Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
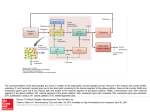
Basal ganglia Basal ganglia • Basal ganglia regulate – – – – muscle contraction muscle force multijoint movement Sequencing of movement • The output of the basal ganglia is via – Motor area of the cerebral cortex – Pendunculopontine nucleus (elicits rhythmical behaviors such as locomotor patterns) : located in the brain stem Caudate Putamen Globus pallidus Subthalamic nucleus Substantia nigra Corpus straitum straitum Caudate nucleus putamen Leniform nucleus Globus pallidus The function of caudate : cognitive, not motor The function of the ventral striatum : limbic Basal ganglia : no direct connections with lower motor neurons (1) Motor planning areas of the cerebral cortex (2) Pedunculopontine nucleus of the midbrain • Subthalmic nucleus : inferior to the thalamus and lateral to the hypothalamus • Substantia nigra : a nucleus in the midbrain named for the color of its cells Compacta (provide essential dopamine to the striatum) Reticularis • Substantia nigra reticularis and globus palidus internus : output nuclei of the basal ganglia system – Output nuclei : inhibit the motor thalamus and the pedunclopontine nucleus of the midbrain (1) Motor planning areas of the cerebral cortex • a major basal ganglia circuit connects motor and somatosensory areas of the cerebral cortex-> the putamen-> the output nuclei-> the motor thalamus-> motor areas of the cerebral cortex ; corticofugal tracts (2) Pedunculopontine nucleus of the midbrain • From the globus pallidus internus to the pedunclopontine nucleus, thence to the reticulospinal and to the vestibulospinal tracts Basal Ganglia Connections Input Portion STRIATUM (Caudate Nucleus and Putamen) Output Portion 1. PALLIDUM (Globus Pallidus) 2. SNr (Substantia Nigra, Pars Reticulata) Basal Ganglia Connections STRIATUM Afferents from 1. Cerebral Cortex [Corticostriatal Projection] 2. Thalamus [Thalamostriatal Projection] 3. SNc (Substantia Nigra, pars compacta), Ventral Tegmental Area (VTA, A10) and A8(Retrorubral Area) [Nigrostriatal Projection] 4. Dorsal Raphe Nucleus (B6, B8) [Raphestriatal Projection] 5. Amygdaloid Nuclear Complex [Amygdalostriatal Projection] Efferents to 1. Pallidum (GPi & GPe) [Striopallidal Projection] 2. SNr [Strionigral Projection] 3. SNc from striosome Afferent Connections of Basal Ganglia Input-Output Relationship of Basal Ganglia 1. striopallidal fiber 2. strionigral fiber 3. strionigral fiber from striosome to SNc 4. ventrostrioventro-pallidal fiber Basal Ganglia Connections PALLIDUM (Globus Pallidus) Afferents from 1. Striatum [Striatopallidal Projection] 2. STN <GPi & GPe> [Subthalamopallidal Projection] Efferents to 1. Thalamus (VLo, VApc, CM) <GPi> [Pallidothalamic Projection] 2. STN <GPe> [Pallidosubthalamic Projection] SNr (Substantia Nigra, Pars Reticulata) Afferents from Striatum [Striatonigral Projection] Efferents to 1. Thalamus (VLm, VAmc, MD) [Nigrothalamic Projection] 2. Brain Stem Nucleus: Tectum (Superior Colliculus) & Pedunculopontine Nucleus (PPN) Efferent Connections of Basal Ganglia Connections of the Basal Ganglia amygdaloid body Cerebral Cortex raphe STRIATUM Thalamus STN SNc Pallidum SNr habenular nucleus tectum PPN (superior colliculus) (pedunculopontine nucleus) Basal Ganglia (Main Motor Circuit) Connections Primary Motor Area (M I) Supplementary Motor Area (SMA) STRIATUM (Putamen) pyramidal tract THALAMUS (VLo, VApc, CM) LMN ansa lenticularis lenticular fasciculus PALLIDUM (GPi) Basal Ganglia (Prefronatal Complex Loop) Connections Primary Motor Area (M I) Prefrontal Association Cortex STRIATUM (Caudate Nucleus) THALAMUS SNr pyramidal tract (VLm, VAmc, MD) LMN (Substantia Nigra, pars reticulata) Basal Ganglia (Limbic Loop) Connections Orbitofrontal Cortex Anterior Cingulate Gyrus Hippocampal Formation THALAMUS (VAmc, MD) Ventral Striatum Caudate Nucleus Ventral Pallidum GPi, SNr Basal Ganglia (Oculomotor Loop) Connections Primary Motor Area (M I) Frontal Eye Field (area 8) STRIATUM (Caudate Nucleus) THALAMUS SNr pyramidal tract (VLm, VAmc, MD) LMN Tectum (Substantia Nigra, pars reticulata) Basal Ganglia and Pyramidal Tract SMA (supplementary motor area) upper motor neuron UMN pyramidal tract lower motor neuron LMN BASAL GANGLIA CIRCUIT Function of the basal ganglia • Sequencing movements and regulating muscle tone and muscle force • Select and inhibit specific motor synergies; - from putamen to the output nuclei : select synergies (direct path) - via the globus pallidus externus and subthalamic nucleus : inhibit synergies (indirect path) Pathology of the basal ganglia • Movement disorders - hypokinetic disorders parkinson’s disease - hyperkinetic disorders Huntington’s disease Dystonia Subtype of cerebral palsy • Difference in abnormal movements are due to dysfunction in specific parts of the basal gangliathalamocortical motor circuit and in the basal ganglia-pedunculopontine nucleus • The basal ganglia inhibit the motor thalamus and the pedunculopontine Excessive inhibition : hypokinetic disorder Inadequate inhibition : hyperkinetic disorders Parkinson’s disease: • Muscular rigidity Shuffling gait Drooping posture Rhythmical muscular tremors Masklike facial expression Parkinson’s disease interferes with both voluntary and automatic movements • Pathology : the cause of cell death is unknown - the death of dopamine-producing cells in the substantia nigra compacta and acetylcholineproducing cells in the pedunculopontine nucleus • The loss of dopamine in the basal ganglia direct pathway : reduces activity in the motor areas of the cerebral cortex, decreasing voluntary movements • The loss of pedunculopontine cells, combined with increased inhibition of the pedunculopontine nucleus : disinhibits the reticulospinal and vestibulospinal tracts, producing excessive contraction of postural muscles • People with parkinson’s disease : difficulty coming to standing from sitting, flexed posture, shuffling of the feet, decreased or absent arm swing Signs of parkinson’s disease • Rigidity : increased resistance to movement in all muscles; causes active muscle contraction, directly • Hypokinesia : decreased ranges of active motion and in the lack of automatic movements, including facial expression and normal arm swing during walking, decreased ability to control the force output of muscles • Resting tremor : pill-rolling tremor; tremor is prominent when the hand is at rest and diminishes during voluntary movement • Freezing during movement : when their movements abruptly cease (interrupts gait) • Visuoperceptive impairments : deficit in using visual information to guide movements (ex: a walker) • Postural instability : secondary to the extreme stiffness of postural flexor and extensor. • Parkinson’s dementia : – Autonomic dysfunction – Interfere with the ability to plan, to maintain goal orientation, and to make decision. • Dopamine (L-dopa) : initially effective in reducing signs of the disease • However, tolerance to L-dopa, side effects (hallucinations, delusions, psychosis, dyskinesia) and progression of the disease with involvement of other cells • Disknesia : involuntary movements - chorea: brisk, jerky movements - dystonia : involuntary sustained postures or repetitive movements • Surgical procedure • Physical and occupational therapy : improve movement and functional abilities ; moderate level of activity parkinsonism • Collective name for disorders that cause signs similar to parkinson’s disease • disorders that cause the signs seen in parkinson’s disease and encompasses disorders of toxic, infectious, or traumatic etiology • Lesions of the lentiform nucleus are associated with parkinsonism • Side effect of drugs that treat psychosis or digestive problems • Phenothiazine, thioxanthine, antiemetics and other drugs that block CNS dopamine receptor Multiple system atrophy • Multiple system atrophy(MSA) : – progressive degenerative disease affecting the basal ganglia, cerebellar, and autonomic systems and cerebral cortex – MSA is characterized by; • Parkinsonism • Cerebellar signs • Autonomic dysfunction Parkinsonism : slow movements and rigidity Cerebellar aspects : dysarthria (uncoordinated speech), truncal and gait ataxia (narrow-based) Autonomic aspects : postural hypotension, bladder and bowel incontinence, abnormal respiration, decreased sweating, tears, saliva, impotence in men A decrease in goal-oriented cognitive ability and difficulty with directing attention In men : usually impotence In women : difficulty urinating Diagnosis • Pure parkinsonism : if no autonomic or cerebellar signs are present • Pure autonomic failure : orthostatic hypotension and other autonomic signs occur without signs of basal ganglia or cerebellar involvement - affects postganglionic neurons of the sympathetic system - MSA : both the preganglionic and postganglionic neurons in the sympathetic and parasympathetic systems • In MSA : autonomic neurons : - lost from brain stem nuclei and from the spinal cord - Parkinson’s disease is the most common misdiagnosis, and one third of people with MSA die while still misdiagnosed - poor response to L-dopa, orthostatic hypotension, difficulty with urination, rapid progression of functional limitations, lou • MSA poor response to L-dopa orthostatic hypotension difficulty with urination rapid progression of functional limitations Loud breathing impotence • MSA is synonymous Olivopontocerebellar atrophy : incoordination, dysarthria, balance deficits Striatonigral degeneration : rigidity and bradykinesia Shy-Drager syndrome : autonomic dysfunction • Treatment drugs Decrease orthostatic hypotension - slow position changes avoiding prolonged standing eating smaller meals use of elastic garments avoidance of warm temperature Exercise programs to maintain strength and physiologic fitness Hyperkinetic Disorders • Abnormal involuntary movements Huntington’s disease Dystonia Some type of cerebral palsy Huntington’s disease • Autosomal dominant hereditary disorder • Causes degeneration in many areas of the brain, most prominently in the striatum and cerebral cortex • Decrease in signals from the output nuclei, resulting in disinhibition of the motor thalamus and pedunculopontine nucleus -> disinhibition of the motor thalamus and pedunculopontine nucleus -> excessive output from the motor area of the cerebral cortex • Signs : chorea, consisting of involuntary, jerky, rapid movements, dementia • Onset : 40~ 50 age • Progressive, resulting in death about 15 years after signs first appear • Prevalence : 5~10 cases per 100,000 people Dystonia • Genetic, usually nonprogressive • Movement disorders : involuntary sustained muscle contractions causing abnormal postures or twisting, repetitive movements • Focal dystonias: limited to one part of the body (writer’s cramp, musician’s cramp) ; reduced reciprocal inhibition due to decreased descending inhibition • Treatment Avoidance of heavy gripping of instruments Sensory retraining Mental rehearsal of the target movement without overt body movement Motor control Heat, cold and exercise Medications : acetylcholine, GABA, dopamine Surgical lesion of the motor thalamus or injection of botulinum toxin into the affected muscles • Segawa’s dystonia : interfere with walking and may mimic the appearance of cerebral palsy; progress slowly and can be effectively treated with medications Choreoathetotic cerebral palsy • Abnormal involuntary movements • People with choreoathetosis, a type of cerebral palsy • Chorea : abrupt, jerky movements • Athetosis : slow, writhing, purposeless movements summary • Basal ganglia disorders interfere with voluntary and automatic movements Produce involuntary movements Hypokinesia : decrease in the amount of and speed of voluntary and automatic movements (Parkinson’s disease) Hyperkinesia : abnormal excessive movement (huntington’s disease, dystonia, choreoathetotic palsy)