Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
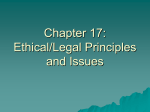
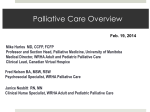
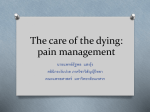
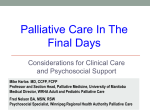
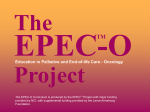
Care for the Dying Patient: Common Symptoms at End of Life Lisa Marr, MD (Devon Neale, MD) Palliative Medicine Palliative Care and Hospice Life Prolonging Care Hospice Care Palliative Care Objectives • Understand prevalence and pattern of symptoms near the end of life • Present management recommendations (with evidence base, such as it is…) • Provide practical tips to improve care of patients and families in last days of life What is a good death? What is a good death? Steinhauser et al. Factors considered important at the End of Life by Patient, Family, Physicians, and Other Care Providers. JAMA 2000. Evidence for Care at End of Life • Large trials (e.g. SUPPORT) or surveys describing symptom prevalence and patient desires • Rest of literature mostly small, single-site case series or trials – mostly in cancer patients • Evidence for most practices is quite poor, often anecdotal Preparing for the last hours of life • Regularly review the plan of care: prepare the family – Time course unpredictable – Signs /symptoms to expect, management plan • Any setting that permits privacy, pt goals • Anticipate need for medications, equipment, supplies Predicting Death • Most difficult and one of the most crucial parts of our job in caring for people near end of life • Allows patients / families to plan and make decisions • Important that consistent message from all member of the team The Reality of the Last Years of Life: Death Is Not Predictable 100 CANCER CHF, dementia Function 80 60 40 20 0 Time (slide courtesy of Joanne Lynn, MD, Rand Health) Signs Associated with Actively Dying Cancer Patients • Patient becomes bedbound • Patient is semi-comatose • Patient able to take only sips of fluid • Patient no longer able to take oral meds J Ellersaw and C. Ward. Care of the dying patient: the last hours or days of life. BMJ. 2003. 326:30-34. Data from: Morita et al. A prospective study on the dying process in terminally ill cancer patients. Am J Hosp Pall Care. 1998. Multivariable Models for Very Sick Patients Cannot Predict Time of Death Precisely (from SUPPORT)* Median 2-month Survival Estimate 1.0 0.8 Congestive heart failure 0.6 0.4 Lung cancer 0.2 0.0 7 6 5 4 Days before Death 3 *Lynn et al. New Horizons 1997;5:56-61. 2 1 Signs Associated with Actively Dying in Patients with Heart Failure • Previous admission with worsening heart failure • No identifiable reversible precipitant • Receiving optimum tolerated conventional drugs • Deteriorating renal function • Failure to respond within two to three days to appropriate changes in diuretics or vasodilator drugs J Ellersaw and C. Ward. Care of the dying patient: the last hours or days of life. BMJ. 2003. 326:30-34. Physiologic changes during the dying process • • • • • • • Increasing weakness, fatigue Decreasing appetite / fluid intake Decreasing blood perfusion Neurologic dysfunction Pain Loss of ability to close eyes Respiratory changes: dry mouth Conill et al. Symptom Prevalence in the Last Week of Life. Jnl Pain Symptom Manaage. 1997 Weakness / fatigue • Decreased ability to move: “withdrawing” – Listen to their body – don’t need OOB to chair, PT • Joint position fatigue: passive movement – Rarely in last hrs – days • Increased risk of pressure ulcers – Balance preventing / causing disturbance Decreasing appetite / food intake • Fears: “giving in,” starvation • Reminders – listen to their body: it’s telling them what they need and can “process” – food may be nauseating – risk of aspiration and vomitting – clenched teeth express desires, control • Help family find alternative ways to care – What is calming to pt: music, touch, reading, story-telling – Oral care Decreasing fluid intake . . . • Fears: dehydration, thirst – One study examining thirst showed no relationship with BUN/Cr, Na, osmolality, and ANP • Remind families, caregivers – dehydration does not cause distress – dehydration may be protective (endorphins) • Parenteral fluids may be harmful – fluid overload, breathlessness, cough, secretions, ascites, edema Morita et al. Determinants of the sensation of thirst in terminally ill cancer patients. Supportive Care Cancer, 2001. Dry Mouth • Dry mouth is one symptom which increases near end of life – experienced by > 60% of patients at end of life • What do you do to treat dry mouth? Morita et al. Determinants of the sensation of thirst in terminally ill cancer patients. Supportive Care Cancer, 2001. Oral Care: • Teach RN and family • Mouth swabs: NOT GLYCERIN • Artificial saliva or water • Petroleum jelly to lips q2h: NOT WATER • Topical nystatin for oral candidiasis Decreasing blood perfusion • • • • Tachycardia, hypotension: stop monitoring Peripheral cooling, cyanosis Mottling of skin Diminished urine output Parenteral fluids will not reverse Neurologic dysfunction • Decreasing level of consciousness • Communication with the unconscious patient • Terminal delirium • Changes in respiration • Loss of ability to swallow, • Loss of sphincter control Communication with the unconscious patient . . . • Awareness > ability to respond – Assume patient hears everything • Create familiar, calming environment • Include in conversations – assure of presence, safety • Touch, hold hand • Give permission to die Family Giving Permission to Die “Patty and Jacob and Denise and I are all here with you. We are going to take care of each other, we will be OK. It’s OK to go” 2 Roads to Death • “Usual” – Sleepy Lethargic Obtunded Comatose Death • “Difficult Road” – Restless Confused Tremulous Hallucinations Delirium Myoclonic Jerking Seizures Death Delirium at End of Life • Most prevalent symptom • Studies report rates as high as 88% for patients in final days • May be frightening to patients and family, “premature separation” for family Kaplan-Meier plot of patient survival in 104 cancer patients Prospective trial of patients with advanced cancer admitted to inpatient palliative care unit – cases and control both have advanced cancer – delirium diagnosis is at any point during admission. Lawlor, P. G. et al. Arch Intern Med 2000;160:786-794. Copyright restrictions may apply. To work up or Not to work up? • Delirium reversible in 50% of cases at end of life – i.e. not always curable, but treating some underlying causes may improve other symptoms (pain, urinary retention) and decrease severity of delirium symptoms • Pain, dyspnea, anxiety, ADE to medication (atropine, benzo, anti-histamine) Medications for Delirium at EOL • Best known randomized controlled trial – looking at chlorpromazine vs. lorazepam vs. haloperidol in AIDS patients • Admitted non-delirious patients and followed prospectively for development of delirium • Lorazepam arm stopped early because of increased agitation Breitbart et al. A double blind trial of haloperidol, chlorpromazine and lorazepam in the treatment of delirium in hospitalized AIDS patients. Am J Psychiatry. 1996 Treating Terminal Delirium • Family needs support, education • Nonpharm management: – Environment • Decrease irritating stimuli; Vitals, monitors, alarms, foley?, nebs? IV? • Increase familiar / pleasant surroundings – Voice, Re-orientation, touch – Day – Night cycle maintenance Treating Terminal Delirium • Medical management – Neuroleptics • Start treatment EARLY • Haloperidol: oral concentrate, IV, SC • Haldol 0.5mg PO / IV q6h, titrate up as needed – Sometimes add Benzodiazepine • Ativan: dose finding (0.5mg IV) then prn or standing / infusion • Can have paradoxical effect, monitor closely Death Rattle • What is death rattle? Death Rattle • What is death rattle? • Two types— 1. Normal salivary / bronchial secretions which can’t be expectorated due to weakness/fatigue/loss reflexes 2. Respiratory secretions due to underlying lung pathology #1 can be easily treated, #2 can’t be DR Prevalence and Prediction • High prevalence rates – 45-92% in the literature • Studies indicate it is the most uncontrolled “symptom” • Sign that death is imminent – – One retrospective study in Belgium of patients on pall care unit 48% developed DR within 24 hours of death 76% developed DR within 48 hours of death Wildiers and Menten. Death Ratle: Prevalence, Prevention, and Treatment. JPSM. 2002. 23 (4): 310-317. Ellershaw et al. Care of the Dying Patient: Setting Standards for Symptom Control in the Last 48 hours of Life Jnl Pain Sympt Manage. 2001. Medications • Scopolamine, Glycopyrrolate, Atropine, Hyoscyamine • Multiple trials for scopolamine vs. glycopyrrolate • None for atropine or hyoscyamine Scopolamine vs. Glycopyrrolate • Most trials done in Britain with both SQ • Good evidence to show scopolamine is better than glycopyrrolate both in terms of decreased DR, rapid onset, favorable side effects – but more expensive Beck et al. A study comparing hyoscine hydrobromide and glycopyrrolate in the treatment of death rattle. Palliative Medicine. 2001 Bennet et al. Using anti-muscarinic drugs in the management of death rattle: evidence-based guidelines for palliative care. When to Give Meds for DR • Try repositioning, turn partially to side • DO NOT give to prevent death rattle. Thickened secretions more difficult to expectorate for pt with intact reflexes • Give when you begin to hear secretions accumulating. Meds don’t remove secretions, just decrease rate of production • Explanation to family is key – No evidence it is distressing to pts – They are NOT DROWNING Pain • What is the prevalence at the end of life? • Common management techniques • Side effects to watch for SUPPORT: Patients who Experienced Moderate or Severe Pain at Least Half of the Time Within Their Last Few Days 50% SUPPORT Investigators. SUPPORT: A Controlled Trial to Improve Care for Seriously Ill Hospitalized Patients. JAMA 1995. Use of opioids at end of life • Standard pain management: – Dose finding – Basal level of pain medication – Episodic dosing (breakthrough / incident pain) – Least invasive means of administration (never IM) Differences at end of life: Specifics for prn • Before changing soiled pads / linens • Signs of pain: consistent grimacing, guarding • When family feels pt looks “UNCOMFORTABLE” Renal failure: accumulation of metabolites • Preferred medications: dilaudid, fentanyl • Dose reduction, discontinuation of basal • Check for myoclonus (risk of seizure) – Dose reduction, Opioid switching – Add benzodiazepine Other medications • Acetaminophen: Mild pain • Lidocaine (jelly with dressing, patch) – Neuropathic pain • Nsaids: Bone Pain • Steroids: – Capsular distension – Decrease size of large mass – Neuropathic pain FEARS Do opioids used in patients with advanced disease hasten death? • Secondary analysis of National Hospice Outcomes Project prospective cohort of patients in 13 facilities – 725 patients who had at least one opioid dose change prior to death. – Outcome = time until death after last dose change. – No association between % dose change and time until death. – There was an association between shorter survival and higher final opioid dose (p=.010), but accounted for at most 10% of the variance. Portenoy R. et al. Opioid use and survival at the end of life: a survey of a hospice population. Journal Pain Symptom Management 2006: 32; 532-540. Double-Effect • It is legal and ethical to use a medication / procedure that may decrease time to death WHEN the primary intent of use is to treat symptoms / improve QoL Dyspnea Near End of Life Prevalence anywhere from 22%-61% • Can be difficult to know if respiratory changes result from dyspnea, pain, agitation, or response to changes in metabolic acidosis • Ask family “Do they look uncomfortable to you?” Management of Dyspnea • • • • • Etiology: fluid overload, obstruction by mass Good air circulation, fans, cool room temp Repositioning Managing anxiety Low dose opioids: starting ½ analgesic dose – Modulation of sense of breathlessness (mu effect on CNS processing of stimulation of J-recepters in lung) – Titrate to . . . . ? Opioids for Dyspnea • Titrate to: “Comfortable breathing” – Subjective report of pt – Evaluation of observer / family • Treatment of: – Gasping respirations – Accessory muscle use – Appearance of “respiratory distress” – Rapid shallow breathing • Tachypnea is not necessarily dyspnea “Hold for respiratory rate <6” “Hold for respiratory rate <6” • The process of dying involves cessation of breathing • Discuss with nurse and family: – Patient is dying, eventually will stop breathing – We are treating discomfort and shortness of breath with opioids to prevent suffering during process of dying. “Terminal Sedation” • Sedating patients at end of life is rarely needed for control of symptoms. – Explore symptoms, multi-modal management – Expert palliative input • Usually barbituate or benzo drip, – – – – Start very low dose Titrate to lowest dose that causes unconciousness Do not stop other meds (pain meds) After 48h, decrease sedation, attempt communication to ensure symptoms were well managed. Terminal Sedation • One secondary data analysis of a trial of patients admitted to an inpatient palliative care unit examining use of medications for sedation showed no difference in survival Morita et al. Effects of high dose opioids and sedatives on survival in terminally ill cancer patients. J Pain Sympt Manage. 2001 Very Different From Euthanasia • Goal is alleviation of symptoms, not hastening death • One secondary analysis of a trial of patients admitted to an inpatient palliative care unit examined use of medications for sedation demonstrated no difference in survival Morita et al. Effects of high dose opioids and sedatives on survival in terminally ill cancer patients. J Pain Sympt Manage. 2001 Family as the Patient 5 Things Families Can Say to Loved Ones Near Death • • • • • Please forgive me. I forgive you. Thank you. I love you. Goodbye. Attributed to Byock. The Four things that Matter Most. New York, NY; Free Press; 2004. Referral for Bereavement Counseling • Hospices offer bereavement counseling to the larger community, not just the families of patients under their care Generalizations • PROGNOSIS: – Important for patient and family to achieve goals / closure – Time-frame: hours-days, days-weeks • PREPARATION: – Prepare family for likely signs/sx, causes, and treatment – Discuss plan with nursing staff / wider team (consultants) – Stop inappropriate orders, document expected death • SYMPTOMS: – Only treat what is / appears to be disturbing to patient (or family in some cases) – Avoid treating one symptom and causing a new one (turning) – Be explicit about the purpose of using each medication