Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
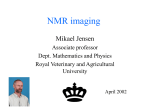
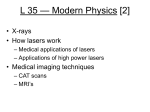
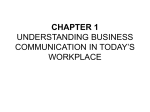
new england journal of medicine The established in 1812 November 3, 2016 vol. 375 no. 18 Acute Neurologic Disorder from an Inhibitor of Fatty Acid Amide Hydrolase Anne Kerbrat, M.D., Jean‑Christophe Ferré, M.D., Ph.D., Pierre Fillatre, M.D., Thomas Ronzière, M.D., Stéphane Vannier, M.D., Béatrice Carsin‑Nicol, M.D., Sylvain Lavoué, M.D., Marc Vérin, M.D., Ph.D., Jean‑Yves Gauvrit, M.D., Ph.D., Yves Le Tulzo, M.D., Ph.D., and Gilles Edan, M.D., Ph.D. a bs t r ac t BACKGROUND A decrease in fatty acid amide hydrolase (FAAH) activity increases the levels of endogenous analogues of cannabinoids, or endocannabinoids. FAAH inhibitors have shown analgesic and antiinflammatory activity in animal models, and some have been tested in phase 1 and 2 studies. In a phase 1 study, BIA 10-2474, an orally administered reversible FAAH inhibitor, was given to healthy volunteers to assess safety. METHODS Single doses (0.25 to 100 mg) and repeated oral doses (2.5 to 20 mg for 10 days) of BIA 10-2474 had been administered to 84 healthy volunteers in sequential cohorts; no severe adverse events had been reported. Another cohort of participants was then assigned to placebo (2 participants) or 50 mg of BIA 10-2474 per day (6 participants). This report focuses on neurologic adverse events in participants in this final cohort. A total of 4 of the 6 participants who received active treatment consented to have their clinical and radiologic data included in this report. RESULTS An acute and rapidly progressive neurologic syndrome developed in three of the four participants starting on the fifth day of drug administration. The main clinical features were headache, a cerebellar syndrome, memory impairment, and altered consciousness. Magnetic resonance imaging showed bilateral and symmetric cerebral lesions, including microhemorrhages and hyperintensities on fluid-attenuated inversion recovery and diffusion-weighted imaging sequences predominantly involving the pons and hippocampi. One patient became brain dead; the condition of two patients subsequently improved, but one patient had residual memory impairment, and the other patient had a residual cerebellar syndrome. One patient remained asymptomatic. From the Departments of Neurology (A.K., T.R., S.V., M.V., G.E.), Radiology (J.-C.F., B.C.-N., J.-Y.G.), and Infectious Diseases and Medical Intensive Care (P.F., S.L., Y.L.T.), Centre d’Investigation Clinique–Plurithématique, INSERM 1414 (P.F., Y.L.T., G.E.), and EA 4712 Comportement et Noyaux Gris Centraux Laboratory (M.V.), Rennes University Hospital, and the Vision, Action, and Information Management System in Health team, Institut National de Recherche en Informatique et en Automatique (A.K., J.-C.F., J.-Y.G.) — all in Rennes, France. Address reprint requests to Dr. Edan at CHU Hôpital Pontchaillou, 2 rue Henri Le Guilloux, 35033 Rennes CEDEX 9, France, or at gilles.edan@chu-rennes.fr. N Engl J Med 2016;375:1717-25. DOI: 10.1056/NEJMoa1604221 Copyright © 2016 Massachusetts Medical Society. CONCLUSIONS An unanticipated severe neurologic disorder occurred after ingestion of BIA 10-2474 at the highest dose level used in a phase 1 trial. The underlying mechanism of this toxic cerebral syndrome remains unknown. n engl j med 375;18 nejm.org November 3, 2016 1717 The n e w e ng l a n d j o u r na l A decrease in fatty acid amide hydrolase (FAAH) activity increases the levels of endogenous analogues of cannabinoids, or endocannabinoids.1 FAAH inhibitors have shown analgesic and antiinflammatory activity in animal models,2 and some have been tested for these purposes in phase 1 and phase 2 studies.3 Phase 3 studies were not pursued owing to a lack of efficacy. BIA 10-2474, with the chemical name 3-(1-(cyclohexyl(methyl)carbamoyl)-1H-imidazol4-yl)pyridine 1-oxide, is a new reversible FAAH inhibitor. A phase 1 study was conducted in healthy volunteers to explore the safety profile of BIA 10-2474. Five of the six participants who had received the highest cumulative dose had an acute and rapidly progressive neurologic syndrome.4 Me thods Trial Conduct BIA 10-2474 was developed by Bial, a Portuguese pharmaceutical company. The research trial was conducted by Biotrial, a contract research organization that has been approved by the French Health Ministry. This was the first randomized, double-blind, placebo-controlled study of BIA 10-2474 involving humans. Sequential cohorts of 8 participants (6 assigned to the active agent and 2 assigned to placebo) were enrolled. A single ascending dose of BIA 10-2474 (0.25 mg, 1.25 mg, 2.5 mg, 5 mg, 10 mg, 20 mg, 40 mg, and 100 mg) had been administered to 48 healthy volunteers. A multiple ascending dose of BIA 10-2474 (2.5 mg for 10 days, 5 mg for 10 days, 10 mg for 10 days, and 20 mg for 10 days) had been administrated to 24 healthy volunteers. A total of 12 other participants, who were enrolled in an additional cohort to study food interaction, received 40 mg of BIA 10-2474. Therefore, BIA 10-2474 had been administered to 84 healthy volunteers between July 2015 and December 2015, and no serious adverse events had been reported. In January 2016, the fifth multiple-dose cohort of 8 participants was studied; 2 received placebo and 6 received 50 mg per day of BIA 10-2474. This report focuses on the adverse events in the patients in this final cohort. of m e dic i n e obtained from all the volunteers by Biotrial. Of the six participants who received active treatment in the final study cohort, three participants and the family of the deceased participant provided written informed consent for their inclusion in this report. Two participants who received active treatment in the final cohort of eight volunteers declined to be included in this report. This article thus reports on the clinical and radiologic findings of four of the six participants. They were transferred from the Biotrial clinical research facility to Centre Hospitalier Universitaire Hôpital Pontchaillou (Rennes University Hospital) after the occurrence of neurologic disorders (three participants) or for systematic monitoring (one participant). During the past 5 years, in its capacity as a contract research organization, Biotrial had conducted research at Rennes University Hospital that involved the Departments of Neurology and Radiology (studies of mitoxantrone–interferon beta-1a and of biotin). Biotrial also provides financial support to Institut des Neurosciences Cliniques de Rennes, which funds academic research projects on brain diseases in Rennes. The authors of this report are employed by Rennes University Hospital but were not involved in the conduct of the phase 1 study of BIA 10-2474. R e sult s Patients The four patients who were transferred to Rennes University Hospital were previously healthy men, 27 to 49 years of age. No major clinical or surgical history and no history of drug abuse were reported at screening. They were taking no medication other than the study drug. At the time of the patients’ admission to the hospital, analyses for amphetamines, barbiturates, benzodiazepines, cannabinoids, cocaine, and opiates were negative. Two of the four patients had previously participated in phase 1 studies testing molecules that were not related to the endocannabinoid system. The first day of drug administration (day 1) was January 6, 2016; clinical follow-up extended to 55 days. A 50-mg dose of BIA 10-2474 was Participants and Study Oversight administered orally to each patient between 8 a.m. The trial was approved by the institutional review and 8:45 a.m. each day; Patient 1 received the board of Brest on June 23, 2015. Written in- drug for 5 consecutive days, and Patients 2, 3, and formed consent for participation in the trial was 4 for 6 consecutive days. The first serious adverse 1718 n engl j med 375;18 nejm.org November 3, 2016 Acute Neurologic Disorder from an FA AH Inhibitor Table 1. Clinical Data for the Four Patients.* Variable Patient 1 Patient 2 Patient 3 Patient 4† Age (yr) 49 38 42 27 Cumulative dose of BIA 10-2474 (mg) 250 300 300 300 First symptoms 5 7 5 — Admission to the hospital 5 7 8 — Peak of symptoms 9 9 10 — Blurred vision, headache Anterograde amnesia, headache Dizziness, headache None Sequence of neurologic symptoms (days after treatment initiation) Description of neurologic symptoms First neurologic symptoms Subsequent neurologic symptoms Headache Severe Mild Moderate — Gait disturbance Severe Mild Severe — Slurred speech Severe Mild Severe — Dizziness Severe — Severe — Blurred vision Severe — Severe — Description of neurologic signs Altered consciousness Somnolence — Mild Moderate — Severe — — — Anterograde amnesia NA Severe — — Retrograde amnesia NA Mild — — Coma Amnesia Cerebellar syndrome Limb ataxia Severe Mild Severe — Gait ataxia Severe Mild Severe — Postural ataxia Severe Mild Severe — Dysarthria Severe Mild Severe — Nystagmus Severe — Moderate — No 1 g/day for 5 days 1 g/day for 3 days No Glucocorticoid treatment at admission *NA denotes not available owing to severely altered consciousness. †Patient 4 had no neurologic symptoms or signs. event was reported on day 5. Clinical and radio- University Hospital at 8:50 p.m. The physician in logic data are summarized in Tables 1 and 2. the emergency department described moderate limb ataxia, which was worse on the left side, inPatient 1 volving the arm and leg equally; moderate cerebelAt 11 a.m. on day 5, Patient 1 reported moderate lar dysarthria; and gaze-evoked and directionblurred vision and floating specks. At 3:30 p.m., changing nystagmus. The patient was awake and he reported moderate headache. When gait dis- had no sensory loss, weakness, oculomotor paralyturbance and slurred speech developed, he was sis, Babinski sign, reflex alteration, or memory transferred from the Biotrial clinical research defect. The temperature was 36.4°C, heart rate 62 facility to the emergency department of Rennes beats per minute, blood pressure 149/89 mm Hg, n engl j med 375;18 nejm.org November 3, 2016 1719 The n e w e ng l a n d j o u r na l of m e dic i n e Table 2. Description of Magnetic Resonance Imaging Abnormalities in the Four Patients.* Variable Patient 1 Day 6 Patient 2 Day 8 Day 7 Day 8 Patient 3 Day 9 Day 8 Patient 4 Day 9 Hyperintense lesions on diffusion-weighted images Pons Hippocampus Amygdala Mammillary bodies No Severe Severe Moderate Severe Severe Mild Mild Mild Severe Mild Moderate Moderate Moderate Moderate — Severe Mild Moderate Moderate — Mild Moderate Severe — Moderate Moderate — — Cortex — Severe — — — — — Thalamus — Severe — — — — — External capsule — Severe — — — — — Pathologic hypersignal on FLAIR images Pons Hippocampus NA No Severe Severe Severe Severe Severe Severe Moderate Severe Severe Severe Moderate Moderate Amygdala Moderate Severe Moderate Moderate — — Mammillary bodies Moderate Severe Moderate Moderate — — Medulla oblongata Mild Severe — — Mild Mild Moderate Severe — — — — Anterior temporal lobe — Severe Mild Mild — — Cortex — Severe — — — — Thalamus — Severe — — — — Midbrain Microhemorrhages on susceptibility-weighted images Pons Hippocampus Amygdala Medulla oblongata Day 8 NA No Severe Severe Mild Moderate Mild Moderate Moderate Severe Mild Moderate — Mild — Severe Mild Moderate Mild Mild Mild Moderate — — — — Midbrain — Moderate — — — — Cortex — Severe — — — — External capsule — Severe — — — — Basal ganglia — Severe — — — — *FLAIR denotes fluid-attenuated inversion recovery, and NA not available. and oxygen saturation 95% while the patient was breathing ambient air. A cranial computed tomographic (CT) scan and a CT angiogram were initially interpreted as normal. A subtle hypodensity in the pons could be seen, retrospectively. The complete blood count and blood levels of electrolytes, urea, creatinine, and C-reactive protein (CRP) were normal, as were the results of coagulation and liver-function tests. The patient received 160 mg of aspirin. At 7:45 a.m. on day 6, he suddenly became confused and agitated, and 1720 he had worse limb and postural ataxia with severe dysmetria, limb and truncal kinetic tremor, and an inability to sit up in bed. Magnetic resonance imaging (MRI) (Fig. 1) showed hyperintensities in the pons and hippocampi on fluid-attenuated inversion recovery (FLAIR) and diffusion-weighted sequences, with multiple microhemorrhages in the pons. As the patient’s condition deteriorated further, he became unconscious (Glasgow Coma Scale score of 9, on a scale from 3 to 15, with lower scores indicat- n engl j med 375;18 nejm.org November 3, 2016 Acute Neurologic Disorder from an FA AH Inhibitor A B C E F G I J D H K Figure 1. Magnetic Resonance Imaging (MRI) Studies in Patient 1. Panels A through F depict MRI studies from day 6, and Panels G through K depict studies from day 8. On day 6, MRI showed hyperintense lesions (thin arrows) on diffusion-weighted images in the pons (diffuse lesion; Panel A) and right hippocampus (punctate lesion; Panel D), microhemorrhages (thick arrows) on susceptibility-weighted images in the pons (Panel B) and hippocampi (Panel E), and pathologic hypersignal (arrowhead) on fluid-attenuated inversion recovery (FLAIR) images in the pons (Panel C) and midbrain (Panel F). On day 8, MRI showed worsening of lesions: hyperintense lesions on diffusion-weighted images involving mainly the cortex, external capsula, thalami (Panel J) and the pons, hippocampi, amygdala, and mammillary bodies (not shown); microhemorrhages on susceptibility-weighted images in the hippocampi, amygdala, external capsula, all the basal ganglia, and the cortex (Panels G, H, and I); and pathologic hypersignal on FLAIR images in the cortex, thalami (Panel K), and the brain stem, hippocampi, and amygdala (not shown). ing a reduced level of consciousness; the pupils were symmetric and reactive to light), and he required tracheal intubation and mechanical ventilation with sedation. The temperature became elevated to 38.2°C. The cerebrospinal fluid had 173 white cells per cubic millimeter (87% of which were neutrophils), a protein level of 353 mg n engl j med 375;18 per deciliter, and a glucose level of 4.58 mmol per liter; the serum glucose level was 8 mmol per liter (144 mg per deciliter). He received acyclovir, cefotaxime, and amoxicillin until cerebrospinal fluid studies for herpes simplex virus, varicella virus, and Listeria monocytogenes were determined to be negative. Levels of antinuclear antibodies, nejm.org November 3, 2016 1721 The B A D n e w e ng l a n d j o u r na l of m e dic i n e C E F G Figure 2. MRI Studies in Patient 2. A time series of diffusion-weighted images on day 7 (Panel A), day 8 (Panel B), and day 9 (Panel C) shows progressive worsening of hyperintense lesions in the hippocampi and amygdala. MRI on day 9 (Panels C through G) showed several moderate microhemorrhages (thick arrows) on susceptibility-weighted images in the median part of the pons (Panel D) and in the hippocampi and amygdala (Panel E) as well as pathologic hypersignal (arrowhead) on FLAIR images in the pons and anterior temporal lobe (Panel F) and in the hippocampi and amygdala (Panel G). complement, and ADAMTS13 (a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13) were normal, and there were no signs of thrombotic microangiopathy. On day 7, the patient’s heart rate was slower than 40 beats per minute, and he was hypotensive. A CT scan showed edema of the brain stem, hippocampi, and temporal lobes. On day 8, he had bilateral dilated and light-unreactive pupils. MRI showed diffuse hyperintense lesions on FLAIR and diffusion-weighted sequences and multiple microhemorrhages, mainly involving the brain stem, hippocampi, cortex, and thalamus. He was declared brain dead the following day. An autopsy was performed, but the results have not been made available to the authors. Patient 2 On day 7, Patient 2 began asking the same questions repeatedly about recent activities. He was transferred from the Biotrial clinical research facility to the emergency department of Rennes 1722 n engl j med 375;18 University Hospital. A neurologic examination was performed by the on-duty neurologist. The patient was incapable of encoding new facts, events, or names. Although the retrieval of information from years ago was relatively preserved, his memory for the previous 2 to 3 months was incomplete. He reported moderate headache. Brain MRI showed hippocampal and anterior pontine signal hyperintensities on diffusion-weighted sequences (Fig. 2). The complete blood count and blood levels of electrolytes, urea, creatinine, and CRP were normal, as were the results of coagulation and liver-function tests. On day 8, he had moderate dysarthria and moderate limb and gait ataxia (he was incapable of walking in a straight line). A second MRI scan showed hyperintense lesions on FLAIR and diffusion-weighted sequences and several microhemorrhages involving the pons and hippocampi. The patient received intravenous glucocorticoids from day 8 to day 12. On day 9, his condition was unchanged. A third MRI showed an increased nejm.org November 3, 2016 Acute Neurologic Disorder from an FA AH Inhibitor A B C D E F G H Figure 3. MRI Studies in Patient 3. MRI on day 8 showed hyperintense lesions (thin arrows) on diffusion-weighted images in the pons (Panel A), several microhemorrhages (thick arrows) on susceptibility-weighted images in the median pons (Panel B), and pathologic hypersignal (arrowhead) on FLAIR images in the pons (Panel C) and hippocampi (Panel D). MRI on day 9 showed punctate hyperintense lesions (thin arrows) on diffusion-weighted images in the hippocampi and amygdala (Panel E), worsening of existing microhemorrhages (thick arrows) on susceptibility-weighted images in the median pons (Panel F) as well as new microhemorrhages in the hippocampi and amygdala (Panel G), and pathologic hypersignal (arrowhead) on FLAIR images (Panel H) in the pons, anterior part of the medulla oblongata, and the hippocampi (not shown). number of microhemorrhages. His condition gradually improved, and at the last clinical follow-up, on day 55, his amnesic symptoms had lessened, but he had partial retrograde amnesia regarding the period from 2 months before to 1 month after administration of the drug and minimal anterograde amnesia. Dysarthria and ataxia were no longer evident. MRI showed that the diffusion-weighted hyperintensities had disappeared and that the FLAIR hyperintensities had partially regressed (Fig. S1 in the Supplementary Appendix, available with the full text of this article at NEJM.org). The hippocampi had heterogeneous signal hyperintensities, and some focal hyperintensities were still visible in the pons on FLAIR images. No new lesion had appeared. Patient 3 On day 5, Patient 3 reported mild asthenia, headache, and dizziness, but repeated neurologic examinations performed by the physician at the Biotrial clinical research facility were normal. At n engl j med 375;18 7:38 a.m. on day 8, he presented with a subacute gait disturbance, slurred speech, and a syncope. He was transferred from the Biotrial facility to the emergency department of Rennes University Hospital. A neurologic examination was performed by the on-duty neurologist. The patient was somnolent and had severe limb, gait, and postural ataxia (he was unable to walk or sit up in bed without assistance) and moderate dysarthria. No sensory or motor disturbances (including oculomotor paralysis) and no memory defects were found. Nystagmus (gaze-evoked and direction-changing) subsequently appeared. The headache ceased. The results of blood tests were normal. MRI showed hyperintensities on diffusion-weighted and FLAIR sequences in the brain stem (pons and medulla oblongata) and hippocampi and a focal microhemorrhage in the pons (Fig. 3). The cerebrospinal fluid had a protein level of 1.13 g per liter but no white or red cells. He received intravenous glucocorticoids from day 8 to day 10. On day 9, the cerebellar syndrome was unchanged. On day 10, he had severe nejm.org November 3, 2016 1723 The n e w e ng l a n d j o u r na l dysarthria and somnolence. He was given 1 g of intravenous cyclophosphamide. His condition gradually improved beginning on day 11, and he could walk without assistance on day 13. At the last clinical follow-up on day 55, he was able to walk without assistance but had difficulty with tandem gait and had nystagmus on left lateral gaze. MRI showed that the diffusion-weighted and FLAIR hyperintensities in the medulla oblongata and hippocampi had disappeared (Fig. S2 in the Supplementary Appendix). Focal hyperintensities were still visible in the pons on FLAIR images, as were micro hemorrhages. Patient 4 Patient 4 had moderate diarrhea on days 6 and 7. MRI scans on days 8 and 10 were normal, except for an asymptomatic cavernous malformation located in the brain stem. On day 55, he remained asymptomatic. Discussion The healthy volunteers described in this article participated in a phase 1 study of BIA 10-2474, a new FAAH inhibitor. They had received the highest cumulative dose (250 to 300 mg) administered to humans. A total of 84 healthy volunteers had previously received cumulative doses of up to 200 mg of BIA 10-2474. No clinical severe adverse event had been reported. The product contained in the capsules administered to all the volunteers was the same as that used for the toxicology studies, and assays confirmed that it was of high purity.4 These data suggest that the toxic effects we observed were related to drug accumulation. This hypothesis is supported by the nonlinear pharmacokinetics of BIA 10-2474 for doses higher than 40 to 100 mg.4 The clinical syndrome in these patients was an acute and rapidly progressive central nervous system disorder with limb, gait, and postural ataxia as well as dysarthria and nystagmus, all of which are compatible with a cerebellar syndrome; amnesia compatible with medial temporal amnesia; headache; and altered consciousness. Consistent with these clinical signs and symptoms, the lesions on MRI involved mainly the pons and hippocampi, bilaterally and symmetrically. The cerebellar syndrome can be explained by lesions in the cerebellar peduncles of the crossing cerebellar fibers at the pontine and 1724 of m e dic i n e mesencephalic levels, because the cerebellum was not directly affected on MRI. Thalamic and cortical lesions were seen in Patient 1 and had radiologic characteristics that were similar to those of the pontine and hippocampal lesions; these findings suggest that a similar pathophysiological process took place that was restricted mostly to gray matter in many regions of the brain. The MRI findings included microhemorrhages on susceptibility-weighted images and hyperintensities on FLAIR and diffusion-weighted images. The diffusion hyperintensities may have been related to vasogenic or cytotoxic edema. The apparent diffusion coefficient usually helps to differentiate between vasogenic and cytotoxic edema. However, because the microhemorrhages disrupted the signal, apparent-diffusion-coefficient maps could not be reliably used to characterize the underlying mechanism. The meningitis reported in Patient 1 may have been from severe brain-tissue injury, but it is possible that there was an inflammatory component to the toxic syndrome. No meningitis was found in the other patient who underwent a lumbar puncture and who had a milder form of the syndrome (Patient 3). The syndrome was partially reversible in Patients 2 and 3, and the potential benefit of early high-dose glucocorticoid infusion remains an open question. Long-term clinical and MRI follow-up of the surviving patients is planned. Because three of the four volunteers who had received the molecule presented with adverse events, a genetic susceptibility to these effects is improbable. The atypical distribution of the brain lesions; the widespread, bilateral, and symmetric pattern of the injury; and the drug-accumulation–dependent toxic effects suggest direct toxicity of BIA 10-2474.5 Nevertheless, the precise mechanism of this toxic cerebral syndrome is unknown. The distribution of the brain lesions does not exactly match the location of the endocannabinoid system.6 Endocannabinoid receptors and FAAHs are highly expressed in the hippocampi but not in the pons. Moreover, severe toxic effects in the central nervous system as a result of an increased level of endocannabinoids have not been reported previously; this suggests the possibility of an offtarget effect of the drug, owing to the low specificity of BIA 10-2474 for FAAH, or an effect of a metabolite.4 These unanticipated severe adverse events were caused by the drug and reflect the complexities of clinical drug research. n engl j med 375;18 nejm.org November 3, 2016 Acute Neurologic Disorder from an FA AH Inhibitor Disclosure forms provided by the authors are available with the full text of this article at NEJM.org. We thank Ms. Sara Calmanti for her help in writing the first draft of this article and Ms. Elizabeth Portier for her help in References 1. Cravatt BF, Demarest K, Patricelli MP, et al. Supersensitivity to anandamide and enhanced endogenous cannabinoid signaling in mice lacking fatty acid amide hydrolase. Proc Natl Acad Sci U S A 2001; 98:9371-6. 2. Roques BP, Fournié-Zaluski MC, Wurm M. Inhibiting the breakdown of endogenous opioids and cannabinoids to alleviate pain. Nat Rev Drug Discov 2012; 11:292-310. 3. Huggins JP, Smart TS, Langman S, Taylor L, Young T. An efficient randomised, placebo-controlled clinical trial editing an earlier version of the manuscript; the family of the patient who died and the three other patients for consenting to the publication of their clinical and MRI data; and the staff at Rennes University Hospital for caring for the patients. with the irreversible fatty acid amide hydrolase-1 inhibitor PF-04457845, which modulates endocannabinoids but fails to induce effective analgesia in patients with pain due to osteoarthritis of the knee. Pain 2012;153:1837-46. 4. Report by the Temporary Specialist Scientific Committee (TSSC), “FAAH (Fatty Acid Amide Hydrolase)”, on the causes of the accident during a Phase 1 clinical trial in Rennes in January 2016. Saint-Denis, France:Agence Nationale de Sécurité du Médicament et des Produits de Santé (http://ansm.sante.fr/var/ansm_ site/storage/original/application/ 744c7c6daf96b141bc9509e2f85c227e .pdf). 5. Sharma P, Eesa M, Scott JN. Toxic and acquired metabolic encephalopathies: MRI appearance. AJR Am J Roentgenol 2009;193:879-86. 6. Hu SS, Mackie K. Distribution of the endocannabinoid system in the central nervous system. Handb Exp Pharmacol 2015;231:59-93. Copyright © 2016 Massachusetts Medical Society. n engl j med 375;18 nejm.org November 3, 2016 1725