Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
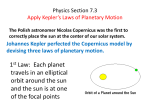
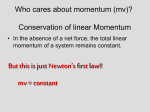
The eye ball & the orbit. • The globe is positioned in the anterior portion of the orbit and constitutes about 20% of the entire volume of the orbit. • It is slightly closer to the lateral orbital wall than the medial wall and is nearer the roof than the floor of the orbit. • At its closest distance to the bony orbit the globe is about 4 mm from the roof, 4.5 mm from the lateral wall, 6.5 mm from the medial wall, and 6.8 mm from the floor. • The lateral orbital rim is considerably recessed compared with the medial orbit, which continues anteriorly to end at the nasal bridge. This leaves approximately one half of the globe unprotected. 1 The bony orbit. 2 3 Bony orbit. Orbital Wall Bones • Superior (roof) = Frontal . • Lateral wall = Zygoma ,Sphenoid (greater wing). • • Inferior (floor) = Maxilla (medial), zygoma (lateral), palatine (posterior). • Medial wall = Maxilla, lacrimal, ethmoid, sphenoid (anterior to posterior). 4 Superior orbital fissure &optic foramen • • • • • • OF=optic foramen. SOF=superior orbital fissure. IOF=inferior orbital fissure. IV=trochlear nerve III=third cranial nerve VI=sixth cranial nerve (the abducent) • L=lacrimal nerve • F=frontal nerve. • N=nasocillary nerve 5 Nerve supply 6 Extraocular muscles 7 ORBITAL CELLULITIS Orbital cellulitis is an acute inflammation of the fatty-cellular tissue of the orbit. Etiology Commonly caused by the spread of infection from the neighbouring areas, erysipelas of the face, ethmoidal sinusitis, lacrimal abscess, stye or suppurating chalazion Rarely direct infection by a penetrating wound, especially if a foreign body is retained within the orbit. Metastatic infection via the blood stream, e.g. in cases of pyaemia. Clinical Picture General.—Fever, malaise and prostration are common symptoms. Sometime cerebral symptoms supervene, namely, delirium, coma and convulsions. Ocular.—The following signs are most important : (a) Severe pain in the orbit which increases during ocular movements. (b) Lid oedema with redness of the skin (c) Chemosis of the conjunctiva. (d) Proptosis which is axial and irreducible. (e) Limitation of ocular movements usually in all directions causing diplopia. (f) Fundus examination may reveal engorged retinal veins and sometimes papillitis. Abscess formation may occur. It may burst through the skin of the eyelids near the orbital margin or in the conjunctival fornix. Complications of Orbital Cellulitis 1. Thrombosis of the cavernous sinus. 3. Panophthalmitis. 2. Meningitis. 4. Optic neuritis. Treatment of Orbital Cellulitis A swab is taken from the conjunctival sac for culture and sensitivity test to available antibiotics. Vigorous systemic and local use of antibiotic drugs to which the causative microorganisms are sensitive, e.g. sulphonamide or any broad spectrum antibiotic. Local heat by frequent hot bathing is very beneficial. If abscess formation is suspected, early incision is recommended. CAVERNOUS SINUS THROMBOSIS is caused by spread of infection from a focus of sepsis in the area drained venous sinus, e.g. orbital cellulitis, erysipelas or septic wounds of the face, middle ear or thrombophlebitis from infection in the mouth, pharynx, paranasal sinuses in the mastoid region. Rarely, cavernous sinus thrombosis may occur from metastatic infection. Clinical Picture General.—There are severe systemic effects, e.g. high fever often associated with rigors, headache, vomiting and drowsiness. Ocular.—The following signs are most important : 1 Severe supraorbital pain due to irritation of the ophthalmic nerve. 2. Marked chemosis of the conjunctiva. 3. Rapidly increasing proptosis. Limitation of ocular movements due to paralysis of the third, the fourth and the fifth cranial nerves, which run in the lateral wall of the cavernous sinus. Congestion of the retinal veins and sometimes papilloedema. Presence of oedema in the mastoid region due to congestion of the emissary vein. Transference of symptoms to the opposite eye occurs in 5O%of cases. The first sign is often paralysis of the opposite external rectus. Complications 1. Meningitis. 2. Pyaemia. 3. Pulmonary abscess caused by a septic embolus. Treatment 1. Intensive antibiotic and sulphonamide therapy. 2. Intravenous anticoagulants. 3. Treatment of the causative focus of sepsis. CHRONIC ORBITAL INFLAMMATIONS CHRONIC NON-SPECIFIC INFLAMMATORY GRANULOMA Chronic Inflammatory Granuloma of the Orbit Orbital pseudotumours comprises a group of space occupying lesions in the orbit resulting from a non-specific granulomatous inflammation, which are difficult to differentiate clinically from orbital tumours. Clinical Picture.—Proptosis and pain are the cardinal features. This is usually associated with edema of the lids, chemosis of the conjunctiva and vascular engorgement often at the insertion of the rectus muscles. Limitation of vertical ocular movements are more frequent than the horizontal ones. Treatment.-Conservative therapy is the rule. Systemic steroids, 40 - 60 mg daily for 1 - 2 weeks usually give dramatic response. The dose is tapered when the condition becomes under control with resolution of pain, proptosis and visual defect. Radiation therapy may shrink the lymphocytic infiltration. DYSTHYROID EYE DISEASE (Endocrine Exophthalmos) The precise cause of dysthyroid eye disease is still obscure. Endocrine orbitopathy is thought to arise from a malfunctioning of the hypothalamic-pituitary-thyroid hormonal axis. More recent studies have been directed to link the dysthyroidism and the ophthalmopathic changes to an immunologic aspect. Ophthalmopathy of dysthyroid eye disease may occur in apparently euthyroid or even hypothyroid patients. Clinically two distinct types of endocrine exophthalmos are usually met with namely, the thyrotoxic and thyrotrophic types. Thyrotoxic Exophthalmos (Graves' Disease) Graves' disease is characterised by hyperthyroid and exophthalmos. The disease occurs often in females between the ages 25-45 year Etiology. —Thyrotoxic exophthalmos was believed to be due to an adrenaline-enhanc ed thyroxine on the alpha receptors situated in the smooth muscle of Muller leading to lid retraction Ocular Clinical Manifestations : 1. Exophthalmos, probably due to an increase in the bulk of the orbital tissue, engorgement of the orbit with the development of oedema, contraction of the muscle of Muller and weakness of the tone of the rectus muscles 2. Lid retraction. 3. Upper lid lag on downward gaze (Von Graefe s sign). 4. Infrequent blinking (Stellwag's sign). 5. Weakness of convergence for near objects (Moebius' sign). 6. Defective eye movements (Ballet's sign). 7. Weak lateral gaze fixation (Suker's sign). 8.Unequal pupillary dilatation (Knie's sign). 9. Jerky pupillary consensual light contraction (Cowen 's sign). 10. Poor forehead wrinkling on upward gaze (Jojfoy's sign). Treatment Local treatment of the ocular changes is extremely important. Protection of the exposed cornea is of prime importance. This is achieved by the instillation of oily antiseptic and lubricants or the use of a perforated transparent eye-shield. Surgical Treatment. —Lateral tarsorrhaphy may be indicated in moderate cases. For severe and progressive cases, radiotherapy and orbital decompression, e.g. orbitotomy via maxillary antrum approach may be indicated. Surgical treatment of extra-ocular muscle abnormalities should usually be performed only after the defective eye movement has be stable for at least six months. Laboratory Assessment of Thyroid Function ORBITAL TUMOURS tumours include tumours of the globe, optic nerve, lacrimal system, other orbital contents and tumours of orbital walls. PRIMARY ORBITAL TUMOURS 1. Developmental Tumours, e.g. dermoid cyst. Dermoid Cyst. —It presents clinically as a cystic swelling at the outer and less commonly the inner, upper angle orbit. The cyst is small, freely mobile and contains sebaceous material and hair follicles. It is often attached to the underlying bone in which a defect can be demonstrated radiologically. 2. Vascular Tumours, e.g. hemangioma. Haemangioma of the Orbit. —It occurs in childhood or early adult life at 9-16 years of age. It produces a slowly developing, painless proptosis which is compressible, sometimes pulsatile but never associated with a bruit. It is usually unassociated with loss of ocular movements. In the most typical cases, proptosis is increased by all circumstances which increase venous congestion, e.g. crying, straining or pressure on the jugular veins. 3. Mesenchymal Tumours, e.g. fibroma and sarcoma. 4. Muscle Tumours, e.g. rhabdomyoma and rhabdomyosarcoma. 5. Hemopoietic Tumours, e.g. Lymphoma, lymphosarcoma, Hodgkin's disease, etc. 6. Nerve Tissue Tumours, e.g. glioma. Glioma of the Optic Nerve.—The majority of cases (88%) occurs before the age of 20 years. There is a very slowly developing painless proptosis. Vision is affected early and severely. This embryonic tumour is an astrocytoma. It assumes a fusiform shape and causes enlargement of the optic foramen which may be demonstrated radiologically. 7. Epithelial Tumours, e.g. carcinoma and melanoma of the lids and the conjunctiva. 25 26 Rhabdomyosarcoma 27 PROPTOSIS Proptosis is a condition in which the eyeball is passively pushed forwards by a bulbar mass, haemorrhage, oedema, inflammatory tissue or neoplasm. However, some cases may give rise to a false impression of proptosis, called pseudoproptosis. Causes of Pseudo-Proptosis : 1. Unilateral Enlargement of the globe : (a) Unilateral axial myopia. (b) Unilateral congenital glaucoma. (c) Unilateral infantile glaucoma. (d) Congenital cystic eyeball. 2. Retraction of the Upper lid from any cause e.g. thyrotoxicosis. 3. Asymmetry of the face or the bony orbits. CAUSES OF PROPTOSIS A. BILATERAL PROPTOSIS Endocrine exophthalmos due to dysthyroid eye disease. Cavernous sinus thrombosis. Metastatic neuroblastoma. Orbital myositis (due to causes other than thyroid dysfunction). B.UNILATERAL PROPTOSIS : 1. Haemangioma. 2. Dermoid cyst. 4. Lymphangioma. 5. Rhabdomyosarcoma. C. -TRANSIENT PROPTOSIS 1. Arterio-venous malformations. 2. Orbital varices. D. -PULSATING PROPTOSIS 1. Vascular Pulsations : Arterio-Venous Aneurysm. —The site of the aneurysm may be in the cavernous sinus (between the internal carotid artery and the cavernous sinus) or, rarely in the orbit (between the ophthalmic artery and an orbital vein). Saccular aneurysm, either of the internal carotid artery in the cavernous sinus or of the ophthalmic artery. Vascular tumours in the orbit either angiomata or highly vascular sarcomata. 2. Cerebral Pulsations : Cerebral pulsations may occur when the orbital wall is defective, e.g. a congenital failure of development of the orbital roof associated with a meningocele or an encephalocele ; or a traumatic or operative hiatus in the orbital roof resulting in the formation of a meningocele. ORBITAL BLOWOUT FRACTURE • Orbital fractures are a relatively common form of periorbital injury. • Although any bone surrounding the orbit may be fractured, the thin bones of the orbital floor and medial orbital wall are most vulnerable. • The most common site for a blowout fracture is the thin part of the maxillary bone (0.5-mm thick) in the posterior medial aspect of the floor. • In addition, the very thin ethmoid bone (0.25-mm thick) along the medial wall of the orbit may be involved • Due to the relative thickness of the orbital rim, it is often spared in orbital fractures. • The term "blowout fracture" refers specifically to a fracture of an orbital wall in the presence of an intact orbital rim. 31 32 33 REFERENCES • Parson’s disease of the eye • Wright interactive ophthalmology. By K.Wright ,1997 on CD. • Lecture notes in ophthalmology. By Bruce James…ninth edition,2003,Blackwell publications. • Duane's ophthalmology ,basic science,on CD,2003 34