Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
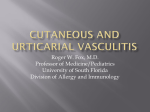
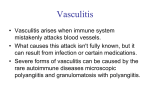
RHEUMATOID VASCULITIS Kamal Kolappa UNC Internal Medicine Morning Report 7.7.10 BACKGROUND Rheumatoid Vasculitis (RV) is a rare complication of longstanding, severe Rheumatoid Arthritis (RA) Estimated incidence in 2-5% of RA patients1 Associated with chronic RA: Mean lag time 13.6 years between diagnosis of RA and onset of RV Males are 2-4x more likely to develop RV than females RV cutaneous ulcer Characterized by Extra-Articular involvement of disease Specifically the small and medium vessel arteries similar to polyarteritis nodosa Correlated to high RF levels and low complement at onset of RV development; indicating uncontrolled RA disease as a risk factor2 Anecdotal evidence that viral infections and drug reactions can precipitate RV occurrence in RA patients3 DISEASE MANIFESTATIONS Cutaneous Manifestations secondary to vascular compromise (90% of RV patients evidence this)4 Digital ischemia to fingers and toes Cutaneous ulcers resulting from obstruction of superficial and medium vessels Nail fold infarcts Nerve Infarction (involves vasa vasorum) causing mononeuritis multiplex foot and wrist drop Associated w/ neuropathy characterized by numbness, burning, pain that precedes muscle weakness, paralysis, and wasting Ocular Scleritis Non specific signs: Fever, Weight Loss Source: Up to Date INVOLVEMENT OF LARGE ARTERIES Classically, disease often limited to small and medium arteries; case reports of large artery involvement exist Bowel6 Renal Brain (CVA’s) Coronary Vasculitis (rare)5 Focus back to Ms. R: Extensive CVA w/o other leading cause (MCA distribution) Hematuric evidence of possible Renal involvement GG pulmonary opacities can be seen w/ pulmonary vasculitis Large cecal perforation w/ bx proven vasculitic involvement CTA-Head +CTA Chest Of Ms. R DIAGNOSIS OF RV Fibrinoid Necrosis in vessel wall Source: Up to Date Evidence gathered from: H&P: Suspect RV in any RA patient w/ fevers, weight loss, skin ulcerations, necrotic digits, or sx of sensory or motor nerve dysfxn Labwork: specifically elevated RF7, low complement, elevated ESR, elevated Anti-CCP (citrullinated peptides) high odds ratio for possible RV in a person w/ h/o RA Keep in Mind: No definitive Lab dx of RV Imaging: Angiogram rarely useful as majority of vessels involved are medium (below image resolution); findings(segmental narrowing) are nonspecific to RV Full Thickness Skin Biopsy: As above, would show evidence of fibrinoid necrosis of vessels DIFFERENTIAL DIAGNOSTIC CONSIDERATIONS Cryoglobulinemia (Rx w/ Plex as opposed to immunosuppression Rx of RV)7 Presents w/ palpable purpura, cutaneous ulcers, myalgias Usually RF positive Small vessel vasculitis of skin(purpura, pustules) usually not seen in RV as in Cryoglobulinemia Polyartertis Nodosa (nearly indistinguishable from RV); key is clinical features, i.e. pt w/ strong hx of RA more likely has RV rather than PN ANCA Vasculitides: Also RF positive Wegener’s, Churg Strauss, Microscopic Polyangiitis Vasculitis-like Syndromes Thrombo-embolic phenomenon (cholesterol emboli) Infectious Endocarditis (fever, skin lesions, active urine sediment) TREATMENT OF RHEUMATOID VASCULITIS Differs based on extent of involvement: Cutaneous vs. Systemic8 Cutaneous Involvement Isolated Nailfold Infarctions: secondary to low grade small vessel vasculitis symptomatic Rx, low risk of progression to systemic vasculitis Leg ulcerations: Rx ~venous stasis, i.e. wet to moist saline dressings, compression bandages, hydrogel occlusive dressings; Higher assocation w/ systemic RV Systemic RV High Dose Glucocorticoids (1-3 days of Solumedrol 1gram/day) transition to PO Prednisone Cytotoxic agent (e.g. Cyclophosphamide); Achieves disease remission; Alt: MTX, Azathoprione, TNF inhibitors REFERENCES 1. Voskuyl AE et al. Factors associated with the development of vasculitis in rheumatoid arthritis: results of a case-control study. Ann Rheum Dis. 1996; 55:190 2. Scott DG et al. Systemic Rheumatoid Arthritis: a clinical and laboratory study of 50 cases. Medicine(Baltimore) 1981; 60:288-290 3. Iyngkaran P et al. Rheumatoid vasculitis following influenza vaccination. Rheum. 2003; 42: 907-909 4. Sayah A et al. Rheumatoid Arthritis: A review of cutaneous manifestations. J Am Acad Dermatol. 2005; 53: 191-193 5. vanl Albada-Kuipers et al. Coronary arteritis complicating rheumatoid arthritis. Ann Rheum Dis. 1986; 45:963-968 6. Pagnoux C et al. Presentation and outcome of gastrointestinal involvement in systemic necrotizing vasculitides: analysis of 62 patients with polyarteritis nodosa, microscopic polyangiitis, wegener granulomatosis, churg-strauss syndrome, or rheumatoid-associated vasculitis. Medicine (Baltimore) 2005; 84:115-116 7. Geirsson AJ et al. Clinical and serological features of severe vasculitis in rheumatoid arthritis: A clinicopathologic and prognostic study of thirty-two patients. Arhtritis Rheum. 1995; 55:190-193 8. Abel T et al. Rheumatoid Vasculitis: effect of cyclophosphamide on the clinical course and levels of circulating immune complexes. Ann Internal Medicine. 1980; 93:407-408 APPRECIATE YOUR ATTENTION! Special Thanks to my Med U team: Eric Edwards, Andy Mcwilliams, Chris Sayed, Ross, Tim and Damon, Crystal, Eric Allman, and Paul Dombrower aka Master P