Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
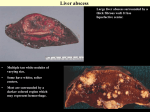
MODULE 5 – LIVER CANCER LIVER CANCER Primary Liver Cancer Secondary Liver Cancer Version 1.1 – April 2007 TP-ROW-01 for internal use only page 1 MODULE 5 – LIVER CANCER Version 1.1 – April 2007 TP-ROW-01 for internal use only page 2 MODULE 5 – LIVER CANCER Despite the fact that primary liver cancer is not quite common in the western world, some authors suggest HCC being one of the most common fatal tumours worldwide with an estimated 1 million cases occurring annually. Version 1.1 – April 2007 TP-ROW-01 for internal use only page 3 MODULE 5 – LIVER CANCER The geographical distribution of HCC varies greatly and correlates almost 100 per cent with the regional incidence rates of hepatitis B and C infections. HCC affects persons of all age groups. In Asian and African countries, the morbidity peak is reached in adolescence or between the ages of 20 and 40years, corresponding to predominantly perinatal or postnatal infections with hepatitis viruses. The HCC gender ratio between men and women is 2.5:1 up to 8:1 in countries with high incidence. In a cirrhosis free liver, however, men and women are effected by HCC at the same rate. The patient is suspected to be suffering from HCC when the subjective complains continue to deteriorate and when an increase in complains cannot be explained by the progression of cirrhosis. Occasionally, the course of HCC may be acute, resembling liver failure or liver abscess. It is widely accepted that when HCC is discovered in a symptomatic patient, the disease is usually rapidly fatal. The clinical situation deteriorates rapidly: febrile temperatures and leucocytosis as well as subicterus are observed; there are also signs of encephalopathy. An arterial murmur can often be heard on auscultation, since the tumour is mainly supplied with blood from the hepatic artery. Version 1.1 – April 2007 TP-ROW-01 for internal use only page 4 MODULE 5 – LIVER CANCER An AFP>20ng/mL in a group of patients with cirrhosis has been shown to be an independent predictor for developing HCC. With regard to imaging techniques, sonography is the method of choice in monitoring the course of risk patients, particularly in combination with AFP (alphafoetoprotein) determination. Nevertheless the sensitivity has been reported to vary from 43% to 90%. Other imaging procedures include angiography, magnetic resonance imaging and scintigraphy. The FNB is associated with the risk of tumour spreading. The nodular surface indicating liver cirrhosis (HCC and alcohol) can be seen. Tumour formation can been seen in the right lobe of liver, in parts at the margin. Left hand picture: Large-bulbous hepatocellular carcinoma due to alcohol abuse and active chronic hepatitis B with cirrhotic transformation in some places. Right hand picture: Small to medium-coarse nodular, alcoholic cirrhosis with undifferentiated, multilobular hepatocellular carcinoma and subcapsular vascularization. Version 1.1 – April 2007 TP-ROW-01 for internal use only page 5 MODULE 5 – LIVER CANCER The rule of thumb is that the bigger the tumour and the quicker it grows the shorter is the life expectancy. The prognosis is if even worse if the tumour has already spread to other organs such as the lung. The prognosis of HCC is very bad. Almost all patients die within the first year after diagnosis, some of them within only two month. Secondary liver cancer is referred to with the staging of the primary tumour. Version 1.1 – April 2007 TP-ROW-01 for internal use only page 6 MODULE 5 – LIVER CANCER By including clinical and laboratory parameters, K.Okuda introduced a classification into stages in order to improve the prognostic accuracy regarding survival time. The survival rate in the untreated course was calculated to be 11 month in stage 1, 3 month in stage 2 and 1 month in stage 3. There are a few cases of spontaneous regression reports. However, recurrence after regression has also been reported. Anorexia is a loss of appetite or lack of desire to eat. Cachexia is often seen as loss of weight and is a consequence of emaciation. Version 1.1 – April 2007 TP-ROW-01 for internal use only page 7 MODULE 5 – LIVER CANCER Liver metastasis may occur as solitary or multiple nodes and many ultimately infiltrate almost the whole liver tissue. Histology of liver metastasis is often similar to that of a primary liver tumour which makes the classification almost impossible. Carcinoid tumours: The curious name of these tumours was coined in 1907 to emphasize the benign course which they follow, although a proportion are malignant at the outset and others become so with time. The liver is the first destination of venous blood drainage from multiple intra-abdominal organs. As a result of its dual blood supply (75% from the portal vein and 25% from the hepatic artery) and histological filtering structure, the liver is a common site of metastatic deposits. Version 1.1 – April 2007 TP-ROW-01 for internal use only page 8 MODULE 5 – LIVER CANCER There has been little enthusiasm for resection and local therapy of non-portal hepatic metastasis (breast, lung, melanoma) because of the high probability of extra-hepatic disease. Only colorectal, pancreaticneuroendocrine and carcinoid tumours have a reasonable chance of having liver metastasis only because the liver is the first ‘filter’. Colorectal cancer metastasis to the liver is by far the most extensively studied and its management continues evolve. Version 1.1 – April 2007 TP-ROW-01 for internal use only page 9 MODULE 5 – LIVER CANCER Large metastases in the right hepatic lobe subsequent to breast cancer. A solitary node is found in some 10% of patients at the time of diagnosis. The metastasis often shows a central depression due to tumour necrosis caused by insufficient blood supply within the tumour (= cancer umbilicus) Pronounced liver invasion by metastases of varying size and neo-vascularization (bronchial carcinoma). Liver metastasis may ultimately infiltrate the whole liver tissue. This may result in extreme hepatomegaly with a liver size of more than 5kg. Version 1.1 – April 2007 TP-ROW-01 for internal use only page 10 MODULE 5 – LIVER CANCER In addition jaundice with advancing cachexia usually develops as the tumour continues to grow. Symptoms like ascites, thrombosis often show up at a very late stage when the liver function is already weakened. In sonography metastases from 0.5-1cm can be detected. However, this method is not able to differentiate between benign and malign disease. Version 1.1 – April 2007 TP-ROW-01 for internal use only page 11 MODULE 5 – LIVER CANCER Version 1.1 – April 2007 TP-ROW-01 for internal use only page 12 MODULE 5 – LIVER CANCER Tumours arising from neuroendocrine cells of the gastrointestinal tract and pancreas present special challenges in diagnosis and therapy. These tumours often cause symptoms from excess hormone secretion rather than from growth. Frequently slow growing, they may nonetheless be lifethreatening because of uncontrolled release of specific hormones or neurotransmitters. Version 1.1 – April 2007 TP-ROW-01 for internal use only page 13 MODULE 5 – LIVER CANCER Version 1.1 – April 2007 TP-ROW-01 for internal use only page 14