Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
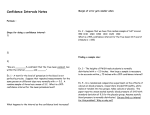
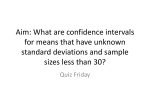
559 The Contractile State of Cat and Dog Heart in Relation to the Interval between Beats J. PIDGEON, M. LAB, A. SEED, G. ELZINGA, D. PAPADOYANNIS, AND M.I.M. NOBLE Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017 SUMMARY We induced atrioventricular dissociation and initiated ventricular pacing in intact dogs and isolated cat hearts. Left ventricular pressure, its time derivative (dP/dt), and action potentials were recorded. When a test pulse was introduced at varying intervals after a period of steady pacing, an optimum contractile response was obtained at an average interval of 720 msec. A similar optimum interval was obtained after pacing at various frequencies and after paired pulse stimulation but was shortened to 560 msec after infusion of epinephrine. The magnitude of the optimum contractile response increased with an increase in the frequency of prior pacing which was accompanied by an increase in the time the cell membrane was depolarized. The optimum contractile response following paired pulse stimulation was greater than that following regular pacing, with the same number of stimuli per minute and the same time of membrane depolarization. The results are explicable in terms of intracellular calcium ion recirculation with separate compartments for release to and uptake from the contractile proteins. A negative feedback control of Ca2+ inflow to the cell by intracellular Ca2+ content is postulated to explain the effect of paired pulse stimulation and shortening of action potential duration following an increase in regular pacing frequency. Circ Res 47: 559-567, 1980 CONSIDERABLE insight has been gained in recent years into the relationship between the strength of a cardiac muscle contraction and the interval between beats. Studies of this topic have been carried out on isolated strips of cardiac muscle in which isometric tension can be measured and action potentials recorded by intracellular microelectrodes (Koch-Weser and Blinks, 1963; Allen et al., 1976; Edman and Johannsson, 1976). Anderson et al. (1976) already have shown that patterns of mechanical response observed in isolated muscle hold for the intact ventricle. These studies show a marked influence of the preceding interval on the strength of a beat. In particular, there is a partial refractoriness of the mechanical response after a previous contraction which takes a period of time to recover. Edman and Johannsson (1976) first defined the time interval after a priming period of steady state stimulation at which a further stimulus would evoke an optimum contraction, and then examined how the frequency during the priming period influenced the force of this optimum response. This optimum contractile response proved to be a useful index of the potential contractile force, which was assumed to be related to the amount of activator calcium available. We wished to establish whether this held in the From the Departments of Medicine and Physiology, Charing Cross Hospital, London, England; Department of Physiology, Free University, Amsterdam, The Netherlands; and Midhurst Medical Research Institute, Midhurst, Sussex, England. This work was supported by grants from the Medical Research Council, the Wellcome Trust, the Mason Medical Research Foundation, and N.A.T.O. Address for reprints: Dr. W.A. Seed, Department of Medicine, Charing Cross Hospital, London W6 8RF, England. Original manuscript received June 5, 1979; accepted for publication April 24, 1980. intact heart. We therefore initially followed Edman and Johannsson's experimental design and then attempted to characterize the activation system in some further detail. The experiments we describe were performed in anesthetized open- or closedchest dogs with intact circulations and in isolated, blood-perfused, and ejecting cat hearts. Methods Preparations Closed-Chest Anesthetized Dogs Six mongrel dogs were anesthetized with intravenous thiopental followed by 1% halothane in nitrous oxide and oxygen. A right thoracotomy was performed under aseptic conditions. The pericardium was opened and epicardial pacing wires were sewn to the right ventricle. To allow studies at cardiac frequencies below the spontaneous heart rate, we induced complete heart block by injecting small quantities of formaldehyde into the interventricular septum in the vicinity of the bundle of His while the electrocardiogram was monitored (Steiner and Kovalik, 1968). When complete atrioventricular dissociation had been established, an implantable demand pacemaker (Devices 3821) was connected to the pacing wires and buried under the skin at the back of the neck. In two dogs, two piezoelectric crystals were implanted into the left ventricle in order to measure a cavity diameter with ultrasound. The chest was closed and drained. One week after recovery, and in one case on later occasions also, the dogs were anesthetized with intravenous 1% thiopental followed by chloralose (40 mg/kg), and the pacing wires at the back of the neck were exposed. A Gaeltec (Gaeltec Ltd.) cath- 560 CIRCULATION RESEARCH eter tip micromanometer was introduced into the left ventricle via a femoral artery. Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017 Open-Chest Anesthetized Dogs Ten mongrel dogs were anesthetized with intravenous thiopental followed by 1% halothane in nitrous oxide and oxygen. This anesthetic plus intermittent positive-pressure ventilation with a Blease Manley ventilator was maintained until the end of the experiment; arterial Po2, Pco2, and pH were monitored and kept normal. Each animal was positioned on its back, and a window consisting of the sternum and some of the adjacent ribs was removed to expose the anterior aspect of the heart. The pericardium was incised and the edges were sutured to the chest wall to form a pericardial cradle. Pacing wires were sewn to the right ventricle, and heart block was induced as described previously. A Gaeltec catheter-tip manometer was introduced as before. An electrode was applied to the surface of the ventricles for action potential recording. Isolated Ejecting Cat Heart The preparation was set up as described by Elzinga and Westerhof (1978). Cat hearts were isolated in such a way that normal function of the left heart was maintained. This was achieved by cannulating the aorta and left atrium while the pulmonary veins were tied off. The left atrial cannula was connected to an overflow vessel providing a constant filling pressure, and the cannula in the aorta coupled the heart to a hydraulic model of the input impedance of the cat's systemic arterial system. In the cannula connected to the aorta, an occluder was mounted as described by Elzinga et al. (1977) so that isovolumic beats could be interpolated. Electrodes were sewn on the right ventricle for pacing, and heart block then was induced in the same way as for the dog preparations. Measurements Pressure Left ventricular (LV) pressure was measured in the dogs with a Gaeltec catheter-tip pressure transducer used in conjunction with Hewlett-Packard (8805B) or Devices (3552) carrier amplifiers. The resonant frequency of the manometers was about 12 kHz. They showed no detectable gain change between room and blood temperature (<0.5%) but in some cases showed small baseline drifts. Therefore hydraulic calibrations at room temperature were used to derive gain, and zero was taken as the signal recorded at the moment of removal of the catheter tip from the femoral artery. The pressure signals were differentiated electronically to derive the rate of change of pressure (dP/ dt). The response of the differentiators was linear for amplitude and phase to 100 Hz with a transit VOL. 47, No. 4, OCTOBER 1980 time of 1 msec. The ventricular pressure signals also were amplified to allow determination of enddiastolic values. Aortic pressure was measured through a fluid-filled catheter in the carotid artery. In the cat hearts, LV and aortic pressures were measured through short fluid-filled cannulas; the resonant frequencies were 80 Hz for aortic and 150 Hz for LV catheter manometer systems. LV Diameter The distance between the two implanted crystals was calculated from the transit time between them of ultrasound pulses generated via an Ekoline 20 (Smith Kline Instruments) echocardiograph. During the experiments, an analog signal of the diameter through the cardiac cycle was obtained from the time analog module of the Ekoline. The linearity of this system was confirmed in vitro, and the frequency response was shown to be flat to 30 Hz. Epicardial Action Potentials Measurements were made as described by Lab and Woollard (1978). The open end of a polyethylene tube 2 mm in diameter was held in position on the surface of one or other ventricle by the application of negative pressure to the other end of the tube. Two silver-silver chloride electrodes were used, one in contact with the heart within the lumen of the tube and one on the outside of the tube which made contact with the heart surface by means of a saline-soaked cotton pledget. The potential difference between the two electrodes was measured with a Devices 3461 preamplifier. The action potential duration (taken as the time during which the myocardial cells were depolarized by more than 70%) was measured directly from the records. Recording Signals were recorded on Brush 480, Devices M 19 or Elema Schonander EMT 81 pen recorders, or a Micromovements M10-120A light-beam recorder. In those experiments in which action potential measurements were made, the primary signals also were recorded on a Racal Store 4 or a Hewlett-Packard 352A instrumentation tape recorder. Stimulation Timing of stimuli used to drive the ventricles was achieved with, a Digitimer (Devices, 3290) which provided two adjustable cycle times, each of which contained one or more trigger pulses. This system provided pulses for steady single or paired pacing and abrupt changes of rate by switching between cycle times. The trigger pulses from the Digitimer were used to drive a Devices 2538 stimulator, the voltage of which was adjusted to be 10-15% above threshold. INTERVAL-STRENGTH RELATION OF INTACT HEART'/Pidgeon et al. PROTOCOL 1 PROTOCOL 2 TEST PULSE INTERVAL PRIMING PERIOD OPTIMUM TEST PULSE INTERVAL PROTOCOL 3 TEST PULSE INTERVAL PROTOCOL 4 OPTIMUM TEST PULSE INTERVAL Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017 FIGURE 1 Patterns of pacing used in this study. Stimulation Protocols Determination of Optimum Interval (Fig. 1, Protocol 1) During the period prior to the introduction of a test pulse (the "priming period"), the heart was paced at a fixed frequency until ventricular pressure, dP/dtmax, and action potential duration had reached a steady state. Then a test pulse was introduced by switching briefly to a different cycle time on the Digitimer pulse generator. This new interval (test pulse interval) then was switched out, usually after one beat, and reset to a new duration. After a further priming period had ensured recovery of the original steady state, it again was switched in. This procedure was repeated until a range of test pulse intervals had been explored. LV dP/dt^x of the test beat, either as an absolute value or as a ratio of the preceding steady state value, then was plotted against the test pulse interval to derive by eye the optimum test pulse interval. In six experiments, the test pulse interval curve at a given priming frequency was determined before and during an infusion of epinephrine. At very long intervals, the aortic diastolic pressure falls to low levels at which the maximum rate of rise of LV pressure is no longer an isovolumic event (Van den Bos et al., 1973). The possible occurrence of this situation was monitored from the 561 aortic and LV pressure records; in none of the experiments was it seen. In the cat hearts, the beat after the test pulse interval was an isovolumic one against a closed shutter. Influence of Priming Frequency (Fig. 1, Protocol 2) The procedure described above was repeated with a number of different priming frequencies ranging from 1 to 4 Hz. The effect of the steady state heart rate on the entire test pulse interval curve thus was determined. The optimum values from each curve then were plotted against the priming (steady state) frequency (Edman and Johannsson, 1976). To obtain more points on this plot, additional tests were performed using many values of priming frequency and a test pulse interval fixed at the optimum value determined during the previous runs. Experimental records from such a test are shown in Fig. 2. Paired Pulse Stimulation (Fig. 1, Protocols 3 and 4) With the Digitimer set to generate paired pulses, test pulse interval curves were determined (protocol 3) from which the optimum test pulse interval was estimated. In addition, in six experiments, protocol 4 was followed. Stimuli at the optimum test pulse interval (previously determined) were applied after periods of single pacing at a given frequency and of paired pulse pacing at half that frequency. The process was repeated at several priming frequencies, and plots of optimum contractile response against priming frequency were constructed for both single and paired pacing. Volume Infusion To determine the effect of changes in heart size upon dP/dtmax, saline at 37 °C was rapidly infused intravenously in all the experiments reported. LV end-diastolic pressure or diameter was used to monitor the changes in heart size, and dP/dtmax was measured at a number of different steady state priming frequencies. In addition, in five dogs, test pulse interval curves (Fig. 1, protocol 1), performed at the same priming frequency before and after the saline infusion, were examined. In isolated cat hearts, we raised the left atrial reservoir instead of infusing saline. Observations were made at a variety of steady state priming intervals over the range of heart size explored. Results Effect of Ventricular Volume on Contractile Indices A change of heart size had no effect on LV dP/ max in the majority of experiments (Table 1). In 562 CIRCULATION RESEARCH VOL. 47, No. 4, OCTOBER 1980 38 —, L. V. DIAMETER mm 30 _ 5000 _, L V . dP dt mm Hg sec. 0 —' 150 —, Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017 r\ r\ L. V. PRESSURE mm.Hg. V-J I 1 Second I 2 Experimental records demonstrating the frequency dependence of optimum contractile response. Top record shows LV diameter measured with ultrasound crystals. Bottom record shows LV pressure and middle record shows its rate of change (dP/dt). The priming frequency increases in steps (Fig. 1, protocol 2). The last beat on each record is the test pulse. Note constant (optimum) test pulse interval and progressive increase in amplitude of the test pulse dP/dtmax. FIGURE those experiments in which dP/dtmax was affected, we eliminated volume-dependent changes in dP/ dtmax by excluding from analysis all those observations in which LV dimensions or end-diastolic pressure at the onset of the test contraction exceeded those during the priming period. In the five dogs in which test pulse interval curves were examined 1 The Effect of Elevation ofLV End-Diastolic Pressure on Steady State TABLE Experiment no. 1 3 4 5 7 8 (i) 8 (ii) 9 10 12 13 14 15 16 19 20 21 Increase in LV end-diastolic pressure (mm Hg) 9.0 0.8* 10.0 6.0 6.4 9.7 n.q 2.8 10.7 5.7 18.0 2.1 5.4 6.6 14.8 7.4 5.5 •increase in end-diastoiic diameter (cm). t Significant rise (p < o.oi). % Change of LV dP/dt™. 115.8 115.4 145.4 0.0 1 6.4 T22.0| 1 4.5 114.9 1 3.1 T 15.8| 117.6 0.0 1 9.4 T12.0f 143.4 1 9.8 t 3.9 before and after volume expansion, no changes in shape or optimum test pulse interval were observed. Optimum Test Pulse Interval As the test pulse interval was increased (Fig. 1, protocol 1), the strength of the contraction increased and reached a maximum. The interval at which this maximum occurred was: 665 msec (range 500-800) for six closed - chest dogs; 750 msec (range 500-1000) for 10 open-chest dogs; and 795 msec (range 700-1000) for six isolated, ejecting cat hearts. Under control conditions, there was little further change or a gradual decay in contractile strength at intervals longer than these. Results from an individual experiment on a dog are shown in Figure 3a and from an experiment on a cat in Figure 3b. There was a tendency for the optimum test pulse interval to shorten with increasing priming frequency. In six dogs studied over the widest range of priming frequencies (1-4 Hz), optimum test pulse interval shortened significantly ( P = 0.02) when values at 1 and 4 Hz were compared but not when intermediate values were compared. Figure 3 also shows that the entire test pulse interval curve shifted upward when the priming frequency was increased (priming interval decreased). There is one point on each curve at which the test pulse interval is the same as the priming interval. In Figures 3a and 3b, these points have been joined by a solid line to indicate that the INTERVAL-STRENGTH RELATION OF INTACT HEART/Pidgeonetal. 563 LV dP/dt max 2200 ImmHg/secl 2000 LV aP/dt nax 4000 fnnHg/seci 1800 1600 3000 140L> - 1200 1000 2000 STEADY STATE INTERVAL (msl 800 600 1000 Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017 STEADY STATE INTERVAL ims) 400 200 B 0 200 400 600 800 1000 TEST PULSE INTERVAL 1200 1400 1600 200 400 imsi 600 800 1000 1200 1400 1600 TEST PULSE INTERVAL (ms) LV dP/dt max 4000 (mmHg/seci 3000 RATIO TP/SS 1.4 1.4 LV dP/dt max 1.2 - 1.0 - 2000 c / / INTERVAL 333ms 0.8 AControl x Epinephrine infusion /• 0.6 - Before heart block • After heart block • / 1000 0.4 STEADY STATE INTERVAL 333 ms /• 0.2 / D 0 400 800 TEST PULSE INTERVAL 1200 1600 imsi 0 100 200 TEST P U L S E 300 400 500 INTERVAL (msl 3 A: Test pulse interval curves for a dog heart, constructed at three different steady state frequencies. The curves in this and subsequent figures were drawn by hand through the data points. The optimum test pulse interval is about 550 msec and shows little change with increasing steady state frequency. The solid line shows how the steady state response changes with changing priming frequency. B: Test pulse interval curves at three frequencies for an isolated cat heart. C: Test pulse interval curves before and during epinephrine infusion at 1 fig/kg per min in a dog. D: Test pulse interval curves for the same animal before and after heart block. Test pulse amplitude in each case normalized by preceding steady state amplitude. The curve is incomplete because the spontaneous beat-to-beat interval before block was 500 msec. FIGURE contractile strength of the priming beats (steady state strength-interval response) changes little with increasing frequency. The effect of epinephrine on the test pulse inter- val curve was studied in nine dogs. After control studies, epinephrine was infused at a rate (1-2 jug/ kg per min) sufficient to produce an increase of more than 50% in LV dP/dtma,, and that rate was 564 CIRCULATION RESEARCH maintained while the test pulse interval curve was remeasured. In all nine experiments, epinephrine caused a shortening of the optimum test pulse interval and a steeper decline of contractile strength at intervals longer than the optimum. The mean test pulse intervals were: control, 740 ± 100 (mean ± SD) msec; and epinephrine, 560 ±110 msec (P < 0.01, Student's paired t-test). VOL. 47, No. 4, OCTOBER 1980 Normalized 160 LV dP/dt max n-6 (Results + SEMI i • Test pulse contraction IOCR) / O Steady state contraction / 140 / 120 Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017 Effect of Ventricular Pacing (Asynchronous Contraction) on Contractile Indices Activation of the ventricles by ventricular pacing differs from normal activation, and this might influence the strength-interval behavior of the heart. To examine this possibility, we constructed test pulse interval curves in five dogs before and after the induction of heart block. Before heart block, the heart was paced via right atrial epicardial electrodes, using a priming frequency just above the spontaneous heart rate and test pulse intervals up to this frequency. After heart block, the process was repeated with right ventricular pacing. Because of the high spontaneous heart rate, the preblock experiment yielded only truncated test pulse interval curves. In one animal, the results before and after block were indistinguishable. In the remainder, absolute values of dP/dtmax were reduced after block, but when the results were normalized against dP/ dtmax during the priming periods to allow for this, the test pulse interval curves were indistinguishable (Fig. 3d). Thus, although heart block reduced absolute values of dP/dt,nax in most instances, it did not change its relation to test pulse interval. Effect of Changing Priming Interval (Fig. 1, Protocol 2) As described above, the strength of the priming beats changed little with increasing priming frequency. However, the contractile strength of the test contraction at the optimum interval increased progressively over the range of priming frequencies, as can be seen in Figures 2 and 3a and 3b. In Figure 4, optimum contractile response and steady state response are plotted against steady state frequency, for the isolated cat heart (Fig. 4a) and the intact dog heart (Fig. 4b). In both species, there was a progressive rise in optimum contractile response, in contrast to the steady state response. An increase of priming frequency caused a decline in action potential duration to a new steady state value (Fig. 5a). However, with each increase in priming frequency, because of the greater number of action potentials per unit time, the heart spent a progressively greater proportion of time depolarized. Under these circumstances, there was a correlation between optimum contractile response and the percentage of time the membrane was depolarized (Fig. 5b). 100 • A 1.0 Normalized LVdp/dt max 3.0 2.0 FREQUENCY IHzl IW DOC 150 n •6 (Results ; SEM) 140 . o Test pulse contraction (OCR I A Steady state contraction 130 120 110 100 B "1 2 3 Frequency 4 IHzl FIGURE 4 Behavior of steady state and optimum contractile responses with frequency of steady state stimulation. Optimum contractile response (OCR; ordinate) expressed as a ratio ofdP/dtma% for that beat divided by dP/dtmai for steady state response at lowest frequency tested. Data pooled from six isolated cat hearts (A) and six dog experiments (B). Paired Pulse Stimulation Paired pulse stimulation during the priming period (Fig. 1, protocol 3) was performed at coupling intervals between 210 and 300 msec; the interval was kept constant within a given experiment. This produced augmented responses to both priming and test pulses compared to single pacing. The optimum test pulse interval following paired pulse stimula- INTERVAL-STRENGTH RELATION OF INTACT HEART/Pidgeon et al. 565 LV dP/dt max (mmHg/sec) 40 mV 40 mV STEADY • STATE o Normal Pacing (Interval 500ms) Paired Pacing (Interval looomsl 0.5s Normalised LVtfc/cfl max (OCR) I Results with SEM n-6 140 0 400 800 1200 TEST PULSE INTERVAL 1600 (ms) OCR tnmHq/secl 3d Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017 2200 r 120 110 T 100 * . 0 1 B ,, 25 30 35 45 Fraction of time membrane > 70% depolarised 45 1200 (%l 5 A: Epicardial action potentials recorded at the same paper speed in the dog during steady state stimulation at 1.25 and 2.1 Hz. The broken line indicates 70% depolarization, the level at which action potential duration was measured. Note shortening with increased heart rate. B: Relationship between percentage of time spent depolarized by membrane and optimum contractile response. Optimum contractile response normalized as in Figure 4. Results pooled from six dogs. 1000 FIGURE tion was similar to or shorter than that observed with single pacing (Fig. 6a). In order to explore further the relationship between optimum contractile response and the percentage of time during the priming period which the muscle spent depolarized, we examined optimum contractile responses for both single and paired pulse pacing using protocol 4 (Fig. 1). The results of such an experiment, performed at several priming frequencies, are shown in Figure 6b. The behavior with single pacing is the same as that described earlier (Fig. 4). With paired pacing, however, the optimum contractile response is consistently higher for any given percentage of time the membrane spends depolarized and shows little augmentation as depolarization time increases. Discussion This study shows that the ability of the heart to contract reaches an optimum 500-1000 msec after the previous beat and that this optimum contractile B 40 Fraction of time me Drane FIGURE 6 A: Test pulse interval curves for the same dog heart paced singly (protocol 1) and paired (protocol 3). B: Optimum contractile responses of a dog heart for single and paired pacing as illustrated in Figure 1, protocol 4. response increases with increasing frequency of the preceding beats. Recent analyses (see for example, Kaufmann et al., 1974; Allen et al., 1976; Edman and Johannsson, 1976) have interpreted the strength-interval relationship in terms of calcium ion movements. The concept has evolved that contractile force is determined by the amount of ionic calcium released in the immediate vicinity of the contractile proteins from stores within the cell. These stores trap Ca2+ which moves into the cell during the action potential, and release it for activation during subsequent action potentials. Thus, the Ca2+ content of the stores, which determines the inotropic state of the muscle at any instant, is labile and depends on the preceding history of activity. Studies on isolated cardiac muscle suggest that the Ca2+ released to activate the contractile proteins is re-stored during relaxation and requires a finite time to come into a state where it can be released again. If one beat follows another after an interval which is shorter 566 CIRCULATION RESEARCH Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017 than this recycling time, only a fraction of the Ca2+ taken up during relaxation is released. This results in a negative inotropic effect and masks the effect of the change in interval on the total amount of Ca2+ in the storage system, which can be considered to determine the potential contractile performance achieved if the total Ca2+ is released. Edman and Johannsson (1976) examined this potential by inserting stimuli after test intervals equal in time to the recycling time and found that the resulting contractions (termed "optimum contractile response") increased progressively over the entire range of steady state frequencies studied. This is the positive inotropic effect of increased frequency. In the present study of the intact heart, we followed the experimental protocols of Edman and Johannsson. To control the interval between beats over a wide range, heart block was induced and the right ventricle was paced. The sequence and synchrony of activation were therefore abnormal, and in most cases the magnitude of dP/dt max fell after block. However, this should not affect the analysis of the underlying mechanisms in the blocked heart, especially as the early part of the test pulse interval curve up to 500 msec had an identical form before and after block (Fig. 3d). A major potential problem is the fact that indices of contractile strength may be dependent on end-diastolic volume, and enddiastolic volume varies with the interval between beats. LV dP/dtmax sometimes can be independent of end-diastolic volume (Van den Bos et al., 1973), and this proved to be the case more often than not in this study (Table 1). Therefore, we consider that the plot of dP/dtmax against test pulse interval (Fig. 3) is relatively free from distortion from this cause. We conclude that the optimum interval obtained, 500-1000 msec (Figs. 3 and 6), is a valid indication of the true optimum of the intrinsic mechanism in the muscle which controls the contractile response. According to Edman and Johannsson, this is the time for Ca2+ (both entering during the previous action potential and sequestered from relaxation) to come into the releasable state. Effects similar to those shown in the present study can be observed in the records of KiLz et al. (1969), Anderson et al. (1976), and Arentzen et al. (1978). The problem of variable end-diastolic volume has less effect on the relationship between the priming frequency and the optimum contractile response (Fig. 4) because the test pulse interval (and therefore filling time) is fixed. Thus, the optimum contractile response increases progressively with heart rate over the entire range studied. This confirms Edman and Johannsson's findings for rabbit papillary muscle. Edman and Johannsson attributed the increase in optimum contractile response with increased stimulation rate (Fig. 4) to increased Ca2+ entry into the cell accompanying the increased number of action potentials per unit time. They found a close correlation between the fraction of time the cell VOL. 47, No. 4, OCTOBER 1980 membrane is depolarized and the optimum contractile response, a result which we have confirmed in the intact dog heart (Fig. 5b). In both their study and this one, an increase in heart rate produced its effect on optimum contractile response within a few beats. Therefore, a new balance between Ca2+ entry and efflux from the cell must be established rapidly in such circumstances since, in the steady state, Ca2+ inflow during the action potential of each beat must be balanced by an equal loss of Ca2+ from the cell. Evidence for such a beat-dependent effect is available from several studies (Hoffman et al., 1956; Koch-Weser and Blinks, 1963; Braveny and Sumbera, 1970; Wohlfart, 1979). When the heart rate is increased, there is an increase in Ca2+ influx due to the greater time the membrane is depolarized. Initially, this exceeds Ca2+ efflux so that Ca2+ accumulates but, subsequently, influx and efflux equalize to produce a new steady state with a higher intracellular Ca2+ as indicated by the greater optimum contractile response. This equalization could be due to increased efflux, resulting from the greater amount of Ca2+ within the cell. Alternatively, or in addition, the higher intracellular Ca2+ could reduce influx by shortening the action potential (Fig. 5a). Thus, we would not expect an obligatory relationship between the amount of Ca2+ in the intracellular pool and the steady state influx rate. Indeed, with paired pacing (Fig. 6b), for any given proportion of time that the membrane spent depolarized (time available for Ca2+ influx), the optimum contractile response is much greater than for single pacing. Our finding that catecholamines shorten the optimum interval (Fig. 3c) may be due to their property of producing faster relaxation, i.e., faster uptake of Ca2+ from the contractile proteins. If this calcium is passed to the releasable store, it might be expected to be available for release in a shorter time, thus shortening the optimum interval as observed. The best known analysis of the strength-interval relation is that of Koch-Weser and Blinks (1963) who assumed that the effect of a change in interval between beats depended on a summation between a positive inotropic effect, a negative inotropic effect, and the basal "rested state" level of contractility of the unstimulated or infrequently stimulated muscle. We now would interpret the positive inotropic effect of increased frequency, demonstrated by the increase in optimum contractile response, as following from a transient increase in calcium influx over efflux, leading to an increased s- •:? of the calcium pool. However, if successive l«eats at the higher frequency occur at less than the optimum interval, their contractility is reduced because of inadequate time between beats for Ca2+ to come into a releasable state; this reduction of contractility is the negative inotropic effect. Thus, the steady state contractile response results from a balance between INTERVAL-STRENGTH RELATION OF INTACT HEART/Pidgeon et al. the pool size of calcium and the time available for its recycling. The behavior of beats immediately following a step change in frequency can be interpreted in the same way. Thus, the beat obtained immediately after a change to higher frequency is weak because the interval is shorter than the optimum. With a sudden reduction of frequency, the first interval is lengthened, allowing greater filling of the releasable store, so the first beat is strong, reflecting the greater amount of Ca2+ in the system during the preceding period of high-frequency stimulation. These effects have been shown to occur in the intact heart (Kilz et al., 1969; Noble et al., 1969) as well as in isolated preparations. References Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017 Allen DG, Jewell BR, Wood EH (1976) Studies of the contractility of mammalian myocardium at low rates of stimulation. J Physiol (Lond) 254: 1-17 Anderson PAW, Rankin JS, Arentzen, CE, Anderson RW, Johnson EA (1976) Evaluation of the force-frequency relationship as a descriptor of the inotropic state of canine left ventricular myocardium. Circ Res 39: 832-839 Arentzen CE, Rankin JS, Anderson PAW, Feezor MD, Anderson RW (1978) Force-frequency characteristics of the left ventricle in the conscious dog. Circ Res 42: 64-71 Braveny P, Sumbera J (1970) Electromechanical correlations in the mammalian heart muscle. Pfluegers Arch 319: 36-48 Edman KAP, Johannssoh M (1976) The contractile state of rabbit papillary muscle in relation to stimulation frequency. J Physiol (Lond) 254: 565-581 567 Elzinga G, Westerhof N (1978) The effect of an increase in inotropic state and end-diastolic volume on the pumping ability of the feline left heart. Circ Res 42: 620-628 Elzinga G, Noble MIM, Stubbs J (1977) The effect of an increase in aortic pressure upon the inotropic state of cat and dog left ventricles. J Physiol (Lond) 273: 597-615 Hoffman BR, Bindler E, Suckling EE (1956) Post-extrasystolic potentiation of contraction in cardiac muscle. Am J Physiol 175:95-102 Kaufmann R, Bayer R, Furniss T, Krause H, Tritthart H (1974) Calcium movement controlling cardiac contractility. II. Analogue computation of cardiac excitation-contraction coupling on the basis of calcium kinetics in a multicompartment model. J Mol Cell Cardiol 6: 543-559 Kilz U, Niedermayer W, Nordmann KJ, Schaefer J, Schwarzkopf HJ, van Zwieten PA (1969) A comparison between frequency potentiation and post-extrasystolic potentiation in vitro and in situ. Pfluegers Arch 311: 226-242 Koch-Weser J, Blinks JR (1963) The influence of the interval between beats on myocardial contractility. Pharmacol Rev 15: 601-652 Lab MJ, Woollard KV (1978) Monophasic action potential electrocardiograms and mechanical performance in normal and ischaemic epicardial segments of the pig ventricle in situ. Cardiovasc Res 12: 555-565 Noble MIM, Wyler J, Milne ENC, Trenchard D, Guz A (1969) Effect of changes in heart rate on left ventricular performance in conscious dogs. Circ Res 24: 285-295 Steiner C, Kovalik AT (1968) A simple technique for production of chronic complete heart block in dogs. J Appl Physiol 25: 631-632 Van den Bos GC, Elzinga G, Westerhof N, Noble MIM (1973) Problems in the use of indices of myocardial contractility. Cardiovasc Res 7: 834-848 Wohlfart B (1979) Relationships between peak force, action potential duration and stimulus interval in rabbit myocardium. Acta Physiol Scand 106: 395-409 The contractile state of cat and dog heart in relation to the interval between beats. J Pidgeon, M Lab, A Seed, G Elzinga, D Papadoyannis and M I Noble Downloaded from http://circres.ahajournals.org/ by guest on June 14, 2017 Circ Res. 1980;47:559-567 doi: 10.1161/01.RES.47.4.559 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1980 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/47/4/559 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/