Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
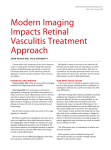
em 1996;22 (May) BriefReports Human brucellosis is commonly associated with musculoskeletal manifestations. Apart from sacroiliitis and spondylitis, peripheral arthritis presenting as monarthritis or asymetric peripheral oligoarthritis has been commonly described [1]. However, to our knowledge, the occurrence of a Baker's cyst as the first sign of brucellosis has not been described. We feel that brucellosis must be considered when a patient presents with a Baker's cyst and a constitutional syndrome, especially if the patient has risk factors for the development of this infectious disease. Ricardo Blanco, Miguel A. Gonzalez-Gay, Jose Varela, Rafael Monte, Amalia Sanchez-Andrade, and Carmen Gonzalez-Vela Divisions of Rheumatology and Infectious Diseases. Hospital XeralCalde, Lugo; and Division of Pathology. Hospital Marques de Valdecilla, Santander. Spain References I. Alarcon GS, Bocanegra TS, Gotuzzo E, Espinoza LR. The arthritis of brucellosis: a perspective one hundred years after Bruce's discovery. J Rheumatol 1987; 14:1083-5. Tuberculosis-Related Retinal Vasculitis in an Immunocompetent Patient In recent years, tuberculosis has reemerged as a serious public health problem [1], raising the possibility that rare manifestations of the disease, such as ocular tuberculosis, may also become more prevalent. We describe a previously healthy 31-year-old man with retinal vasculitis associated with systemic tuberculosis. Mycobacterium tuberculosis was isolated from a cervical lymph node biopsy specimen and sputum. A test for antibody to HIV was negative. Ophthalmologic examination revealed normal visual acuity in both eyes. Preretinal hemorrhage, exudates, and periphlebitis were observed on the retina of the right eye (figure 1). Behcet's syndrome, multiple sclerosis, systemic vasculitis, and syphilis were clinically and biologically ruled out as potential causes of retinal vasculitis. The patient was treated with a 6-month regimen of isoniazid, rifampin, ethambutol, and pyrazinamide for 2 months followed by isoniazid and rifampin for 4 months. Prednisone (30 mg/d) was administered for 2 weeks as treatment for retinal vasculitis. The patient immediately felt better, and his body temperature returned to normal within 6 days of initiation of treatment. Three weeks later, examination ofthe fundus showed marked abatement of the retinal vasculitis, but peripheral ischemic areas had appeared. Preventive laser photocoagulation of these areas was performed. Seven months after treatment was begun, fluorescein angiography showed complete recovery and no residual lesions. Reprints or correspondence: Dr. Gilles Raguin, Hopital de la Croix-SaintSimon, 125 rue d'Avron, 75960 Paris Cedex 20,France. Clinical Infectious Diseases 1996; 22:873-4 © 1996 by The University ofChicago. All rights reserved. 1058-4838/9612205-0048$02.00 873 2. Cuende E, Barbadillo C, E-Mazzuehelli R,Isasi C,Trujillo A,Andreu JL. Candida arthritis inadult patients who arenot intravenous drug addicts: report ofthree cases and review oftheliterature. Semin Arthritis Rheum 1993; 22:224-41. 3. Austin KS, Testa NN, Luntz RK, Greene JB, Smiles S.Aspergillus infection oftotal knee arthroplasty presenting asa popliteal cyst: case report and review of the literature. J Arthroplasty 1992; 7:311-4. 4. Ellis ME, el-Ramahi KM, al-Dalaan AN. Tuberculosis ofperipheral joints: a dilemma in diagnosis. Tuber Lung Dis 1993;74:399-404. 5. Resnick D, Berthiaume MJ. Sartoris D. Imaging. In: Kelley WN, Harris ED, Ruddy S, Sledge CB, eds. Textbook of rheumatology. Vol. I. Baltimore: WB Saunders, 1993:598, 892. 6. Samanta A, Boyd 0, Roy S. An unusual presentation of Baker's cyst in a patient with rheumatoid arthritis. Br J Rheumatol 1988;27: 500. 7. Anderson CJ, Cannon GW, Andrews JM. Gouty tophus presenting as "pseudo-Baker's cyst" [letter]. J Rheumatol1989; 16:1281-2. 8. Meehan PL, Daftari T. Pigmented villonodular synovitis presenting as a popliteal cyst in a child: a case report. J Bone Joint Surg Am 1994;76:593-5. 9. lsdale AH, Iveson JM. Synovial cysts and sarcoid synovitis. BrJ Rheumatol 1992; 31 :497 9. 10. Brancaccio D, Gallieni M, Padovese P, Anelli A, Coggi G, Uslenghi C. Dialysis amyloidosis with massive popliteal deposition of beta 2mieroglobulin amyloid. Lancet 1988;2:802. Retinal vasculitis may be primary or secondary to a variety of systemic disorders [2]. It has been reported in association with neurological diseases, systemic inflammatory diseases, malignancies, and infectious diseases such as syphilis, endocarditis, malaria, toxoplasmosis, and fungal and viral infections. Samples of retinal vasculitic lesions are usually not available for bacteriologic or histologic examination. Therefore, the diagnosis of tuberculosisrelated retinal vasculitis on the basis of the clinical picture is presumptive. In our case the systemic tuberculosis, the exclusion of other possible etiologies, and the favorable evolution of the Fluorescein angiogram of the right eye of a 31-yearold man with retinal vasculitis associated with systemic tuberculosis revealeda hemorrhage and exudate (A) and a periphlebitic lesion (B). Figure 1. 874 Brief Reports patient's condition with specific treatment made this diagnosis most probable. To our knowledge, all reported cases oftuberculosis-related retinal vasculitis involved symptomatic patients with loss of vision who were referred to ophthalmologists. Our case is remarkable for the identification of retinal vasculitis at a stage when no visual impairment had occurred. This identification allowed early specific ocular treatment. The pathogenesis of tuberculosis-related retinal vasculitis is still unresolved. Two major mechanisms could be implicated. One involves an infectious process; the hypothesis suggests that tuberculous bacilli are directly responsible for the observed lesions. This mechanism seems probable when tubercles are present on the choroid. However, when no specific ocular lesions are seen, it is uncertain whether vasculitie lesions contain active bacilli. The alternative hypothesis states that hypersensitivity mechanisms are responsible for the observed vasculitis [3, 4]. These two models are not mutually exclusive and, whatever the actual mechanism, the treatment remains the same. The appropriate treatment consists of administration of antituberculous agents, usually in association with systemic corticosteroid therapy and photocoagulation of the retina if required. Following treatment, the evolution of the condition is usually favorable. However, after initial substantial abatement of the vaculitis, secondary neovascularization and vitreous Bacteremia and Hemoptysis Due to an Infected False Left Ventricular Aneurysm Associated with a Bronchoventricular Fistula Hemoptysis in a bacteremic patient may present a diagnostic dilemma: this complication may represent a secondary inflammation of the airway, septic pulmonary emboli, or, rarely, a mycotic aneurysm of a bronchial artery. We present a case of massive hemoptysis due to a false aneurysm ofthe left ventricle that became secondarily infected with Staphylococcus aureus and fistulized into the bronchial tree 10 years after a cardiac injury. A 43-year-old male iv drug user presented with acute onset of fever and moderate hemoptysis without associated chest pain or shortness of breath. His medical history revealed a penetrating chest wound and cardiac injury that had been repaired 10 years earlier. In addition, 4 months before the onset of hemoptysis, he developed methicillin-resistant S. aureus (MRSA) bacteremia and osteomyelitis of the left hip that were treated with a 6-week course of vancomycin at another facility. Physical examination showed the patient to be alert, oriented, and in no distress. His temperature was 39.4°C; blood pressure, 136/80 mm Hg; pulse rate, 102; and respiratory rate, 20. The rest of the examination was unremarkable except for tenderness in the left groin and decreased range of motion in the hip. All four blood cultures that were performed over a 3-day period were positive Reprints or correspondence: Dr. Riad Khatib, Medical Education Office, St. John Hospital and Medical Center, 22101 Moross Road, Detroit, Michigan 48236. Clinical Infectious Diseases 1996;22:874-5 © 1996 by The University of Chicago. All rights reserved. 1058-4838/96/2205-0049$02.00 CID 1996;22 (May) hemorrhage have been described [4]. Therefore, until complete recovery, ophthalmologic follow-up is required. Even though it is a rare complication of systemic tuberculosis [5], retinal vasculitis should be searched for in this era of recurrence of tuberculosis. Indeed, retinal tuberculosis may have serious consequences for the patient if the diagnosis and appropriate treatment are delayed. A biomicroscopic eye evaluation is a rapid, sensitive, nonaggressive, low-cost procedure; it should therefore be a routine means of examination of tuberculous patients. Jean L. Reny, Georges ChaUe, Philippe Geisert, Jean Aerts, Jean M. Ziza, and Gilles Raguin Service de Medecine Interne et Maladies Infectieuses, Hopital de la Croix-Saint-Simon, Paris, France References I. Comstock GW. Variability of tuberculosis trends in a time of resurgence. Clin Infect Dis 1994; 19:1015-22. 2. Vine AK. Retinal vasculitis. Semin Neurol 1994; 14:354-60. 3. Helm CG, Holland GN. Ocular tuberculosis. Surv Ophthalmol 1993; 38:229·56. 4. Rosen PH, Spalton OJ, Graham EM. Intraocular tuberculosis. Eye 1990; 4:486-92. 5. Donahue He. Ophthalmologic experience in a tuberculous sanatorium. Am J Ophthalmol 1967;64:742-8. for MRSA. His chest roentgenogram showed a density adjacent to the left heart border. Initially, he was suspected of having pulmonary emboli secondary to septic thrombophlebitis ofthe left femoral vein in association with septic arthritis of the left hip. However, a pulmonary angiogram did not show any abnormalities. He defervesced while receiving vancomycin therapy, and his condition seemed to improve, but occasional scant hemoptysis persisted. Bronchoscopic evaluation of his airway showed bloody secretions in the left lower lobe, without any obvious intrabronchial defect. A transthoracic echocardiogram demonstrated a cystic lesion (4.5 X 6 em) posterolateral to the left ventricle. A CT scan of the chest showed that this lesion represented two contiguous masses (10 X 5 em) that were associated with the ventricle (figure 1). Ventriculography illustrated mild left ventricular enlargement with evidence of anteroapical akinesis and flow into the adjacent mass, consistent with a false aneurysm. On the tenth hospital day, the patient underwent surgery after he developed massive hemoptysis (about I pint of blood), shortness of breath, and hypotension (systolic blood pressure, 80-100 mm Hg; diastolic blood pressure, 45-55 mm Hg). Evidence of an old, healed anterior wound was noted in the left ventricle. The inferior wall had a defect (1.5 X 1.5 ern) leading to a large aneurysmal sac with a chronic thrombus in the exposed left ventricle. Culture of the thrombus yielded MRSA. The patient was treated with a 56-day course of vancomycin and gentamicin (peak levels of gentamicin, 3 j.lg/mL). His left hip was resected because of persistent disabling pain (culture of the resected bone yielded MRSA), and eventually he was discharged. He was well at a 6-month follow-up examination. False aneurysm is a known complication of traumatic cardiac injuries [1- 3]. It may be associated with a variety of symptoms or may cause sudden death. It may also be asymptomatic and be detected during a routine follow-up examination. Our patient