular system
consists of the right atrium (RA) and the aortic origin
(AO). Other abbreviations: R, systemic resistance; P w
central venous pressure; Pra, right atrial pressure; and
Pa, arterial pressure.
FIGURE
Downloaded from http://circres.ahajournals.org/ by guest on April 30, 2017
diac find vascular components. There are two sites
of coupling between these components; (1) the right
atrium serves to connect the terminal veins to the
input side of the pump, and (2) the aortic origin
serves to connect the output side of the pump to
the upstream end of the vascular system. From the
functional viewpoint, the pressures in the aorta (Pa)
and in the right atrium (Pr.) and central veins (Pv)
are the mechanical feedback signals that coordinate
the activities of these two principal components of
the cardiovascular system. In the model, the pressures in the right atrium and large veins are considered to be equal; i.e., P™ ~ Pv. The cardiac contraction tends to establish the prevailing levels of P,
and P v , which in turn are important determinants
of the rate of blood flow through the vascular system. Concomitantly, the characteristics of the vascular system tend also to determine the levels of P«
and Pv, which in turn critically affect the quantity
of blood to be pumped by the heart. Of course, in
the real cardiovascular system, there are many ways
in which the cardiac and vascular components may
interact with one another, other than simply by
virtue of the prevailing levels of P a and P v . Such
important reflex and humoral mechanisms will be
neglected in this discussion, and only the mechanical factors will be considered. The influence of the
modulating factors has been described in detail in
the monograph by Guyton et al. (1973).
The block diagram shown in Figure 2 will help to
outline the manner in which the two principal subunits of the simplified model of the cardiovascular
system interact mechanically with each other. The
blocks in the diagram constitute a feedback loop.
The block in the top half of the loop represents the
cardiac behavior, whereas the two blocks in the
The Cardiac Component
Skeletal muscle contraction, including that of the
respiratory muscles, may play a small role in propelling blood around the circulatory system. However, for all practical purposes, the heart must be
considered to be the energy source responsible for
pumping the total blood flow (Q) around the body,
regardless of whether that flow be denoted as CO
orVR.
Preload, afterload, cardiac contractility, and
heart rate usually are considered to be the factors
that determine the output of the heart. P ra and right
ventricular dimensions are the determinants of
right ventricular preload. Similarly, P a and left ventricular dimensions are the determinants of left
ventricular afterload. Hence, in the "cardiac function" block (A) in Figure 2, P« and P v are shown as
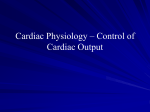
two critical inputs that tend to determine Q. The
response surface displayed in Figure 3 shows the
influence of these two factors on Q (Hemdon and
Sagawa, 1969). In general, Q varies directly with P v
and inversely with P a . Changes in either heart rate
or myocardial contractility result in a shift to a new
response surface.
The Vascular Component
When a fluid is pumped through a system of
tubes, the hydraulic equivalent of Ohm's law is:
Q. = (Pi - P 2 )/R,
(1)
where Q is the flow, R is the total resistance, and
(Pi - P2) is the pressure gradient across that resistance.
If the hydraulic system under consideration were
Q =f(P. ,P.,HR ,Cont)
CARDIAC
(A)
6
p.
A P.
AP,
=
"
C»
C.
VASCULAR
(C)
P.-P, = QR
P.-P. VASCULAR
(B)
2 Block diagram of the feedback loop involved
in the coupling of the cardiac and vascular portions of
the circulatory system. Abbreviations: 0, systemic flow;
Pa, arterial pressure; Pa venous pressure; HR, heart
rate; Cont, cardiac contractility; R, systemic resistance;
Co, arterial capacitance; and Cw venous capacitance.
FIGURE
CARDIAC OUTPUT REGULATION/Levy
741
°t.
4000
FIGURE 3 Response
surface,
showing the change in aortic
flow in an anesthetized dog as a
function of the mean arterial
pressure (MAP) and mean right
atrial pressure (MRAP) (from
Herndon and Sagawa, 1969,
with permission).
3OOO
20O0
Downloaded from http://circres.ahajournals.org/ by guest on April 30, 2017
1000
VJ
300
taken to be the systemic vascular system, the pressure gradient would be the arteriovenous pressure
gradient, P. - Pv. Substituting (P. - Pv) for (Pi P2) in Equation 1 and rearranging, we obtain
P. - P v
(2)
From this equation, it is apparent that the magnitude of the arteriovenous pressure gradient at equilibrium is determined by the peripheral vascular
resistance, R, and by the quantity of blood per
minute being pumped by the heart, Q. An increase
in Q would evoke a proportionate increase in the
gradient, and a decrease in Q would elicit a proportionate reduction in the gradient. Assuming a constant R for the present purpose, and given that the
energy source for the flow is derived from the
pumping action of the heart, we may consider Q to
be the independent variable (i.e., the input, or stimulus) in this relationship, and (P, — Pv) to be the
dependent variable (i.e., the output, or response).
Therefore, in block B of Figure 2, Q is shown as the
input variable to the block, and (P. — Pv) is shown
as the output variable.
The selection of the dependent and independent
variables is often arbitrary. For example, the energy
of cardiac contraction is involved in the development of pressure as well as flow. Therefore, for
other purposes, the opposite assignment of dependent and independent variables might have been
made. The problem of the optimal assignment of
variables is discussed in greater detail below.
The actual level of each of the two terms, P a and
Pv, of the pressure gradient that occurs with a given
change in Q (Equation 2) is determined by the
elastic characteristics of the systemic circulation
and by the blood volume. The arterial capacitance,
Ca, is defined as dV«/dP«, where V« and P« are the
blood volume and pressure, respectively, on the
arterial side of the circuit. Similarly, the venous
capacitance, Cv, is defined as dVv/dPv, where Vv
and P v are the venous volume and pressure, respectively. In our model (Fig. 1), let C« and Cv both be
constant, i.e., independent of both pressure and
volume. Under such conditions, it is also true that
C. = AV./AP., and Cv = AVV/APV.
In the model under consideration (Fig. 1), let the
changes in blood volume take place only in the
systemic arteries and veins. Given a constant total
blood volume,
AV - - A V .
(3)
Hence, any increment in V. is accompanied by an
equal decrement in Vv, or vice versa. But AV, — C«
• AP«, and AVV = Cv • APV. Substituting these values
in Equation 3 and rearranging, we obtain
AP./APv = -Cv/C
(4)
A simple example will illustrate how, with a
742
CIRCULATION RESEARCH
Downloaded from http://circres.ahajournals.org/ by guest on April 30, 2017
specific ratio of Cv/C«, a given change in (P. — Pv)
will produce specific changes in P, and Pv. For the
schema in Figure 1, let R = 20 mm Hg • min/liter,
let CV:C« = 19:1, and let Cv and Ca remain constant,
regardless of the levels of pressure and volume.
These values for R and the Cv:C, ratio are close to
the mean values for normal, resting adults.
Consider the system at first to be static; i.e., Q
= 0. At equilibrium, the pressures throughout the
system all will be equal. Guyton et al. (1973) have
termed this static pressure the "mean systemic
pressure," P™. This pressure depends on the total
blood volume and on the overall capacitance of the
systemic vascular system. Under normal conditions,
Pros is about 7 mm Hg (Guyton, 1955; Guyton et aL,
1957, 1973). For our model, therefore, let Pm, = 7
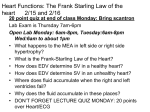
mm Hg. Also, because pressures are equal throughout the system, P« — P v = 7 mm Hg. A graph can be
constructed relating P« and Pv to Q (Fig. 4). Note
that point a on this graph has the coordinates (0, 7)
and represents the value of Pm,.
Consider next that the heart in this previously
static system begins to pump blood at a constant
rate of 1 liter/min. The equilibrium value for (P.
— Pv) may be computed from Equation 2:
P. - P v = 20 mm Hg.
(5)
This computation is represented by block B in
Figure 2. Clearly, the operation of the pump produces the flow of 1 liter/min throughout the systemic circulation. At equilibrium, VR and CO will
both equal 1 liter/min. This flow through the resistance of 20 mm Hg-min/liter is responsible for
the pressure gradient of 20 mm Hg. Stated in another way, Q is the independent variable for this
process, and (P, — Pv) is the dependent variable.
The individual values for P. and P v depend not
only on this gradient but also on P m and the ratio
of Cv:Ca. In our example, Pm, - 7 mm Hg, and C v /
Ca =• 19, as stated above. Therefore, from Equation
4:
AP./APv - -19.
(6)
Let APa = P. - P m , and let APV = P v - Pm. With
reference to Figure 4, AP. and APV represent the
deviations of P« and Pv, respectively, from P m , for
any given level of Q. By substitution of these values
for AP« and APV into Equation 6:
-19(P (7)
P. By solving simultaneous Equations 5 and 7, it is
found that P, = 26 and P v •= 6. Note that the process
by which the individual values for P, and P v are
derived from the value for the arteriovenous pressure gradient is represented by block C in Figure 2.
Note also that the points with coordinates (Q •• 1,
P a = 26) and (Q =» 1, P v = 6) appear as points b and
c, respectively, in Figure 4.
Finally, let the heart begin to pump blood at a
constant rate of 5 liters/min. By the same analytical
VOL. 44, No. 6, JUNE 1979
100 P.
80
>
irnHg
60 40-
(pa-p.)
b/
20 -
ft
P.
y
Pm.
»p.
p,
mmHg
1
0
1
2
3
4
6 (l/min)
1 ^ ^
5
6
FIGURE 4 The values of arterial pressure (Pa) and
central venous pressure (Pu) as functions of the systemic
flow (0) in the model depicted in Figure 1, where R — 20
and CJCa — 19. Point a denotes the value of the mean
systemic pressure (Pms), i.e., the common value for Pa
and Pv when 0 = 0. Points b and c denote the values of
Pa and Po when 0 — 1, and points d and e, the values of
Pa and Pv when 0 = 5. The deviations ofPa and Pv from
P*, are denoted by APO and APD, respectively. Note that
the scales for Pa and Pu are not the same.
process, P a - P v = 100 mm Hg (block B, Fig. 2),
and P, and P v = 102 and 2 mm Hg, respectively
(block C, Fig. 2). Note that points d and e in Figure
4 have the coordinates (Q = 5, P. = 102) and (Q =»
5, P v = 2), respectively.
The Closed Circulatory Loop
The heart and blood vessels operate in the circulatory system as an integral unit, and the function
of either component is affected by the other. The
heart provides virtually all of the energy for the
circulation of the blood through the vascular system. It therefore is responsible for total Q around
the circuit, whether that flow be called "cardiac
output" or "venous return." The magnitude of Q is
determined by a variety of factors, including P. and
Pv (block A, Fig. 2).
P, and Pv, in turn, are determined not only by
the operation of the heart itself but, also, by certain
critical characteristics of the vascular bed. Q and R
determine the arteriovenous pressure gradient
(block B), and the total blood volume and vascular
capacitances determine the actual levels of P. and
Pv (block C). Thus P, and P v are determinants of
Q by virtue of their influences on the heart, and Q
743
CARDIAC OUTPUT REGULATION/Lei/y
is a determinant of P. and P v by virtue of its
interaction with the vasculature. The equilibrium
values of Q., P«, and P v constitute the solution of
the simultaneous equations represented by the
three blocks in Figure 2. The value of P™, which
depends in part on the blood volume, is a boundary
condition for the equation represented by block C.
Interrelations between CO and P,,
Downloaded from http://circres.ahajournals.org/ by guest on April 30, 2017
A complicated, three-dimensional graph (Fig. 3)
is necessary to depict the simultaneous influences
of P. and P v on the pumping capabilities of the
heart (block A, Fig. 2). The functions represented
by blocks B and C in Figure 2 could be represented
by other response surfaces. For a given set of conditions, the equilibrium values for P«, Pv, and Q.
would be represented graphically by the point of
intersection of these three response surfaces. Sagawa (1973) has shown that the equilibrium value
also may be represented by the intersection of the
three-dimensional response surface for CO (Fig. 3)
with a curve in space that represents the vascular
components of the system.
Guyton and his coworkers (Guyton, 1955; Guyton
et al., 1973) have developed a simpler graphical
analysis, in which the interrelations are plotted
between just two of these variables, P v and Q. Two
separate sets of relationships have been delineated,
as shown in Figure 5. Curve A has been called a
"cardiac output curve," and curve B a "venous
return curve." Unfortunately, these designations
tend to be ambiguous because they each represent
the flow around a closed circuit, and, except for
transient influences, any factor that affects CO has
an equal effect on VR, and vice versa. For this
reason, and for others to be cited below, I suggest
substituting the terms "cardiac function curve" and
"vascular function curve" for curves A and B, respectively, in Figure 5. These terms stress the applicability of the respective curves to the cardiac
and vascular components of the cardiovascular system.
The cardiac function curve represents the FrankStarling mechanism. This curve (or, more precisely,
the response surface as shown in Figure 3) describes
the behavior of the heart specifically and is independent of the nature of the vascular system. Indeed, the original studies by Starling and his collaborators were done on isolated heart-lung preparations (Patterson et al., 1914); the systemic circulation was eliminated. The cardiac function curve
depicts the systemic flow (Q) pumped by the heart
as a function of Pv; i.e., P v is the independent
variable and Q. the dependent variable. In accordance with the usual convention, P v is plotted along
the abscissa and Q. along the ordinate. This curve
will be shifted downward by a decrease in contractility or by an increase in afterload and will be
shifted upward by the opposite changes in contractility and afterload. A given cardiac function curve
tARDIAC
FUNCTION
Q
(l/min)
VASCULAR
FUNCTION
Pv (mmHg)
5 The cardiac function curve (A) expresses
how systemic flow (Q) changes as a function of the
central venous pressure (Pv); it represents the FrankStarling mechanism. The vascular function curve (B)
expresses how Pv changes as a function of 0. Note that,
for curve A, Pv is the independent variable and 0 the
dependent variable; for curve B the opposite is true.
FIGURE
represents the intersection of the response surface
in Figure 3 with the vertical plane, parallel to the
MRAP axis, that represents the prevailing arterial
pressure. With respect to the block diagram in
Figure 2, the cardiac function curve represents the
operation of block A.
The vascular function curve (B, Fig. 5) depends
on blood volume, peripheral resistance, venomotor
tone, and vascular compliance, as shown by Guyton
and his coworkers (Guyton, 1955; Guyton et al.,
1955, 1957, 1973) in an extensive series of studies.
Because the curve does depend in part on blood
volume, "hemovascular function curve" would be a
more comprehensive, but a more cumbersome, designation, and therefore will not be used herein. The
vascular function curve is independent of the characteristics of the heart; it may be derived experimentally by totally replacing the heart by an artificial pump. Guyton and his collaborators designated this curve the "venous return curve," because
they considered that P™ is an important determinant of VR. Hence in their plots P v was considered
to be the independent variable and Q the dependent
variable. From their viewpoint, plotting Pv along
the abscissa and Q. along the ordinate, as in Figure
5, would conform to the usual convention.
It may be questioned, however, whether the identification of P v as the independent variable and Q.
as the dependent variable for curve B is the most
judicious selection. The development of a mathematical model is an abstraction, and hence the
assignment of dependent and independent variables
may be arbitrary. If the model is devised to improve
our understanding of a specific problem, however,
the optimal designation of dependent and indepen-
744
CIRCULATION RESEARCH
Downloaded from http://circres.ahajournals.org/ by guest on April 30, 2017
dent variables may be critical, because it usually
implies a certain relationship between cause and
effect. With respect to the two variables that are
related by curve B (Fig. 5), for example, the choice
of designations involves the question of whether a
change in P v is an important cause of a change in
VR or the result of some change in Q around the
circuit.
Guyton and his associates (Guyton, 1955; Guyton
et al., 1973) consider that small changes in Pv may
have enormous effects on VR. They argue that the
difference between Pms and P ra is the "pressure
gradient for venous return." Pms is a weightedaverage pressure and equals the static pressure for
the systemic circulation, as stated above. Normally,
P ms is about 7 mm Hg, and P ra is only slightly less
than that. Therefore, Guyton and his collaborators
have reasoned that a rise in P ra of only about 5 mm
Hg would halt VR and reduce Q to zero, if Pms were
held constant.
The theoretical analysis presented above and
summarized in Figure 4 suggests that the level of
P v (or Pra) is actually a consequence of the rate of
Q around the circuit. It is, of course, also a determinant of Q, but principally through its effect on
the filling of the heart (block A, Fig. 2). It probably
is not an important determinant of "venous return"
by virtue of any "back-pressure" effects. A rise in
P v of only a few mm Hg would reduce the (Pa — Pv)
gradient only slightly at normal levels of P a . From
Equation 2, therefore it would be expected that a
small reduction in the pressure gradient per se
would produce only a small, proportionate reduction in Q. With respect to the hypothetical "pressure gradient for venous return" (i.e., Pv — Pms),
Figure 4 does indeed show that 0 and (Pv — Pms)
are proportional to each other. However, the theoretical analysis indicates that any change in P v —
Pms was evoked by a change in Q, and not the
converse. Stated in another way, Pv — Pms represents a "pressure gradient caused by flow," rather
than a "pressure gradient for venous return."
Guyton et al. (1957, 1973) conducted a series of
experiments on the mechanical factors that control
VR. They used a right-heart bypass preparation, in
which all of the VR to the right atrium was pumped
mechanically into the cannulated pulmonary artery; i.e., an artificial pump replaced the right ventricle. Thin, collapsible tubing was included in the
line between the right atrium and the pump, and
the pump was adjusted to keep the tubing in a
"semi-collapsed condition." To produce new values
of Pra and Q, the hydrostatic level of the collapsible
tubing was changed and the pump was readjusted
to produce the same semicollapsed state in the thin
tubing.
Raising the level of the collapsible tubing and
decreasing the pumping rate until the thin tubing
returned to the semicollapsed state resulted in an
elevation of P ra and a decline of Q. The investigators
(Guyton et al., 1957, 1973) asserted that the col-
VOL. 44, No. 6, JUNE
1979
lapsible tubing permitted direct control of the level
of P ra , and that the changes in Q were a consequence
of the experimentally induced change in P ra . Hence,
they identified P ra as the independent variable
("stimulus") and Q as the dependent variable ("response"). However, the necessity of adjusting both
the level of the collapsible tube and the pumping
rate prior to making a measurement did introduce
ambiguity in the identification of the independent
and dependent variables. Did adjustment of the
height of the collapsible tube set the level of Pra,
which then determined the rate of VR, or did adjustment of the pumping rate (Q) produce the resultant level of Pra?
These experiments on the right-heart bypass
preparation recently were repeated in our laboratory in an open-chest, anesthetized dog. A roller
pump was used to transport the blood returning to
the right atrium into the pulmonary artery over a
range of pumping rates. The only critical difference
in our experimental system from that of Guyton
and his coworkers was that the collapsible tube was
excluded. As stepwise changes were made in the
pumping rate (Q), there were parallel alterations in
Pa, but there were concomitant, inverse changes in
P v and P ra , as shown in Figures 6 and 7. Similar
results have been reported previously by Grodins et
al. (1960) in a group of eight dogs.
Elimination of the collapsible tubing in the experiment shown in Figures 6 and 7 and in the
experiments by Grodins and his collaborators
averted the ambiguity in the identification of the
independent and dependent variables. The pumping rate was the factor that was altered experimentally; hence, Q was the independent variable, by
definition. Changes in Q evoked changes in P a and
Pv, which then constituted the dependent variables.
A series of experiments also was carried out by
Guyton (1955) on a total heart bypass preparation.
A collapsible tube was not included in the experimental design. Changes in Q produced by the arti-
6 The changes in arterial (Pa) and central
venous (Pv) pressures produced by changes in systemic
blood flow (Q) in a canine right-heart bypass preparation. Stepwise changes in Q were produced by altering
the rate at which blood was mechanically pumped from
the right atrium to the pulmonary artery.
FIGURE
CARDIAC OUTPUT REGULATION/Leuy
745
vasculature. Hence, the graphs of Pv as a function
of Q (Figs. 4 and 7) reflect the influence of blood
volume and certain critical vascular factors on the
prevailing flow rate to produce a specified level of
Pv. They do not represent the effect that a change
in Pv will have on Q. Therefore, it is preferable that
such curves be called "vascular function curves,"
rather than "venous return curves."
100 -
mmHg
Graphic Analysis of CO Control
mmHg
Downloaded from http://circres.ahajournals.org/ by guest on April 30, 2017
Q
(l/min)
7 Graphs of arterial (Pa) and central venous
(Pv) pressures as functions of the systemic blood flow
(Q) for the experiment shown in Figure 6. Note that the
scales for Pa and Pv are not the same. Pms is the mean
systemic pressure, i.e., the value of Pa and Pv that prevails when Q = 0.
FIGURE
ficial pump that replaced the heart were associated
with inverse changes in Pv. The change in Q was
initiated by the investigator (Guyton, 1955), and
the inverse change in P v was the response noted in
the animal. It is apparent, therefore, that the
change in P v was a consequence of the experimentally induced change in Q.
Note that the experimental data plotted in Figure
7 are qualitatively similar to those derived theoretically in Figure 4. The curves that represent the
experimentally derived levels of P a and P v as functions of Q are not linear, principally because Ca, Cv,
and R are not constants in vivo, as they were
assumed to be in the model. Also, the level of Pms
was abnormally high, principally because of overhydration and reflexly induced venoconstriction.
Directionally, however, changes in Q evoked concordant changes in P a and inverse changes in Pv,
just as in the theoretical model. Similar results have
also been obtained by Grodins et al. (1960). Although the data in individual animals were nonlinear in their experiments, the composite data for the
group of eight animals indicated that P a and P v
were virtually linear functions of Q.
The experimentally derived plot of P v as a function of Q (lower half of Fig. 7) may be considered to
reflect the interaction between the vascular factors
and the flow generated by the pump. With reference
to Figure 2, this graph represents the actions of
blocks B and C on Q; that is, with a given flow, a
certain level of P v will be achieved, depending on
the blood volume and the characteristics of the
Guyton and his coworkers (Guyton, 1955; Guyton
et al., 1973) made a monumental contribution to
the analysis of cardiovascular control by showing
that, at equilibrium, the levels of CO and P ra are
defined by the point of intersection of the two
independent curves shown in Figure 5. The cardiac
function curve (A) depicts the systemic flow (Q)
pumped by the heart as a function of P ra or Pv; i.e.,
P v is the independent variable and is plotted along
the abscissa, whereas Q is the dependent variable,
and is plotted along the ordinate, in accordance
with convention.
The vascular function curve (B, Fig. 5) depends
on blood volume, peripheral resistance, venomotor
tone, and vascular compliance, as shown by Guyton
and his coworkers (Guyton, 1955; Guyton et al.,
1973). According to the arguments presented above,
it reflects how these characteristics of the vascular
system produce a certain value of P v for a given
level of Q. Hence, for curve B (Fig. 5), Pv and Q are
the dependent and independent variables, respectively. To include this curve and curve A on the
same set of axes, the usual plotting convention must
be reversed for one of these curves. The axes have
arbitrarily been reversed for the vascular function
curve.
To interpret the interactions between these two
functions properly, curve A must be considered to
represent the level of Q that would prevail at a
given level of Pv, and curve B to reflect the level of
P v that would prevail at a given level of Q. At
equilibrium, only one pair of values of P v and Q
satisfy the two relationships. This pair of values are
the coordinates of the point of intersection of the
two curves, as originally enunciated by Guyton and
his colleagues (Guyton, 1955; Guyton et al., 1973).
After a transient perturbation, the levels of Pv and
Q may deviate temporarily from their equilibrium
values. However, given a constant state of the heart
and vasculature, the levels of P v and Q would approach that same equilibrium value in a series of
diminishing steps. Each step would involve the
processes represented by a complete circuit of the
feedback loop shown in Figure 2.
References
Fermoso JC, Richardson TQ, Guyton AC: Mechanism of decrease in cardiac output caused by opening the chest. Am J
Physiol 207: 1112-1116, 1964
Frank 0: Zur Dynamik des Herzmuskels. Z Biol 32: 370-437,
1895
746
CIRCULATION RESEARCH
VOL. 44, No. 6, JUNE 1979
Downloaded from http://circres.ahajournals.org/ by guest on April 30, 2017
Grodins FS: Integrative cardiovascular physiology: A mathematical synthesis of cardiac and blood vessel hemodynamics.
Q Rev Biol 34: 93-116, 1959
Grodins FS, Stuart WH, Veenstra RL: Performance characteristics of the right heart bypass preparation. Am J Physiol 198:
552-560, 1960
Guyton AC: Determination of cardiac output by equating venous
return curves with cardiac response curves. Physiol Rev 35:
123-129, 1955
Guyton AC, Lindsey AW, Kaufmann BN: Effect of mean circulatory filling pressure and other peripheral circulatory factors
on cardiac output. Am J Physiol 180: 463-468, 1955
Guyton AC, Lindsey AW, Abernathy B, Richardson T: Venous
return at various right atria] pressures and the normal venous
return curve. Am J Physiol 189: 609-615, 1957
Guyton AC, Jones CE, Coleman TG: Circulatory Physiology:
Cardiac Output and Its Regulation, ed 2. Philadelphia, WB
Saunders, 1973
Hemdon CW, Sagawa K: Combined effects of aortic and right
atrial pressures on aortic flow. Am J Physiol 217: 65-72, 1969
Patterson SW, Piper H, Starling EH: The regulation of the heart
beat. J Physiol (Lond) 48: 465-513, 1914
Sagawa K: The use of control theory and systems analysis in
cardiovascular dynamics. In Cardiovascular Fluid Dynamics,
vol 1, edited by DG BergeL London, Academic Press, 1972, pp
116-171
Sagawa K: The circulation and its control. I: Mechanical properties of the cardiovascular system. In Engineering Principles
in Physiology, vol 2, edited by JHU Brown, DS Gann. London,
Academic Press, 1973, pp 49-71
Editors' note: Dr. Arthur Guyton was one of
the referees for this Special Article. He provided the following comments, which were
judged to merit publication:
variables listed above then also become dependent
variables.
On the other hand, it often is very useful in
analyses of the circulation to set up "what if" types
of function curves. In our own early analyses we
asked ourselves the two questions: (1) What would
happen to cardiac output if the venous pressure
changed through a range of values? (2) What would
happen to venous return if the venous pressure
changed through the same range of values? Then,
using the two derived curves, we were able to show
that the point of intersection defines both the cardiac output and the right atrial pressure at the same
time, neither one of these two being an independent
variable but instead both being dependent variables. On the other hand, we could equally as well
have constructed these same two curves by asking
the following two questions: (1) What would happen
to the venous pressure if the cardiac output increased from zero up to and above the normal
operating level? (2) What would happen to the
venous pressure if the systemic blood flow changed
through a range of values from zero up to and above
the normal operating level? If we had analyzed
cardiac output and systemic venous pressure using
these two questions, the analysis would have
worked out to be exactly the same. However, in
using these two separate approaches to cardiac
output analysis, in one instance we make the theoretical assumption that the systemic venous pressure is an independent variable and that cardiac
output (and venous return, which is equal to cardiac
output) is the dependent variable. In the other type
of analysis we make the assumption that cardiac
output (and venous return) is the independent variable and systemic venous pressure is the dependent
variable. However, in the actual circulation, neither
of these two theoretical assumptions for independence holds true. Instead, both the cardiac output
and the systemic venous pressure are dependent
variables.
The second semantic point on which I might
differ with Dr. Levy is on the use of the terms
"cardiac function curve" and "vascular function
This paper by Dr. Levy shows a high degree of
insight into the interrelationships between cardiac
and peripheral vascular factors for determining
overall function of the circulation. It is clear from
the paper that most of the concepts presented are
similar to those that we have discussed in previous
papers, but with the addition of new ways of looking
at the problem. Having worked in this field for a
number of years, I find myself in complete agreement with Dr. Levy on all but two minor points,
neither of which is important conceptually and both
of which justify discussion only from a semantic
point of view. These are:
First, Dr. Levy has suggested that, in the analysis
of the venous return curve, venous pressure is a
dependent variable and venous return is an independent variable. I agree wholeheartedly that venous pressure is a dependent variable. However, I
would not quite agree that venous return is an
independent variable, but instead is just as much a
dependent variable as is venous pressure. This lack
of independence becomes especially clear when one
develops a relatively complete mathematical model
of the circulation and then runs the model on a
computer (Guyton et al., Annu Rev Physiol 34: 1341, 1972). One immediately finds that both venous
pressure and venous return are dependent variables. When one considers the mechanics of the
circulation (leaving out reflexes, hormonal factors,
and so forth), the independent variables are such
factors as resistance and capacitance of each segment of the circulation, contractility of the heart,
heart rate, and so forth. On the other hand, there is
no possible way in such a model to make venous
return, cardiac output, venous pressure, or arterial
pressure independent variables. Instead, all of these
are dependent on the independent variables listed
above. When one considers the reflexes and the
hormones as welL even some of the "independent"
COMMENTS ON SPECIAL ARTICLE
Downloaded from http://circres.ahajournals.org/ by guest on April 30, 2017
curve." Actually, in several editions of my Textbook
of Medical Physiology (W.B. Saunders Co., 1966
and 1971), I used the terms "cardiac function curve"
and "systemic function curve." The term "systemic
function curve" was used instead of Dr. Levy's more
encompassing "vascular function curve" to delineate the fact that the systemic circulation and the
pulmonary circulation are different vascular elements. However, in using these two terms I found
that they created confusion because there are many
other types of cardiac function curves and many
other types of systemic function curves. Therefore,
from experience in teaching this subject to students,
I found it much better to use more specific terms,
which explains why I prefer to use the terms "cardiac output curve" and "venous return curve."
When I chose to use these more specific terms, I
also consciously remembered a dictum from my
writing course in the University that whenever several alternative terms might be used, the more
specific one almost always has a more definitive
meaning and is more useful in discussions. This has
747
been my experience after an unsuccessful period of
using the more general terms which were almost
identical to those that are now suggested by Dr.
Levy. Therefore, I hope that we can stick to the
more specific terms, even though I have no conceptual disagreement with the less specific terms.
In any event, the terms and the different analytical approaches are merely tools to help us understand more fully the basic function of the circulation. What is truly important is the conceptual
framework that Dr. Levy has presented in this
paper, and also, I hope, the slightly different framework that we have attempted to present in the past.
The subject of cardiac output regulation is so important that all possible analytical approaches to
its understanding deserve widespread support and
exploration.
Dr. Arthur C. Guyton
Department of Physiology and Biophysics
University of Mississippi Medical Center
Jackson, Mississippi 39216
The cardiac and vascular factors that determine systemic blood flow.
M N Levy
Downloaded from http://circres.ahajournals.org/ by guest on April 30, 2017
Circ Res. 1979;44:739-747
doi: 10.1161/01.RES.44.6.739
Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1979 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7330. Online ISSN: 1524-4571
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circres.ahajournals.org/content/44/6/739.citation
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further information
about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation Research is online at:
http://circres.ahajournals.org//subscriptions/