Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
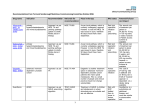
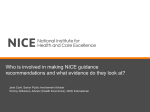
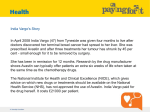
Market Access in Europe Some EU overviews and England as a worked example Christian Hill and Mark Harries MAP BioPharma [email protected] [email protected] [email protected] © MAP BioPharma Limited 2015 Why are there differences amongst Member States? Differential pricing in EU © Can Stock Photo Inc. / RTimages Differences across the EU make Market Access efforts complicated, but are possible with effective coordination Drug Lists HTA requirements (formal like NICE or as part of contract) Contracting Arrangements Country Germany France UK Italy Spain Austria Belgium Czech Republic Denmark Finland Greece Hungary Ireland Netherlands Norway Poland Portugal Sweden Switzerland Positive Negative Price-volume No Yes No Yes No Yes Yes Yes Yes No No Yes Yes Yes Yes Yes Yes Yes Yes Yes No Yes No Yes Yes No No No Yes Yes Yes No Yes NA No No Yes No Possible Yes Possible Yes Possible NA NA No Possible NA Yes Preferred Possible Possible Possible Yes Yes Possible Possible Outcomes based schemes Possible Yes Possible Preferred NA NA NA NA NA NA NA Possible Possible Possible NA NA Possible NA Possible Risk Sharing Possible Possible Yes Yes NA NA NA NA NA NA NA Possible Possible Possible NA Yes Possible NA Possible Clinical Effectiveness, Safety and Budget Impact Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes ICER (cost / QALY) No No Yes No Yes No No Yes NA NA NA Yes Yes Yes NA Yes Yes Yes No Cost Minimisation Analysis Rarely Possible Rarely Possible Yes Possible Rarely Possible NA NA NA Possible Possible Possible NA Possibly Yes Possible No Health Economic Simulation Rarely Emerging Yes Rarely Yes Yes No Yes NA NA NA Possible Yes Yes NA Yes Yes Yes No Differences across the EU • Medicine prices differ across EU due to factors which are often beyond control of companies: – • • Price setting by authorities – national, not EU competence, National health and pharma policies and priorities, Wholesale / pharmacy margins, VAT rates, Pack sizes and distribution channels, Exchange rate fluctuations Member States compare and sometimes reference their prices to other countries prices. Such comparisons must be performed with great caution to avoid unanticipated impact IRP – choice of country basket should take differences between Member States into account: – Purchasing power, GDP per capita; Germany recently decided to include the Czech Republic, Slovakia and Greece in the country basket…The German price is again referenced by 19 other Member States* *P. Kanavos et al for European Parliament, ENVI „Differences in costs of and access to pharmaceutical products in EU”, 2011, p.80 Price Differences between Member States: Reasons and Importance • Nationally dependent variables mean that prices are not directly comparable among Member States – – • • • • • wholesale / pharmacy margins, VAT rates, different pack sizes, distribution channels, exchange rate fluctuations, terms of payment, national price-setting process/outcome by payors governments All of which render any direct comparison inappropriate. Prices are the result of complex evaluation/negotiation processes established by national rules It is essential that the decision-making process for setting the price is objective and transparent which underlines the importance of the Transparency Directive A study by Kanavos et al (2011)1 – price differences largely due to the differences in national priorities (even countries with equivalent income), pharmaceutical policies and market regulation Example of successful differential pricing – vaccines have a differential pricing structure with reasonable market prices in high income countries, low prices in Global Alliance for Vaccines and Immunisations (GAVI) and intermediate prices in middle-income countries2 Danzon and Towse (2003)3 stress that differential pricing allows broader access for patients to innovative products in a sustainable way while promoting innovation 1 P. Kanavos et al for European Parliament, ENVI „Differences in costs of and access to pharmaceutical products in EU”, 2011, available at http://www.europarl.europa.eu/document/activities/cont/201201/20120130ATT36575/20120130ATT36575EN.pdf. 2 P. Yadav, “Differential Pricing for Pharmaceuticals, Review of current knowledge, new findings and ideas for action”, A study conducted for the U.K. Department for International Development (DFID), August 2010, p.28. 3 P.M. Danzon and A Towse (2003), „Differential Pricing for Pharmaceuticals: Reconciling Access, R&D, and Patents" International Journal of Health Care Finance and Economics, 3: 183-205, 2003 Implications of IRP • IRP – acts as a barrier to price adaptation based on a country’s economic situation • IRP mechanically leads to a stronger price convergence • Some practices of cross-border reference pricing can also contribute to a heavy distortion of prices especially in times of financial crisis e.g. Greece! • This is especially the case in countries where the price is set based on the lowest price in the country basket rather than on the average price in the country basket. • Some practices of IRP may spill-over onto other countries and decrease the global incentives to innovate • Companies may also consider the impact of launching a product in one country on the revenues of the other country Trends and the Future • Austerity is increasingly leading to restrictive pricing policy – • Transparency directive – – • • • These countries should be excluded from country baskets as those prices / rebates are set under exceptional circumstances, may be temporary and should not be exported to other countries Official list prices are already made public by Member States The directive is aimed at guaranteeing transparent procedures and payor decisions for pharmaceutical companies, not final prices Ultimately, when IRP policy is aggressive, it directly impacts profitability of product launch Such developments impact the revenues of pharmaceutical companies but also act as a delay to patient access to innovative treatments. The ESMT White Paper (p.17) finds that fewer projects are developed in lowmargin therapeutic areas It is essential to balance the impact of lower prices with the costs associated with less innovation and with fewer products being launched1 1H. Friederiszick, N. Tosini, F. de Véricourt, S. Wakeman, ESMT White Paper, „An Economic Assessment of the Relationship between Price Regulation and Incentives to Innovate in the Pharmaceutical Industry, 2010, available at http://www.esmt.org/en/271562 Price level index for pharmaceutical products in 2005, EU25=100 Source: European Commission Directorate-General for Economic and Financial Affairs (DGECFIN); Costcontainment policies in public pharmaceutical spending in the EU By Giuseppe Carone et al 2012 Simulated savings due to a price convergence of countries with above EU level prices to EU level prices Source: European Commission Directorate-General for Economic and Financial Affairs (DGECFIN); Costcontainment policies in public pharmaceutical spending in the EU By Giuseppe Carone et al 2012 Germany – an example of free pricing at launch but a challenging process overall • Germany is the largest EU state by population, the largest EU economy and accordingly the most important market for pharmaceuticals within the European Union. For a long time manufacturers were effectively free to determine the reimbursement price of patented drugs in the German health care system. In recent years, however, pricing and reimbursement in Germany has changed significantly. In January 2011 a new system was introduced to determine the reimbursement prices of new active substances entering the German market. This new system, known as the “AMNOG-System” foresees a 2-step procedure which new medicines have to undergo as soon as they enter the German market. • The AMNOG-System is a quite recent concept (est. 2011) and is considered to be a “learning system” by the German legislator and the administrative bodies involved. Also, in some parts the legal framework governing the system is not very dense and leaves room for interpretation. Accordingly, many aspects are still being shaped and substantiated by court decisions, law decrees and, most of all, the administrative practice of the authorities involved. This website has been designed to support you when navigating the system to prepare the successful launch of innovative pharmaceuticals in Germany. • In 2012-2014, G-BA assessed 99 new technologies and decided 48% of products had no additional benefit, 25% had minor additional benefit, 18% had considerable additional benefit and the remainder had unquantifiable additional benefit. No technologies have been classified as having major additional benefit. • A high proportion of G-BA decisions have been of no or unquantifiable benefit indicating that obtaining a high price in Germany is challenging The UK A more detailed review Topics 1. An alternative guide to the NHS 2. It’s not as bad as you think though 3. Financial background to medicines in UK 4. NICE consultations, long grass and the doughnut 5. Rare diseases, HST and Chinese whispers © MAP BioPharma Limited 2014 Alternative guide to the NHS http://www.kingsfund.org.uk/projects /nhs-65/alternative-guide-new-nhsengland It’s not as bad as you think: Compare us to the US http://kevinbrady.house.gov/uploade dfiles/obamacarechart.pdf PPRS context (pricing agreed on behalf of all UK nations) Total medicines expenditure / growth Figure 13. Elements driving the change in total medicines expenditure (£ million): Baseline scenario 16,000 2,444 15,592 15,500 15,000 168 629 £m per annum 14,500 13,581 558 14,000 -353 13,500 13,000 -1,435 12,500 12,000 11,500 2011 Start and end Substitution Biosimilars Overall underlying growth Source: Authors’ estimates Future launches Generic entrants LoE products 2015 Projecting Expenditure on Medicines in the NHS ; Phill O’Neilla, Jorge Mestre-Ferrandiza, Ruth Puig-Peirob and Jon Sussexa ; OHE Research Paper 13/02 April 2013 Each of the three other nations in the UK has a slight variation on the English model which impacts on market access Although funded centrally from national taxation, NHS services in England, Northern Ireland, Scotland and Wales are managed separately Northern Ireland: • Funded by the NI Executive through its Health Department • The Health and Social Care Board (HSCB) manage funding, commission services, and work with the HSC trusts • The 6 HSC trusts are responsible for management of services at a local & regional level Southern Ireland: • The Health Service Executive (HSE), responsible for provision of healthcare in Ireland, follows guidance from the National Centre for Pharmacoeconomics (NCPE) Wales: • Managed through 7 local health boards (LHBs), each deliver NHS services for local area • Wales follow NICE and AWMSG guidance Scotland: • Managed through 14 health boards • GPs and pharmacy are contracted through health board but work in community health partnerships based on local authority boundaries • Guidance from SMC and SIGN • MTA Guidance from NICE English NHS Organisation – an enormous organisation © MAP BioPharma Limited 2014 There are two broad stages to successful market access in England 1. National market access 2. Market access commercialisation Launch Phase II/III Key desired outcomes Positive NICE (HTA*) and associated national implementation incentives * HTA = Health Technology Assessment Local action plan to adopt new product Desired rate of commercial uptake Stage 1 National market access begins pre-phase III and continues after launch Go/ no go decision Before start of phase III or -4 years launch On start of phase III or -3 years launch Go/ no go decision -6 months launch Key desired outcome: positive NICE HTA and associated national implementation incentives Post-launch, pre-NICE & post-NICE Launch +3 months Launch +12-18 months Outcomes/ milestones: 1. 2. Ensure appropriate endpoints for EMEA and 3. HTA included in Phase III 4. Selection for NICE appraisal Flagged for NICE guidelines On radar of national service development makers On radar of national clinical opinion leaders Patient Access Scheme (PAS) price approved Favourable position in regional HTA guidance Favourable position in NICE HTA Favourable position in NICE guidelines, quality standards, and incentives e.g. Quality Outcomes Framework (QOF), commissioning for Quality & Innovation (CQUIN) & National Clinical Guidelines Stage 1 …with a range of decision makers and influencers requiring a joined-up approach across the UK operating company… Before start of phase III or -4 years launch Ensure appropriate endpoints for EMEA and HTA included in Phase III NICE Decision makers & influencers: Typical activities should include: • Global ad boards 1. 2. 3. 4. On start of phase III or -3 years launch Selection for NICE appraisal Flagged for NICE guidelines On radar of national service development makers On radar of national clinical opinion leaders -6 months launch Patient Access Scheme (PAS) price approved NICE PharmaScan National Horizon Scanning Centre (NHSC) Department of health (DoH) Patient Access Scheme Liaison Unit (PASLU) • Input data into PharmaScan etc. • Ad board to understand reallife NHS affordability/ positioning • Meetings with NHSC • 1:1 national advocacy development • Direct contact with DoH, PASLU • Negotiating price with Global Post-launch, pre-NICE & postNICE Launch +3 months Favourable position in regional HTA guidance Favourable position in NICE HTA PenTAG, GMMMG, Keele, UKMi etc. Academic pharmacists, KOLs NICE Academics decision support units, patient groups, KOLs, Royal Colleges • Direct contact with organisations • Write submissions (9-12 months) • Bespoke submissions • 1:1s and meetings to create bespoke messages for all stakeholder groups Launch +12-18 months Favourable position in NICE guidelines, quality standards, and incentives e.g. Quality Outcomes Framework (QOF), commissioning for Quality & Innovation (CQUIN) & National Clinical Guidelines NICE Co-opted KOLs National KOLs • Co-ordinating processes & feedback with commissioners • National advocacy development Stage 2 Focussed multi-disciplinary market access commercialisation is then essential to drive the desired rate of product uptake Go/ no go decision -6 months – 2 years to launch during NHS annual planning cycle deadlines Milestones: Local NHS planning cycle has new product on radar and associated impact on budget service configuration planning and local priorities Key outcome: desired rate of commercial uptake 0-90 days + 3 months post NICE Local action plan agreed on how product is to be developed For each planning cycle Decision makers & influencers: Local CCG/ CSU PharmaScan, national horizon scanning & regional HTA groups, local clinical KOLs • Continue to input data into PharmaScan etc. Typical activities: • Continue direct contact with regional HTA • Stakeholder mapping & prioritisation of local accounts • 1:1 activity with MM & lead commissioners using ABN 6-36 months post launch Implementation and monitoring support Review in light of each new competitor Local CCG/ CSU NICE & regional HTA groups, local clinical KOLs • Face to face activity from hybrid clinical/ payer role • Tools to help payers identify local cost implications e.g. BIM • Tools to support formulary inclusion (which will be mandated) • Payer educational materials on key concepts for evaluating • Proactive support and facilitation of creating costed pathways, business cases & service re-design Local CCG/ CSU & clinical team as agreed in local plan • On going clinical/ payer field role face-to-face with MDT • Support on monitoring progress, real world data, case studies, learning sets • Educational support • Joint working and partnership working The roadmap for new medicines in NHS England may not always be obvious – specialised medicines for example have a range of routes to reimbursement NICE Highly Specialized Technologies (HST) Programme Commissioning Policy © Can Stock Photo Inc. / RTimages NICE Single Technology Appraisal (STA) Cancer Drugs Fund (CDF) Individual Funding Requests (IFRs) Commissioning Through Evaluation Strategically there are many things to be considered as to which direction you may or may not want to go What do NICE do? NICE - Explaining what was meant to change in 2014 • • • Proposed addition of burden of illness and wider societal impact These value elements are described as ‘modifiers’ NICE Appraisal Committees use these modifiers to help decide whether to recommend a technology with an incremental cost effectiveness ratio above £20,000 per QALY UK example of a changing environment: Wider societal impact now kicked into the long grass Current UK evaluation requirements: • NHS and personal social services (PSS) perspective • No societal costs included • All societal benefits included (e.g. carer disutility) The Netherlands evaluation requirements • Societal perspective • Some societal costs: patient productivity losses and unpaid carer costs • All societal benefits included (e.g. carer disutility) Sweden evaluation requirements: • Societal perspective • All societal costs: patient productivity losses and consumption; unpaid carer costs • All societal benefits included (e.g. carer disutility) VBA UK evaluation requirements: • Societal perspective • Weightings based on BoI • Wider societal impact based on patient ability to engage with society Adapted from a slide provided courtesy of FIECON Ltd NHS England Consultation – Issued 27 January 2015 90 day consultation period £14bn In prioritising treatments and interventions for the future financial year, NHS England will observe the following sequence • First Order – NICE TA and HST – Estimated budget impact for NICE approvals in 2015/16 = £270m • Second Order – NHS Constitution delivery requirements which affect specialised services e.g. 18-week wait • Third Order – Developments to support national service strategies e.g. increase access to transplantation • Fourth Order The Cancer Drugs Fund – All other specialised services developments currently remains outside Five stages have for treatments and interventions that might typically be commissioned 5. Governance 1. Scanning 3. Building the clinical case 4. Impact analysis and consultation 2. Planning NHS England. Consultation Guide Investing in Specialised Services. 27 January, 2015 https://www.engage.england.nhs.uk/consultation/investing-in-specialised-commissioning/supporting_documents/invspecservconslt.pdf Five stages have for treatments and interventions that might typically be commissioned • Coordinated at a Clinical Reference Group level – There are two published outputs from this stage • The list of potential clinical policies that are identified as ‘Not being routinely commissioned’ • The list of potential service specifications for commissioning 1. Scanning Five stages have for treatments and interventions that might typically be commissioned • Where the National Programmes of Care, who coordinate the work of the CRGs into strategic groupings such as cancer, consider the proposals and select the ones that most fit the programme’s strategic priorities • This will create an Annual Work Programme 2. Planning Five stages have for treatments and interventions that might typically be commissioned • Building the clinical case: where the Clinical Reference Group works with stakeholders, including patients and the public, to define the clinical proposal • An independent review of clinical evidence will usually be commissioned • Finally, a Clinical Appraisal Panel will form a view whether a clinical case is made 3. Building the clinical case Five stages have for treatments and interventions that might typically be commissioned • Where NHS England will develop, using the defined clinical criteria, a service impact analysis and hence a financial impact analysis • This will result in a final policy or service specification that can be considered for commissioning • The scale and duration of consultation will then be defined • Suite of 6 documents 1. 2. 3. 4. 5. 6. Provisional service specification Activity projection report Service impact analysis report Finance impact analysis report Draft specification Engagement report 4. Impact analysis and consultation Five stages have for treatments and interventions that might typically be commissioned • Where the Clinical Priorities Advisory Group assures the Board that the process has been completed and recommends a priority order of commissioning • The NHS England Board approves the prioritisation • Commissioning against the priorities will be overseen by the Specialised Commissioning Committee 5. Governance NHS England latest draft of the specialised commissioning information pack – our concerns • Equity – 'NHS England will not confer higher priority to a treatment or intervention solely on the basis it is the only one available.’ – This seems to be disenfranchising patient groups that currently have ‘no hope’ – Seems inconsistent with the DH’s own 'innovation health and wealth’ strategy • Timeframe and backlog – NHS England has openly struggled with the backlog of proposed commissioning policies and service developments – We welcome the transparent way that the process is laid out – But framework should not be paralysing NHS England latest draft of the specialised commissioning information pack – our concerns • NICE collaboration – The CRG accountable commissioner will be expected to confirm that there is no planned or in progress NICE appraisal – Little evidence of consistency between the NICE appraisal process and that of the NHS specialised services review process – Companies left with the need to plan for both, due to lack of predictability of the system • Appeal – 'The decision itself cannot be appealed.’ and 'A challenge that the correct process has not been followed should be made in letter to the Director of Specialised Commissioning.’ – Not clear how such a challenge would be handled and suggests that only a ‘Judicial Review’ style of appeal would be an option? In conclusion • Challenging – companies slowing down their access efforts to ‘test’ markets first • Unpredictable – companies looking to other markets first • Most important things are: 1. 2. 3. Comparators choosing the wrong one or PBO as comparator can lead to perception of no or little benefit Clinical outcomes in terms of some surrogates vs. validated or mortality measures – are outcomes meaningful? Price – it’s not the most important thing, but it becomes increasingly important without 1 and 2 Thanks to MAP BioPharma for source material Christian Hill and Mark Harries MAP BioPharma [email protected] [email protected] © MAP BioPharma Limited 2014